
Abstract
Purpose
To determine whether preoperative EMG severity predicts clinically meaningful recovery after adult spinal deformity surgery.
Methods
In this single-center observational cohort, prospectively collected data from 84 patients undergoing adult spinal deformity surgery were retrospectively analyzed. EMG radiculopathy severity was graded 1–3; grade 3 defined severe abnormality. 24-month ODI and VAS-leg improvement, MCID achievement, satisfaction, complications, and reoperations were compared. Regression models adjusted for baseline score, age, and fused levels.
Results
ODI improved by 16.20 points and VAS-leg by 3.38 points overall; however, only 51.2% achieved ODI MCID. Severe EMG patients had less ODI improvement (9.09 vs 17.62 points; difference, 8.53; 95% CI, 4.23–12.84) and less VAS-leg improvement (1.15 vs 3.82 points; difference, 2.67; 95% CI, 1.83–3.52). Increasing EMG severity independently predicted less improvement and higher ODI MCID failure.
Conclusion
Major adult spinal deformity surgery improved average patient-reported outcomes; however, severe preoperative EMG abnormality identified a distinct high-risk, low-benefit phenotype in whom surgery was less likely to produce clinically meaningful radicular pain relief and more likely to be followed by poor satisfaction, complications, and reoperation.
Keywords
Introduction
Adult spinal deformity (ASD) is an increasingly prevalent and resource intensive condition in aging populations, commonly presenting with chronic pain, progressive functional limitation, and impaired HRQoL. Contemporary prospective multicenter studies have shown that operative treatment can provide durable average improvements in patient-reported outcomes over mid-term follow-up.1,2 However, these aggregate gains obscure substantial patient level heterogeneity. A meaningful proportion of patients experience persistent disability, medical or surgical complications, and reoperation, particularly among older patients, those with greater comorbidity burden, and those requiring long-segment reconstruction.2–4 Thus, ASD surgery remains a clinical tradeoff between potential functional recovery and considerable biologic and surgical risk.
As a result, the field has increasingly moved beyond radiographic correction alone toward outcomes that reflect patient-perceived benefit. The minimal clinically important difference (MCID) provides a clinically interpretable threshold for determining whether change in disability, pain, or quality of life is meaningful to the patient rather than merely statistically detectable.5,6 In ASD surgery, ODI-based MCID analysis has become particularly relevant because radiographic improvement does not consistently translate into meaningful functional recovery. 7 Current decision frameworks incorporate alignment, frailty, comorbidity, baseline disability, and expected surgical invasiveness, yet they rarely include an objective measure of preoperative nerve root integrity. 8 This leaves an important unresolved question: whether the physiologic severity of radiculopathy can identify patients whose neural recovery potential is limited despite technically adequate decompression and deformity correction.
Electrodiagnostic testing may provide this missing physiologic layer. In lumbosacral radiculopathy and degenerative stenosis, EMG can demonstrate chronic neurogenic change, active denervation, multiroot involvement, and axonal injury, offering information that is distinct from static imaging alone.9–11 Nevertheless, the prognostic literature remains limited and inconsistent, largely derived from lumbar disc herniation or stenosis cohorts rather than complex ASD reconstruction.12–14 The present study therefore evaluates whether preoperative EMG severity is associated with postoperative improvement and MCID achievement after adult spinal deformity surgery. Rather than replacing radiographic assessment, EMG may provide an additional physiologic layer by characterizing the severity of radiculopathic nerve injury before reconstruction. We hypothesized that patients with severe preoperative EMG abnormalities would have smaller absolute improvements and a lower likelihood of achieving MCID in ODI and leg pain after ASD surgery.
Materials and Methods
Study design and setting
This was a single-center observational cohort study based on prospectively collected clinical data analyzed retrospectively. Consecutive patients undergoing surgery for adult spinal deformity with degenerative or degenerative dominant pathology were evaluated to determine whether preoperative lumbar electrodiagnostic severity was associated with postoperative clinical improvement and MCID achievement. The protocol was designed in accordance with STROBE recommendations.
Patient selection
Patients treated between January 2019 and December 2023 were screened. Inclusion criteria were: age ≥50 years; radiographic adult spinal deformity, defined by ≥20° coronal curvature or degenerative kyphosis or spondylolisthesis with multilevel lumbar stenosis; posterior instrumentation and fusion involving at least three motion segments; preoperative lumbar nerve conduction study performed according to the institutional protocol; and complete baseline and minimum 24- month clinical outcome data. At our institution, preoperative lumbar EMG/nerve conduction testing is routinely included in the preoperative evaluation of adult spinal deformity patients with degenerative or degenerative-dominant pathology when radicular symptoms, multilevel stenosis, neurologic complaints, or planned multilevel decompression/fusion are present. EMG was therefore not selectively ordered according to anticipated outcome, deformity severity, or surgeon preference. This institutional practice allowed EMG severity to be assessed in all eligible patients included in the primary analysis set. Exclusion criteria were prior lumbar fusion, idiopathic scoliosis without degenerative predominance, neuromuscular, syndromic, infectious, neoplastic deformity, acute traumatic fracture, peripheral neuropathy or systemic neuromuscular disease likely to confound EMG interpretation, and missing primary outcome data. Eighty-four consecutive eligible patients constituted the primary analysis set. Although the cohort included several adult spinal deformity etiologies, all included patients shared the same operative context: symptomatic adult spinal deformity requiring posterior instrumentation and fusion of at least three motion segments, with preoperative electrodiagnostic evaluation performed within the institutional protocol. Because the primary biological hypothesis concerned the prognostic relevance of radiculopathic nerve injury, a sensitivity analysis was planned in the degenerative or degenerative-dominant subgroup to assess whether the main findings persisted in the population most directly related to stenosis-associated radiculopathy.
Clinical assessment
Baseline variables included age, sex, body mass index, symptom duration, smoking status, diabetes, cardiovascular disease, osteoporosis, and other comorbidities. Clinical outcomes were recorded preoperatively and at routine postoperative follow-up visits at 3, 6, and 12 and 24-months; the 24-month visit was defined a priori as the primary endpoint. Functional disability was assessed with the Oswestry Disability Index, with higher scores indicating greater disability. 15 Pain severity was recorded separately for back and leg pain using a 10-cm visual analog scale (VAS-back and VAS-leg). Health-related quality of life was assessed using the Turkish version of the Short Form-36 (SF-36), and the Physical Component Summary (PCS) and Mental Component Summary (MCS) scores were derived from the SF-36 according to standard scoring methodology. 16 Global clinical outcome was evaluated at final follow-up using the modified MacNab criteria, with outcomes categorized as excellent, good, fair, or poor. 17
Radiographic and electrophysiological assessment
Radiographic evaluation was performed using standing anteroposterior and lateral full-length spine radiographs and preoperative lumbar MRI. Standardized research-grade ASD radiographic measurements were not consistently retrievable from the analyzable dataset. Although standing radiographs were used in routine clinical planning, Cobb angle, SVA, PI–LL mismatch, PT, SS, and LL were not available in a uniform format suitable for statistical modeling. Therefore, these parameters were not incorporated into adjusted analyses, and radiographic characterization in this study was limited to deformity pattern, number of fused levels, and MRI-based stenosis grading. Stenosis grading was based on structured MRI assessment 18
All patients underwent EMG/nerve conduction testing within 6 months before surgery. EMG studies were considered valid for analysis if they were obtained within the institutional preoperative assessment window and before the index operation. All patients underwent a final preoperative clinical evaluation after EMG acquisition, including assessment of radicular pain distribution, motor deficit, sensory deficit, and walking tolerance. Patients with clinically relevant interval neurological progression were reassessed before surgery, and repeat electrodiagnostic testing was considered when the treating team judged that the previous EMG no longer reflected the current neurological status. Thus, the EMG grade used for analysis represented the most recent available preoperative electrophysiological assessment considered clinically applicable at the time of surgery. Examinations were performed by an experienced neurophysiology specialist using a lumbar radiculopathy protocol.9,10 EMG reports were generated during routine preoperative care by an experienced neurophysiology specialist and were extracted from formal neurophysiology reports for this study. Formal blinding of the neurophysiologist to clinical or radiographic information could not be verified retrospectively. However, EMG severity grading for the study was based on predefined criteria and was completed before postoperative outcome analysis. Motor conduction studies included tibial and peroneal nerves; sensory studies included sural and superficial peroneal nerves. Needle EMG sampled bilateral L2–S1 myotomes, including representative muscles such as vastus medialis, tibialis anterior, medial gastrocnemius, gluteus medius, and lumbar paraspinal muscles. The clinical indication for EMG was to document the presence, distribution, and severity of lumbosacral radiculopathy before multilevel reconstruction and to help distinguish root-level dysfunction from peripheral neuropathic or non-spinal causes of lower-extremity symptoms. EMG results were not used to exclude patients from surgery in this study; rather, they were analyzed retrospectively as a prognostic exposure.
EMG severity was classified using a structured, hierarchical 0–3 global radiculopathy severity scale derived from established electrodiagnostic principles for lumbosacral radiculopathy. The grading incorporated chronic neurogenic motor unit changes, active denervation potentials, the number of abnormal limb muscles, the number of involved roots/myotomes, and paraspinal denervation. Grade 0 indicated no electrodiagnostic evidence of lumbosacral radiculopathy. Grade 1 represented mild radiculopathy, defined as limited chronic neurogenic changes confined to a single root distribution without active limb-muscle denervation. Grade 2 represented moderate radiculopathy, characterized by chronic neurogenic changes involving multiple muscles and/or adjacent root distributions, with absent or only limited active denervation. Grade 3 represented severe radiculopathy and required multilevel or multiroot involvement with widespread chronic neurogenic changes and prominent active denervation, including fibrillation potentials or positive sharp waves in more than one limb muscle and/or associated paraspinal denervation. The classification was hierarchical rather than purely additive: multiroot involvement, active denervation, or paraspinal abnormalities increased severity only when they occurred in a distribution compatible with lumbosacral radiculopathy, and multiroot involvement alone was not sufficient for grade 3 classification unless accompanied by widespread chronic neurogenic change and prominent active denervation. 19 For analysis, severe EMG abnormality was defined as grade 3 versus grades 0–2, while active denervation, chronic neurogenic change, paraspinal denervation, and number of involved roots were recorded separately for descriptive and exploratory analyses. 19
Outcome measures
The primary continuous outcome was 24-month ODI improvement, calculated as preoperative ODI minus 24-month ODI; positive values therefore represented improvement. The primary binary outcome was achievement of ODI MCID, defined as ≥10-point improvement.5–7 Secondary outcomes included VAS-back and VAS-leg improvement, VAS-leg MCID response using a prespecified ≥2-point threshold, SF-36 PCS/MCS change, MacNab satisfaction category, any complication, major complication, and reoperation.5,6 Surgical variables included operative time, estimated blood loss, osteotomy, interbody fusion, number of fused segments, and intraoperative complications. Complications were recorded through the 24-month follow-up period. Any complication included perioperative or postoperative medical or surgical adverse events documented in the clinical record. Major complications were defined as events requiring invasive intervention, reoperation, prolonged hospitalization, readmission, new or worsened neurologic deficit, deep infection, thromboembolic event, cardiopulmonary event requiring treatment escalation, or any event resulting in persistent morbidity. Reoperation was defined as any unplanned return to the operating room related to the index deformity procedure during follow-up.
Observer reliability
Clinical scores were patient-reported and recorded prospectively using standardized forms. EMG interpretations were extracted from formal neurophysiology reports. Radiographic and MRI parameters were abstracted from institutional imaging records. Formal interobserver reliability testing was not performed; this limitation was prespecified and considered in interpretation.
Statistical analysis
Continuous variables were summarized as mean ± standard deviation, according to distribution. Categorical variables were summarized as n (%). Normality was assessed with the Shapiro–Wilk test and distributional inspection. Paired preoperative–postoperative changes were analyzed using paired t-tests or Wilcoxon signed-rank tests, as appropriate. Between-group comparisons according to EMG severity were performed using Welch’s t-test or Mann–Whitney U test for continuous variables and Fisher’s exact test for categorical variables. Mean differences, 95% confidence intervals, standardized effect sizes, risk differences, odds ratios, and MCID responder proportions were reported when applicable.
Multivariable linear regression was used for ODI and VAS-leg improvement. Logistic regression was used for MCID failure. Models were kept parsimonious to reduce overfitting and adjusted for clinically relevant covariates, including baseline score, age, and number of fused levels. Variables with complete absence of data were excluded; otherwise, complete-case analysis was used. Statistical significance was set at two-sided p < 0.05. Analyses were performed using SPSS/R-equivalent statistical software.
Ethics statement
The study was approved by the local institutional ethics committee. All patients provided written informed consent for surgery and use of anonymized clinical data for research. Data were deidentified before analysis, and no study-specific intervention was performed.
Results
Patient characteristics and cohort flow
Baseline characteristics of the study cohort according to preoperative EMG severity.
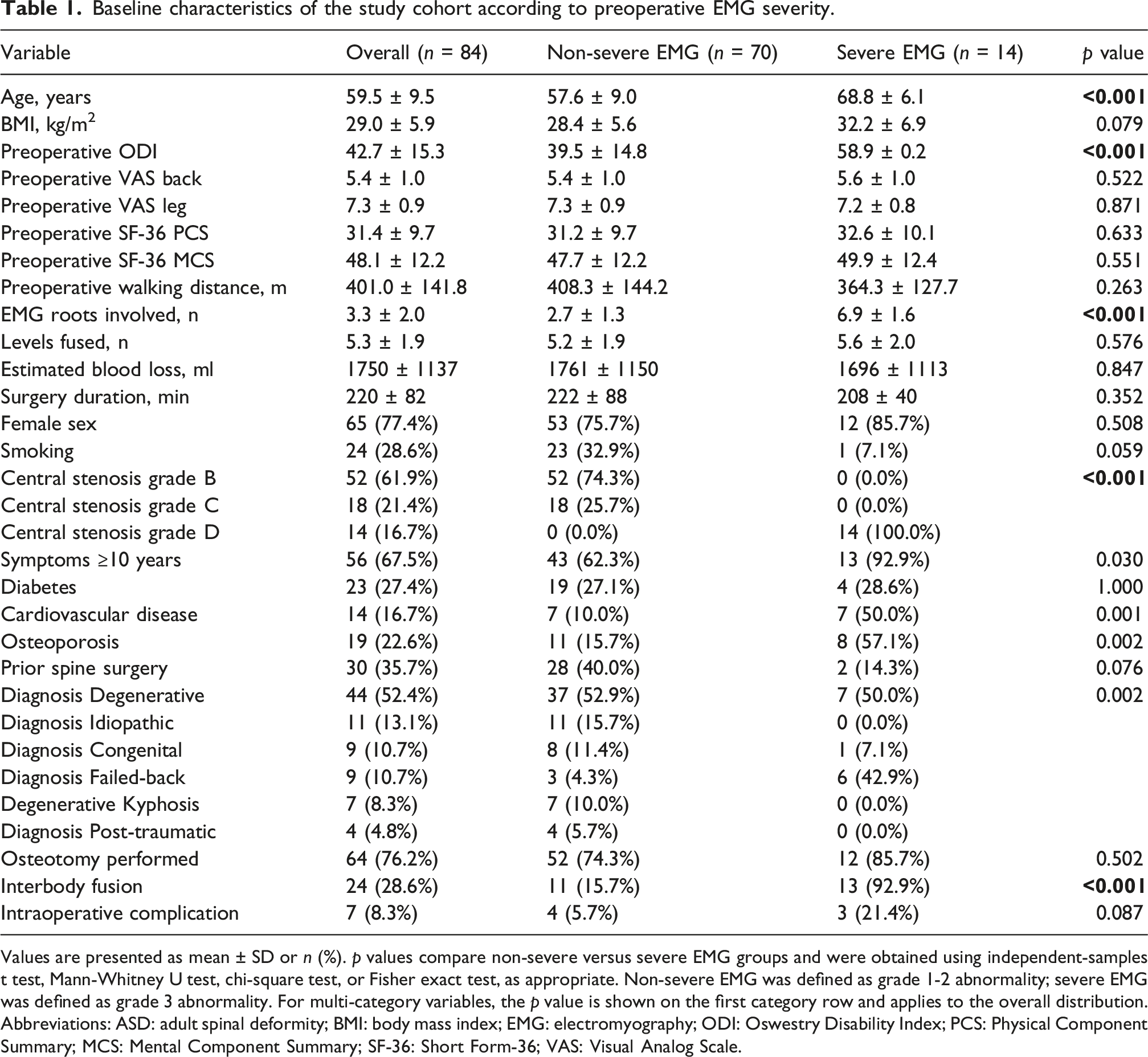
Values are presented as mean ± SD or n (%). p values compare non-severe versus severe EMG groups and were obtained using independent-samples t test, Mann-Whitney U test, chi-square test, or Fisher exact test, as appropriate. Non-severe EMG was defined as grade 1-2 abnormality; severe EMG was defined as grade 3 abnormality. For multi-category variables, the p value is shown on the first category row and applies to the overall distribution. Abbreviations: ASD: adult spinal deformity; BMI: body mass index; EMG: electromyography; ODI: Oswestry Disability Index; PCS: Physical Component Summary; MCS: Mental Component Summary; SF-36: Short Form-36; VAS: Visual Analog Scale.
Baseline findings according to EMG severity
Patients with severe EMG abnormalities were older than those with non-severe EMG findings (68.8 ± 6.1 vs 57.6 ± 9.0 years, p < 0.001) and had greater baseline disability (preoperative ODI: 58.9 ± 0.2 vs 39.5 ± 14.8, p < 0.001). Stenosis grade was closely associated with EMG severity: all patients in the severe EMG group had grade D central stenosis, whereas the non-severe group included only grade B or C stenosis. Cardiovascular disease (50.0% vs 10.0%, p = 0.001) and osteoporosis (57.1% vs 15.7%, p = 0.002) were more frequent in the severe EMG group. Interbody fusion was also more common among patients with severe EMG abnormalities (92.9% vs 15.7%, p < 0.001). Neurophysiologically, all severe EMG patients had active denervation and chronic neurogenic changes. The number of involved roots was higher in the severe EMG group (6.9 ± 1.6 vs 2.7 ± 1.3). These baseline differences indicate that severe EMG abnormality clustered with older age, greater baseline disability, higher comorbidity burden, and greater surgical complexity; therefore, these variables were considered potential confounders rather than simple descriptive differences.
Primary outcome and overall clinical improvement
Overall preoperative to 24-month clinical outcomes in the full cohort.
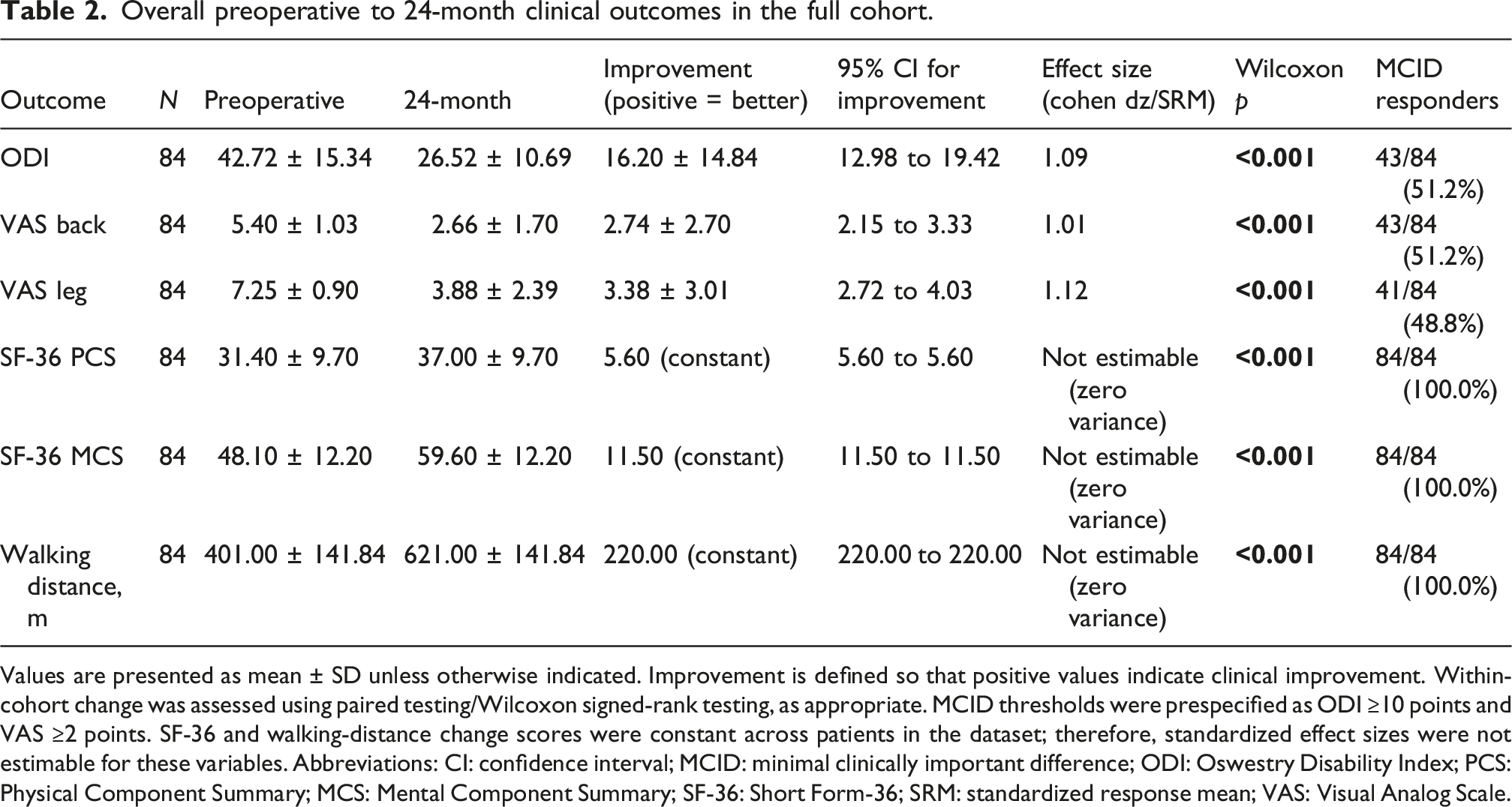
Values are presented as mean ± SD unless otherwise indicated. Improvement is defined so that positive values indicate clinical improvement. Within-cohort change was assessed using paired testing/Wilcoxon signed-rank testing, as appropriate. MCID thresholds were prespecified as ODI ≥10 points and VAS ≥2 points. SF-36 and walking-distance change scores were constant across patients in the dataset; therefore, standardized effect sizes were not estimable for these variables. Abbreviations: CI: confidence interval; MCID: minimal clinically important difference; ODI: Oswestry Disability Index; PCS: Physical Component Summary; MCS: Mental Component Summary; SF-36: Short Form-36; SRM: standardized response mean; VAS: Visual Analog Scale.
VAS-back improved from 5.40 ± 1.03 to 2.66 ± 1.70, with a mean improvement of 2.74 points (95% CI, 2.15 to 3.33; Cohen dz = 1.01; p < 0.001). VAS-back MCID was achieved in 43 patients (51.2%). VAS-leg improved from 7.25 ± 0.90 to 3.88 ± 2.39, with a mean improvement of 3.38 points
Outcomes stratified by EMG severity
Twenty-four month clinical improvement stratified by preoperative EMG severity.
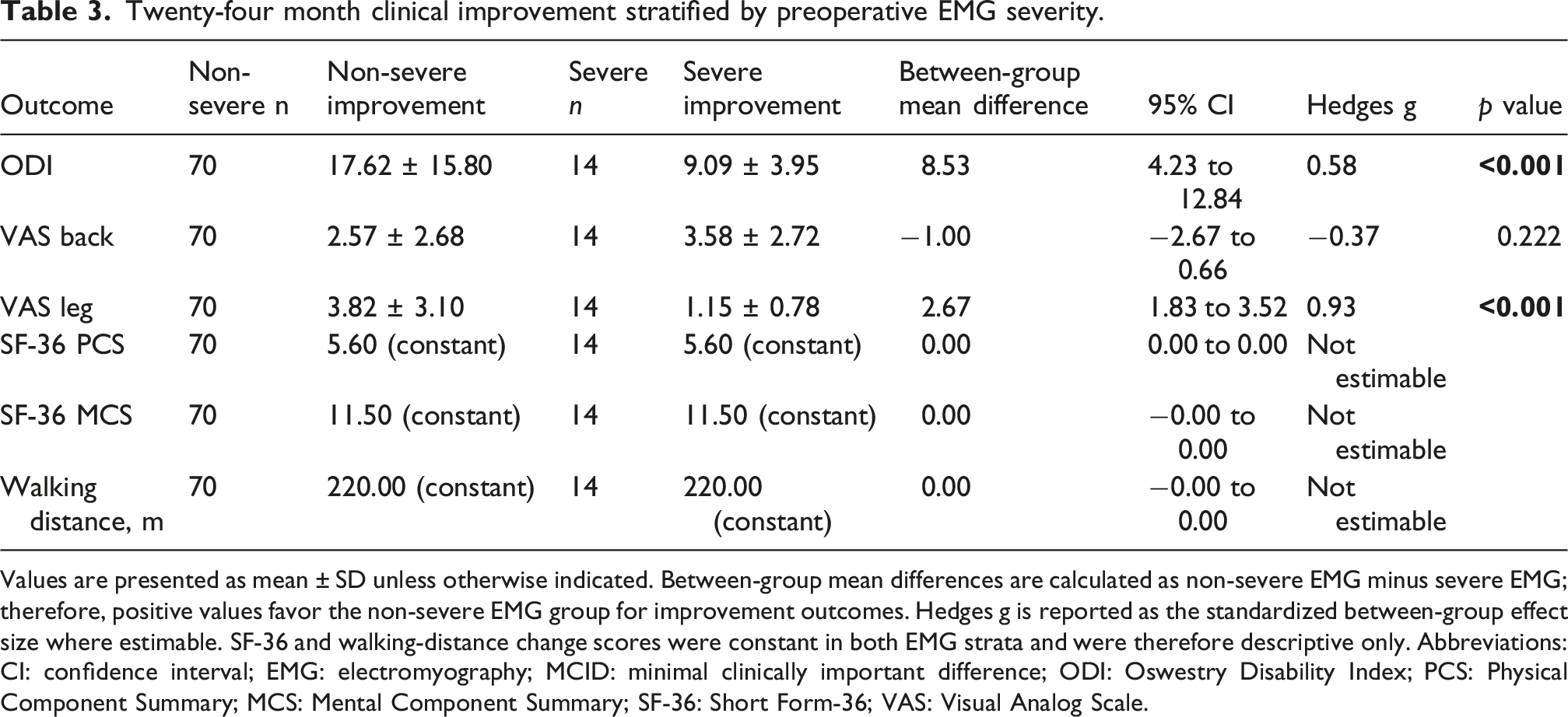
Values are presented as mean ± SD unless otherwise indicated. Between-group mean differences are calculated as non-severe EMG minus severe EMG; therefore, positive values favor the non-severe EMG group for improvement outcomes. Hedges g is reported as the standardized between-group effect size where estimable. SF-36 and walking-distance change scores were constant in both EMG strata and were therefore descriptive only. Abbreviations: CI: confidence interval; EMG: electromyography; MCID: minimal clinically important difference; ODI: Oswestry Disability Index; PCS: Physical Component Summary; MCS: Mental Component Summary; SF-36: Short Form-36; VAS: Visual Analog Scale.
The largest separation was observed for radicular leg pain. VAS-leg improvement was 3.82 ± 3.10 points in the non-severe EMG group and 1.15 ± 0.78 points in the severe EMG group. The between-group difference was 2.67 points (95% CI, 1.83 to 3.52; p < 0.001), with a large effect size
SF-36 PCS increased from 31.4 ± 9.7 to 37.0 ± 9.7 and SF-36 MCS from 48.1 ± 12.2 to 59.6 ± 12.2. The observed changes were +5.6 and +11.5 points, respectively, in both EMG groups. Source-data review confirmed that SF-36 change scores showed no between-patient variability in the available dataset. Therefore, SF-36 variables were summarized descriptively only, and inferential comparisons, variance-based confidence intervals, standardized effect sizes, and EMG-stratified prognostic interpretation were not performed.
MCID responder analysis
MCID responder status, satisfaction, complications, and reoperation according to EMG severity.
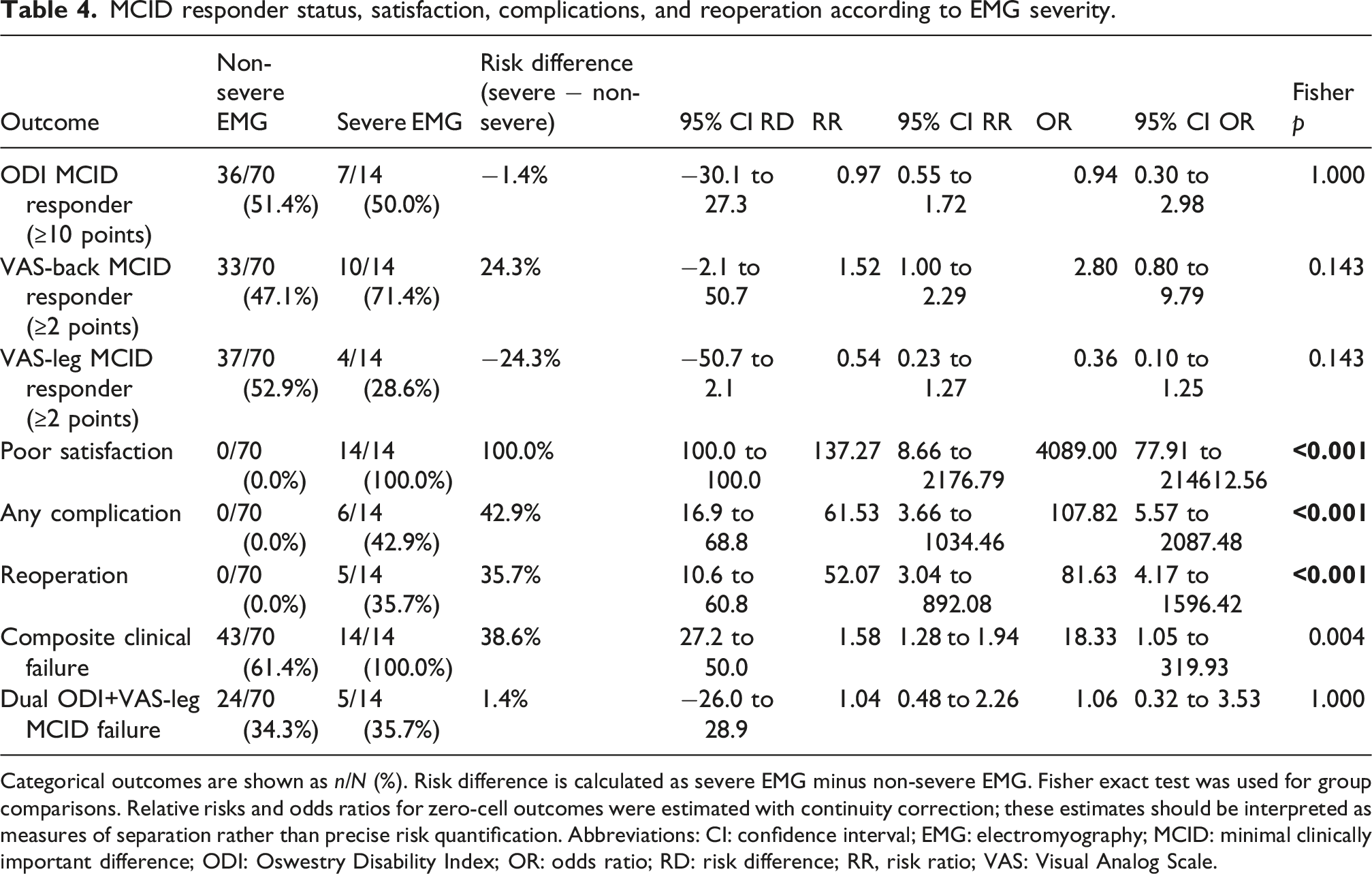
Categorical outcomes are shown as n/N (%). Risk difference is calculated as severe EMG minus non-severe EMG. Fisher exact test was used for group comparisons. Relative risks and odds ratios for zero-cell outcomes were estimated with continuity correction; these estimates should be interpreted as measures of separation rather than precise risk quantification. Abbreviations: CI: confidence interval; EMG: electromyography; MCID: minimal clinically important difference; ODI: Oswestry Disability Index; OR: odds ratio; RD: risk difference; RR, risk ratio; VAS: Visual Analog Scale.
Complications, reoperations, and satisfaction
Parsimonious adjusted multivariable models for 24-month outcomes.
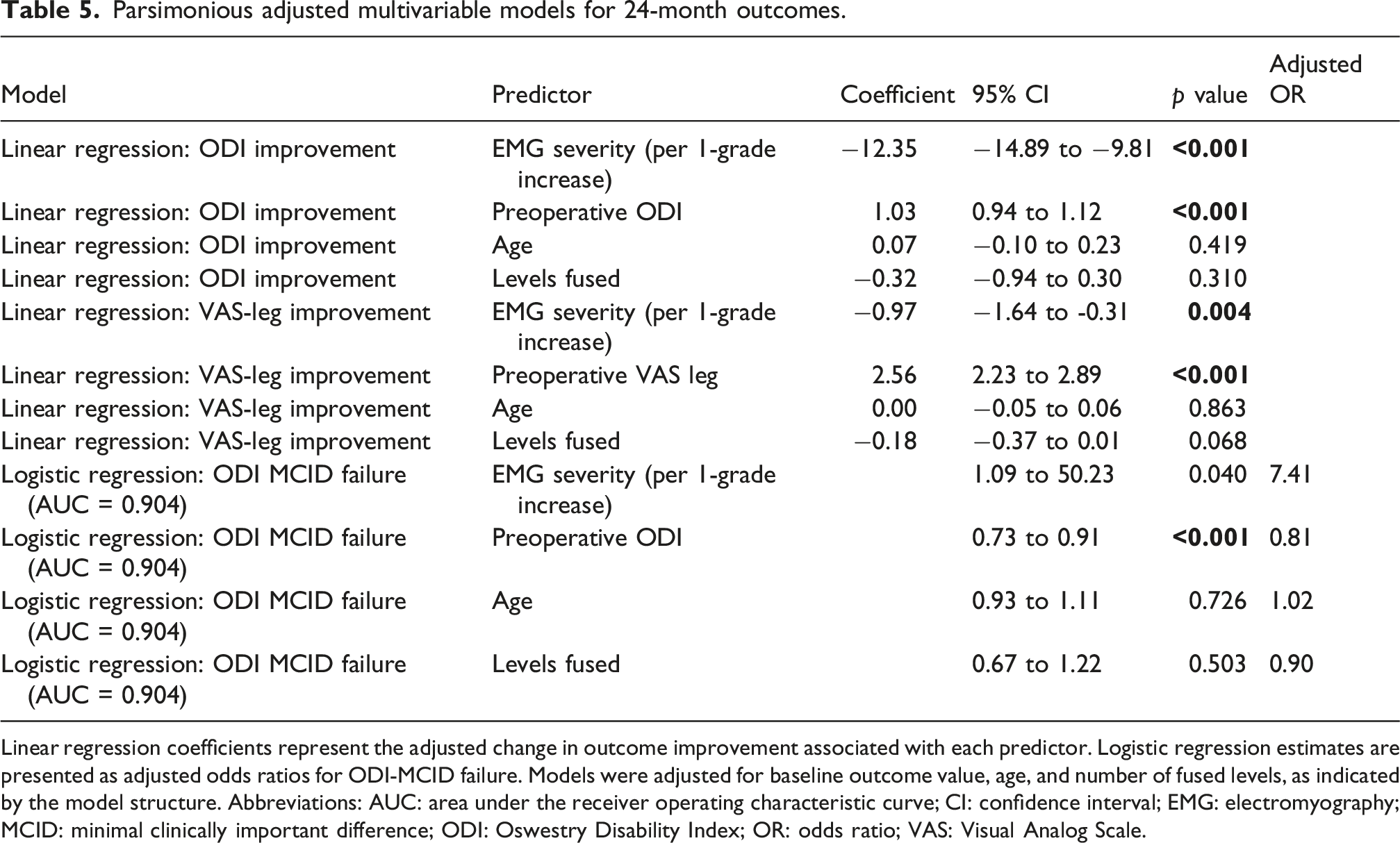
Linear regression coefficients represent the adjusted change in outcome improvement associated with each predictor. Logistic regression estimates are presented as adjusted odds ratios for ODI-MCID failure. Models were adjusted for baseline outcome value, age, and number of fused levels, as indicated by the model structure. Abbreviations: AUC: area under the receiver operating characteristic curve; CI: confidence interval; EMG: electromyography; MCID: minimal clinically important difference; ODI: Oswestry Disability Index; OR: odds ratio; VAS: Visual Analog Scale.
Regression and sensitivity analyses
In adjusted linear regression, each 1-grade increase in EMG severity was associated with 12.35 points less ODI change
In the degenerative-only subgroup (n=44), severe EMG remained associated with reduced VAS-leg improvement (0.94 ± 0.58 vs 4.38 ± 3.04 points; between-group difference, 3.44 points; 95% CI, 2.34 to 4.54; p < 0.001; Hedges g=1.20). VAS-leg MCID was achieved in 1 of 7 severe EMG patients (14.3%) and 23 of 37 non-severe EMG patients (62.2%) (p = 0.035). Poor satisfaction (7/7 vs 0/37, p < 0.001) and reoperation (3/7 vs 0/37, p=0.003) remained concentrated in the severe EMG group.
Discussion
The principal finding of this study was that severe preoperative EMG abnormalities identified a distinct lower-recovery, higher-risk phenotype among patients undergoing adult spinal deformity surgery. Although the cohort improved on average across disability and pain measures, patients with grade 3 EMG abnormalities had smaller functional gains, markedly less radicular pain relief, uniformly poor satisfaction, and a disproportionate burden of complications and reoperations. Importantly, EMG severity remained associated with reduced ODI and VAS-leg improvement after adjustment for baseline scores, age, and number of fused levels. These findings add a physiologic dimension to ASD risk stratification, complementing the current emphasis on alignment, frailty, comorbidity, and surgical complexity.
At the cohort level, surgery produced clinically relevant average improvement. ODI improved by 16.20 points, with a large paired effect size, and both VAS-back and VAS-leg improved significantly at 24-months. These results are broadly consistent with contemporary ASD literature showing durable improvement in patient-reported outcomes after operative treatment.1,20–22 However, the patient-level response was less uniform. Only 51.2% of patients achieved ODI MCID, and 48.8% achieved VAS-leg MCID. This distinction is central: statistically significant mean improvement does not ensure that individual patients experience a change large enough to matter clinically. The MCID framework is particularly useful in this setting because it exposes the gap between average surgical efficacy and patient-level benefit.5,7,23
The most clinically relevant signal emerged when outcomes were stratified by EMG severity. Severe EMG patients improved by only 9.09 ODI points on average, below the conventional 10-point ODI MCID threshold, whereas non-severe EMG patients improved by 17.62 points. The between-group difference was 8.53 points, with a moderate effect size. The separation was even stronger for radicular leg pain: VAS-leg improvement was 1.15 points in the severe EMG group versus 3.82 points in the non-severe group, a 2.67-point difference with a large effect size. This pattern suggests that EMG severity was most informative for outcomes biologically linked to nerve-root recovery, rather than for broad functional disability alone. Active denervation, chronic neurogenic change, and multiroot involvement may therefore represent a reduced neural recovery reserve rather than a simple diagnostic confirmation of radiculopathy.
These findings help reconcile prior EMG literature, which has been mixed. Earlier studies in lumbar disc herniation and sciatica reported limited or inconsistent prognostic value for EMG, often treating electrodiagnostic findings as positive or negative rather than as a severity spectrum.12,24,25 Lee, found that electrodiagnostic testing could provide clinically useful information in lumbosacral disc herniation or stenosis, while other studies emphasized limitations of electrodiagnosis as an isolated predictor.14,26,27 Our study differs in two respects. First, it evaluated a surgically complex ASD population rather than isolated disc herniation or simple stenosis. Second, EMG was analyzed by severity, including active denervation, chronic neurogenic change, and root burden. The present data therefore do not imply that any abnormal EMG predicts poor outcome; rather, they suggest that severe, diffuse, active radiculopathic injury may identify a subgroup with less reversible neural symptoms.
The relationship between structural stenosis and electrophysiologic injury deserves particular caution. All patients in the severe EMG group had high grade stenosis, indicating substantial overlap between advanced anatomic compression and advanced physiologic nerve injury. This prevents any claim that EMG severity was fully independent of stenosis severity. Instead, the combined phenotype may be the clinically meaningful construct: severe central stenosis accompanied by active denervation, chronic neurogenic change, and multiroot involvement. Chang and Park reported electrodiagnostic abnormalities in moderate-to-severe lumbar central stenosis, and recent work has linked redundant nerve-roots with ongoing denervation in lumbar stenosis.28,29 Our findings are consistent with the concept that long-standing or severe compression may progress from an anatomic problem to a physiologic nerve-injury state. In such patients, decompression and alignment correction may relieve mechanical compression but may not fully reverse established axonal injury.
The predictors of non-response in this cohort were not limited to EMG. Patients with severe EMG abnormalities were older, more disabled at baseline, had more cardiovascular disease and osteoporosis, had more involved roots, and underwent more frequent interbody fusion. These differences suggest that severe EMG was part of a broader high-burden clinical phenotype. Nonetheless, adjusted models showed that increasing EMG severity remained associated with less ODI improvement, less VAS-leg improvement, and higher odds of ODI MCID failure. These models should be interpreted with restraint because the severe-EMG subgroup was small and the number of events limited; overfitting remains possible despite parsimonious adjustment. Baseline disability also influences MCID interpretation, because patients with lower baseline ODI may have less room to achieve a 10-point improvement.5,30,31 ODI and VAS are further influenced by non-neurologic pain generators, including axial imbalance, facet degeneration, muscular fatigue, and psychosocial factors.22,32–35 These issues may explain why EMG severity discriminated VAS-leg improvement more clearly than ODI MCID.
The clinical implication is not that severe EMG should be considered a contraindication to ASD surgery. Rather, it should recalibrate counseling and surgical planning. In a patient with grade D stenosis, active denervation, chronic neurogenic change, and multiroot EMG involvement, the surgeon should be cautious about promising meaningful radicular pain relief even when decompression and deformity correction are technically appropriate. These patients may require more explicit expectation management, optimization of bone and medical risk, and careful discussion of complication and reoperation risk. The finding that poor satisfaction, complications, and reoperations were concentrated in the severe EMG group underscores the importance of presenting risk and expected benefit together. EMG may therefore have value not only as a diagnostic adjunct but also as a preoperative counseling tool in selected ASD candidates.
Several strengths support the relevance of these findings. The study incorporated objective preoperative electrodiagnostic stratification in all analyzed patients, treated EMG as a severity construct rather than a binary test, and evaluated both continuous change and MCID response. Outcomes included disability, axial and radicular pain, satisfaction, complications, and reoperation, allowing the clinical signal to be assessed from multiple perspectives. Effect sizes and confidence intervals were reported, and adjusted models accounted for baseline score, age, and fusion levels. The degenerative-only sensitivity analysis supported the main finding, particularly for VAS-leg improvement and reoperation, suggesting that the signal was not solely attributable to etiologic heterogeneity.
The limitations are equally important. The study was observational and retrospective in analysis, so causality cannot be inferred. Although EMG was routinely obtained within the institutional preoperative pathway and was not selectively ordered based on expected surgical outcome, the study remains subject to selection bias because it includes only patients who proceeded to surgery at a single center. Thus, the findings should be interpreted as applicable to a surgically treated ASD population rather than to all patients presenting with adult spinal deformity. The severe-EMG subgroup was small, which limits precision and increases uncertainty around logistic regression estimates. Because standard deformity parameters, including Cobb angle, SVA, PI–LL mismatch, PT, and SS, were not available in the dataset, the present study cannot determine whether EMG severity is independent of, or superior to, deformity magnitude. Therefore, our findings should be interpreted as evidence that severe EMG abnormality is associated with poorer clinical recovery within this cohort, not as proof that electrophysiologic severity outweighs radiographic deformity. Future studies should integrate standardized EMG grading with complete spinopelvic measurements to determine the incremental prognostic value of EMG beyond established ASD radiographic modifiers. SF-36 change scores showed no patient-to-patient variability in the available dataset, preventing meaningful discriminatory analysis by EMG severity. Finally, there was no postoperative EMG follow-up, so the study cannot determine whether persistent symptoms reflected irreversible denervation, incomplete decompression, recurrent stenosis, or other pain mechanisms. These limitations do not negate the observed association between severe EMG abnormality and poorer recovery; however, they require that the findings be viewed as hypothesis-generating and externally validated before EMG-based risk stratification is adopted as a formal decision rule in ASD surgery.
Conclusion
Severe preoperative EMG abnormality was associated with lower functional recovery, substantially less radicular pain improvement, poor satisfaction, and higher complication and reoperation rates after ASD surgery. The findings support the concept of a high-risk phenotype in which severe stenosis and advanced electrophysiologic nerve injury coexist. EMG severity should not be viewed as a stand-alone decision rule, but it may provide clinically meaningful physiologic information that complements imaging, baseline disability, comorbidity, and surgical complexity in preoperative risk stratification.
Footnotes
Ethical considerations
The study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the local institutional ethics committee (Ethics No. 3/6; 2026-91; 05.02.2026).
Consent to participate
All patients were preoperatively informed about the nature and scope of the surgical procedure, and written informed consent was obtained. The surgical consent form included a dedicated section allowing the anonymized use of patient data for academic research purposes, which was explicitly reviewed and approved by the aforementioned ethics committee.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and analyzed during the current study are available from the corresponding author by reasonable request.