
Abstract
Background
The impact of screw trajectory on the stability of internal fixation devices has been widely investigated. Previous studies indicate that ventrally directed blade insertion may compromise fixation stability and exacerbate femoral head varus in proximal femoral nail anti-rotation (PFNA) models of unstable intertrochanteric fractures with combined medial and lateral wall defects (AO/OTA 31-A2.3). According to the AO/OTA classification, the unstable fracture type involving an isolated lateral wall defect (AO/OTA 31-A2.2) is also commonly encountered in clinical practice. Preservation of medial support has been suggested to mitigate instability-related complications; however, whether such preservation can counteract the adverse biomechanical effects of ventral blade insertion remains insufficiently explored in the existing literature.
Methods
In the clinical component, a series of patients with A2.2-type unstable intertrochanteric fractures (isolated lateral wall defect) treated with PFNA fixation were enrolled. The influence of blade trajectory on femoral head varus at nearly 6 months postoperatively was evaluated using both comparative and regression analyses. Additionally, the biomechanical consequences of blade orientation were assessed using a simulated A2.2 unstable fracture model.
Results
Consistent trends were observed across clinical and biomechanical analyses. Specifically, no significant difference in femoral head varus angle was detected between ventral and dorsal blade orientations (Ventral blade: 3.86±4.14°; Dorsal blade: 3.14±5.13°, p=0.565). Blade trajectory was not identified as an independent predictor of varus severity in this patient cohort with isolated lateral wall defects (p=0.565). Biomechanically, variations in blade direction resulted in only minimal differences in stress distribution and displacement of both the blade and femoral head under compressive and physiological loading conditions.
Conclusions
The preservation of medial support appears to mitigate the detrimental effect of ventral blade insertion on fixation stability in patients with PFNA-treated intertrochanteric fractures. This study substantiates, from a novel perspective, the biomechanical importance of medial support in maintaining stable fixation.
Keywords
Introduction
The incidence of osteoporosis has progressively increased, 1 leading to a rise in low-energy traumatic fractures. 2 Among these, intertrochanteric fractures are a common type. 3 The proximal femoral nail anti-rotation (PFNA) is the most widely used device for fixation of these fractures. 4 Nonetheless, postoperative complications following PFNA implantation may adversely affect patient recovery. 5 Among them, varus deformity of the femoral head can significantly impair hip function restoration. 6 The underlying mechanisms of this complication have been extensively studied, with poor fixation stability and stress concentration at the bone–implant interface identified as key contributors to femoral head varus. 7 The influence of screw trajectory on fixation stability and the local biomechanical environment has been well documented. 8 In the PFNA procedure, the trajectory of the anti-rotation blade is widely adjustable. To evaluate the effect of blade trajectory changes on fixation stability and the incidence of femoral head varus, our previous study was conducted. The results indicated that an inferior blade trajectory was associated with interfacial stress concentration, poor fixation stability, and more severe femoral head varus in patients with unstable fractures involving combined medial and lateral wall defects. 9
As mentioned above, both the medial and lateral walls play a predominant role in achieving fixation stability after PFNA operation. In particular, the biomechanical significance of medial support (bony structures within the femoral calcar region) has been widely investigated. 10 Specifically, the medial wall serves as a primary structure for compressive load transfer. 11 Consequently, enhancing medial support may significantly improve fixation stability in osteoporotic bone after fracture fixation surgery. 3 To investigate whether the integrity of the medial wall can effectively eliminate the adverse effects of blade direction changes, a clinical evidence-based biomechanical study was conducted using both patient data and numerical models of AO/OTA 31-A2.2 type fractures (i.e., with lateral wall defect). By evaluating fixation stability in models with lateral wall defects while the medial wall remains intact, the potential confounding effect of lateral wall integrity as a variable can be effectively eliminated, allowing for an independent assessment of the biomechanical significance of medial support. 12 The comparison between this study and our previous work, investigating a single topic across different fracture types with and without medial support, can serve as a reference for deepening our understanding of the proximal femoral biomechanical environment as influenced by this factor.
Material and methods
Clinical review
Patient collection and radiographic measurement
The ethics committee of our hospital reviewed and approved the study protocol (2024gxry01). The inclusion criteria were as follows: (1) patients with an acute AO/OTA 31-A2.2 intertrochanteric fracture (defined as a lateral wall thickness < 20.5 mm 12 with an intact medial wall); (2) treatment with PFNA fixation between January 2019 and December 2023; (3) no history of prior surgical treatment for any fracture. Fracture type was classified on preoperative anteroposterior radiographs by two experienced orthopedic surgeons; all diagnoses of A2.2 fractures were confirmed on radiographs obtained immediately after trauma. The primary objective of this study was to investigate whether isolated lateral wall defects with an intact medial wall would lead to a significantly increased risk of hip varus in patients with a more ventral anti-rotation blade trajectory, and the 31-A2.2 subtype was deliberately chosen because it is fully consistent with this experimental design. The exclusion criteria were: stable intertrochanteric fractures, fractures with medial wall damage, subtrochanteric fractures, pathological fractures, previous hip fracture surgery, revision surgery due to secondary trauma nearly 6 months postoperatively, loss to follow-up, and death during the follow-up period. Demographic parameters, including age, sex, and body mass index (BMI), were recorded from their medical records. 13
Only PFNA fixation without any additional fixation procedures was used in this case series.
10
The direction of blade insertion was determined on immediate postoperative lateral radiographs and categorized relative to the central axis of the femoral neck as either ventral or dorsal. If the axis of the anti-rotation blade was inclined more ventrally than the femoral neck axis, the blade was considered ventrally placed; otherwise, it was considered dorsally placed. In PFNA fixation operation, the anti-rotation blade can only be placed in either a ventral or a dorsal direction within the femoral head, as it is difficult to achieve a trajectory that is strictly parallel to the femoral neck axis. Therefore, the ventral and dorsal groups were designed as direct comparator groups, each serving as the control for the other. Additionally, femoral head varus was evaluated by calculating the femoral neck-shaft angle on both immediate postoperative and six-month follow-up anteroposterior radiographs. 7
Statistical analyses
We conducted statistical analyses using SPSS version 26.0. To assess the potential impact of changes in blade insertional direction on the risk of femoral head varus, we performed significant difference computations and regression analyses separately in this study. Prior to these procedures, both inter- and intra-observer repeatability regarding the assessment of blade direction and femoral head varus angles were evaluated by calculating kappa coefficients and intraclass correlation coefficients (ICC) from a sample of 10 randomly selected patients within the current case series. 15 Subsequently, a normality test for the femoral head varus angle was conducted. Given that the varus angle values were normally distributed, a Student's t-test was employed to compare significant differences in femoral head varus angles between patients with ventral versus dorsal blade insertional directions. 16 A p-value < 0.05 was considered indicative of a significant difference. 17
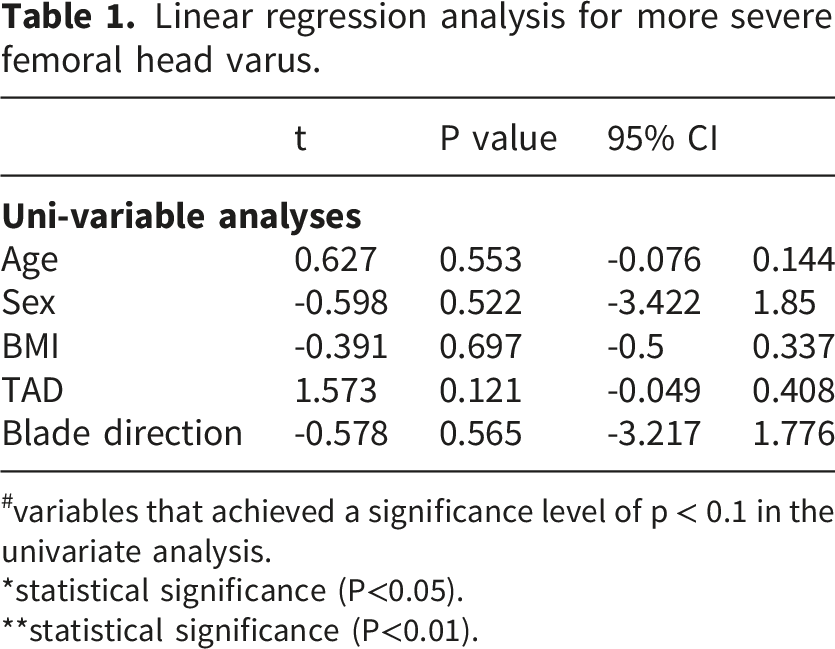
To determine whether changes in blade insertional direction can independently predict the progression of femoral head varus, linear regression analysis was performed in this study. 18 All demographic parameters, TAD value, and blade direction were included in the univariate regression analysis. In this process, p-values for each variable were assessed individually. Finally, variables with p-values < 0.1 were included in the multivariable regression analysis; those with p-values < 0.05 were deemed independent risk factors for more severe femoral head varus. 19
Numerical mechanical simulations
Model construction
The effect blade insertional direction changes on the local biomechanical environment has been investigated. This procedure offers a reasonable explanation for clinically observed phenomena from a biomechanical perspective. 19 The model construction strategy was extensively reported in our previously published studies, and we provide a brief description of the intact model construction here. Specifically, the outline of the proximal femur was derived from an artificial bone model rather than any patient-specific imaging data. This approach to model construction standardizes the outline across a specific research series and optimizes the repeatability of numerical mechanical simulations. 10 Subsequently, based on existing anatomical and imaging studies, the thickness of subchondral bone was established at 1.5 mm. Other regions of the femoral head were defined as cancellous bone, while the femoral shaft was designated as cortical bone.
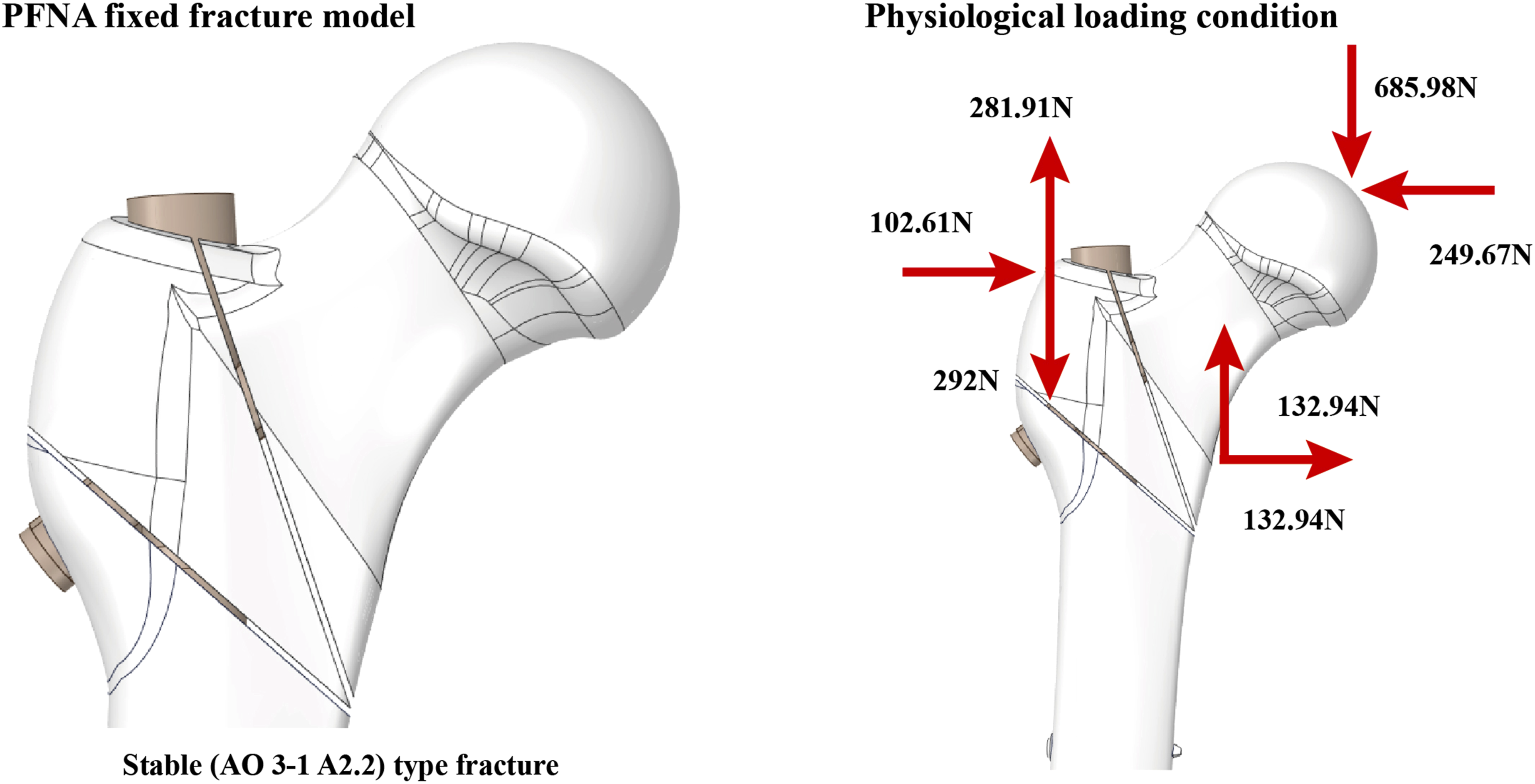
This study established a fracture model with an isolated lateral wall defect (i.e., AO/OTA 31-A2.2 type). In contrast to previous studies utilizing the AO/OTA 31-A2.3 type, the model employed in this study retained an intact medial wall while keeping all other parameters identical. Consequently, this cross-study comparison serves to highlight the biomechanical significance of medial support. To construct the fracture model with a lateral wall defect, a fracture line measuring 1 mm in thickness was created between the greater and lesser trochanters, followed by the removal of the lesser trochanter. Subsequently, another fracture line of 1 mm width was established from the attachment point of the lateral femoral muscle (the superior edge of the lateral wall) to the lesser trochanter.
10
Furthermore, PFNA-fixed fracture models were developed with three different blade insertion directions. In the control group model, the blade direction was aligned parallel to the axis of the femoral neck. Two additional models were constructed with ventral and dorsal blade orientations. In these configurations, the tip of each anti-rotation blade was rotated clockwise and counterclockwise until it reached the outline of cancellous bone in the femoral head (Figures 1 and 2).
9
Schematic illustration of the method for judging blade direction and construction of the numerical model with different blade insertion directions. Schematic for the construction of unstable fracture with laterall wall defect, and the physiological loading scenario.
Boundary and loading conditions
Compared to the hexahedral element, tetrahedral element can better fill structures with irregular curved surfaces. Therefore, only tetrahedral elements were utilized PFNA fixed models with different blade insetional directions in the mesh generation process. Different element sizes were employed for different components, with smaller sizes were utilized on the interfaces between blade and bony structures. By conducting the above mentioned element generation strategy, the average mesh quality surpassed 0.8 in the current models, thereby ensuring computational accuracy. 20 As above mentioned, intertrochanteric fracture is a typical type of low energy trauma in osteoporotic patients, and osteoporosis progression is an important reason for fixation failure and more severe femoral head varus. Consequently, both cortical and cancellous bone were set osteoporotic material properties. Moreover, consisted to our clinical practice, titanium alloy was designated for use in the PFNA operation (Figure 2).
To evaluate biomechanical change caused by different blade insertion directions, the inferior surface of the proximal femoral model was fully constrained. Physiological loading scenarios were established within these models to simulate the daily activities of patients, a bidirectional load was applied at the central point of the femoral head. This included a vertical load of 685.98 N and an outward force of 249.67 N that is parallel to the cross-section. 21 Furthermore, three distinct directional loads were applied at the greater trochanter: a vertical upward force of 281.91 N, a vertical downward force of 292 N, and an inward force measuring 102.61 N that is parallel to the cross-section (originating from the abductor muscles and vastus lateralis muscle). Lastly, two different loads were applied at the lesser trochanter: a vertical upward force combined with an inward force totaling 132.94 N (resulting from the iliopsoas muscle). 22
Results
Clinical review
In total, 56 patients with AO/OTA 31-A2.2 fractures (an unstable intertrochanteric fracture with a lateral wall defect) who underwent PFNA fixation were enrolled in this study (28 with a ventral blade trajectory and 28 with a dorsal blade trajectory).
When assessing inter- and intra-observer repeatability of imaging data measurements, both the Kappa value for blade direction judgment and the ICC value for femoral head varus angle measurement exceeded 0.8. Therefore, this study achieved ideal repeatability in imaging data measurement. Furthermore, regarding the computation of significant differences, no significant difference was observed in femoral head varus angles between patient groups with ventral and dorsal blade directions. According to the results of univariate linear regression analysis, P values for all demographic parameters, including age, sex, and BMI were greater than 0.1; similarly, P values for both TAD and blade direction also exceeded 0.1 (Figure 3 and Table 1). Measurement of femoral head varus in two representative cases with different blade directions at the 6-month follow-up. Linear regression analysis for more severe femoral head varus. #variables that achieved a significance level of p < 0.1 in the univariate analysis. *statistical significance (P<0.05). **statistical significance (P<0.01).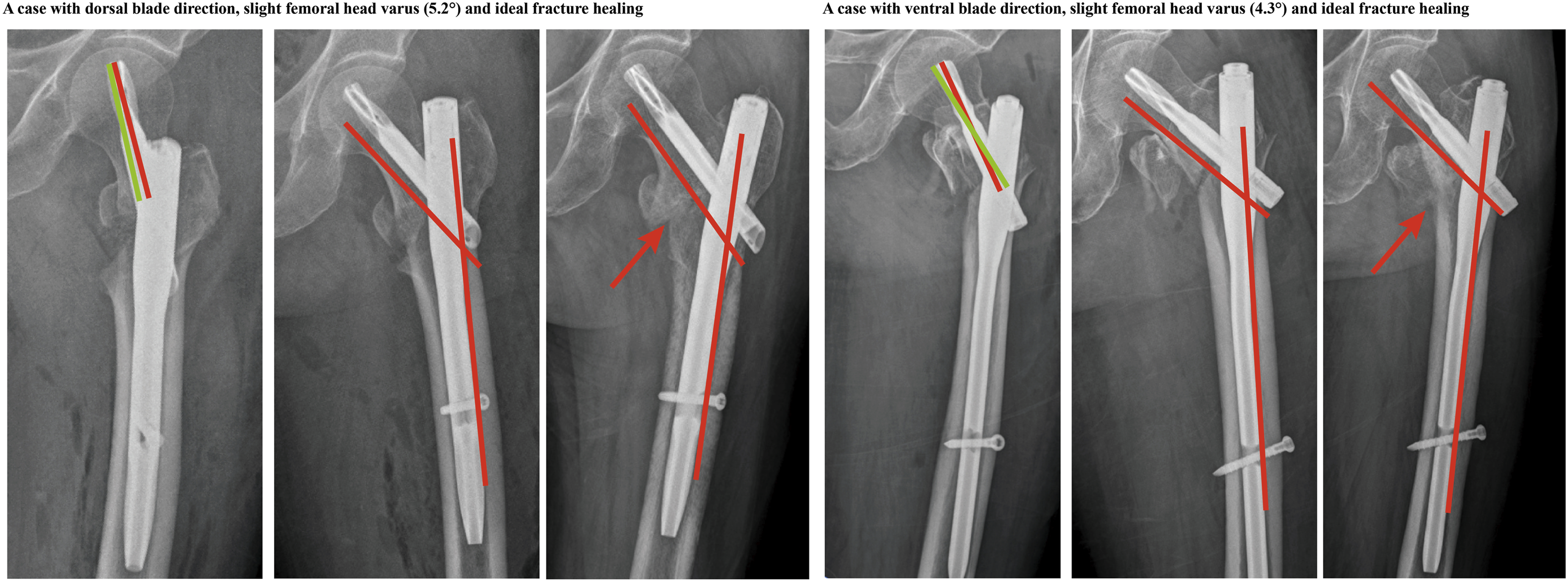
Numerical mechanical simulations
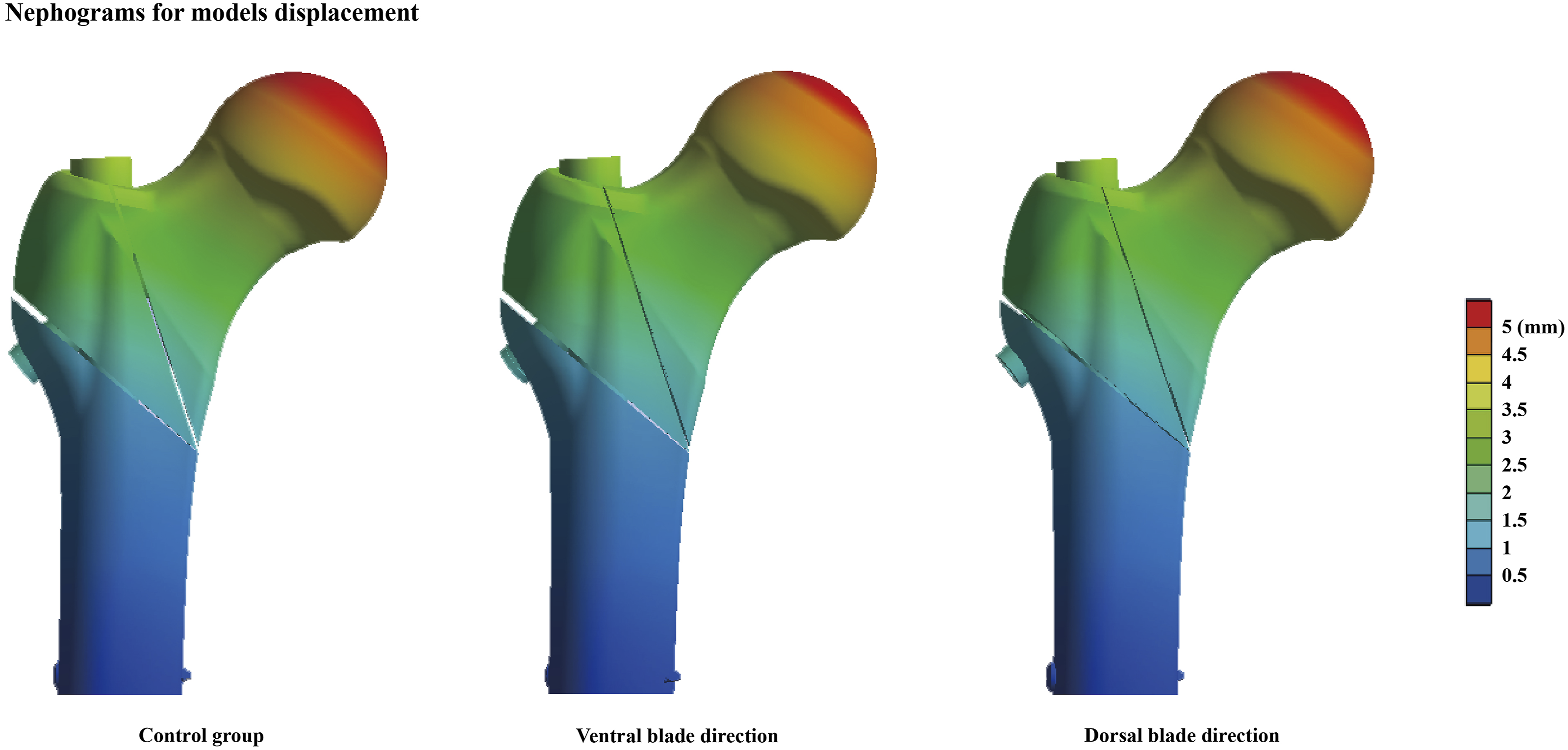
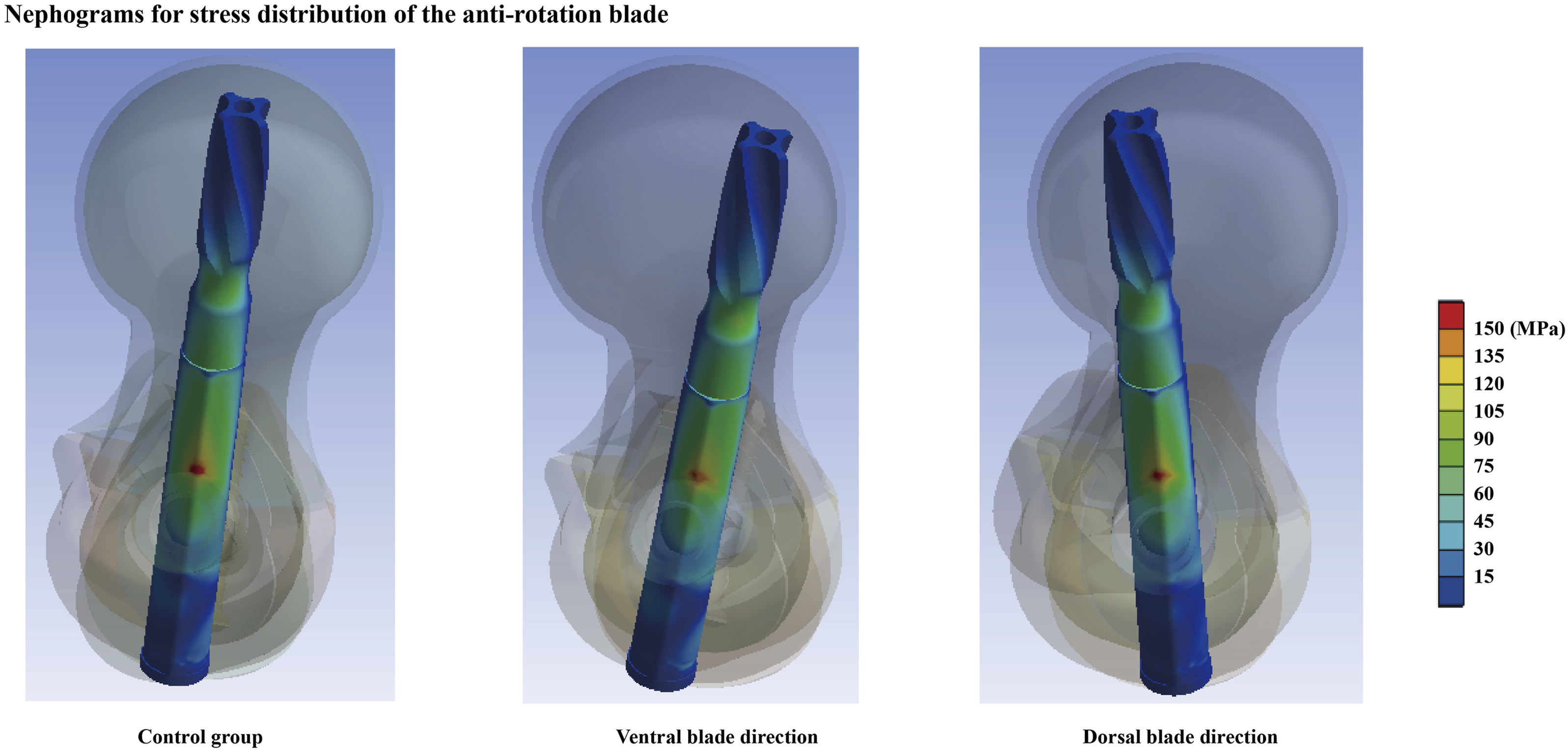
The stress and displacement values for both the femoral head and anti-rotation blade have been computed and recorded under various loading conditions to biomechanically assess potential incidences of femoral head varus. In accordance with the clinical review of the patient series, no significant biomechanical differences were observed between control group models and those with ventral or dorsal side blade orientations. Specifically, compared to the control group, the maximum stress value in cancellous bone decreased by nearly 10% in both models featuring ventral and dorsal blade insertion directions. Conversely, average stress values on the cancellous bone increased in these models. Furthermore, when compared to the control group, maximum stress values at the bone-blade interfaces exhibited reductions across different grades in models with both ventral and dorsal blade orientations. In contrast, only a slight difference (less than 3%) was noted in average interfacial stress values among different models. Finally, regarding initial fixation stability evaluation, it was found that the largest displacement value of the femoral head was recorded in the control group model; only a nearly 2% difference was observed in models with ventral and dorsal blade orientations (Figures 4–6). Computed femoral head maximum displacement value, and stress distribution on both femoral head and the anti-rotation blade. Nephograms for femoral head displacement in different models. Nephograms for anti-rotation blade stress distribution in different models.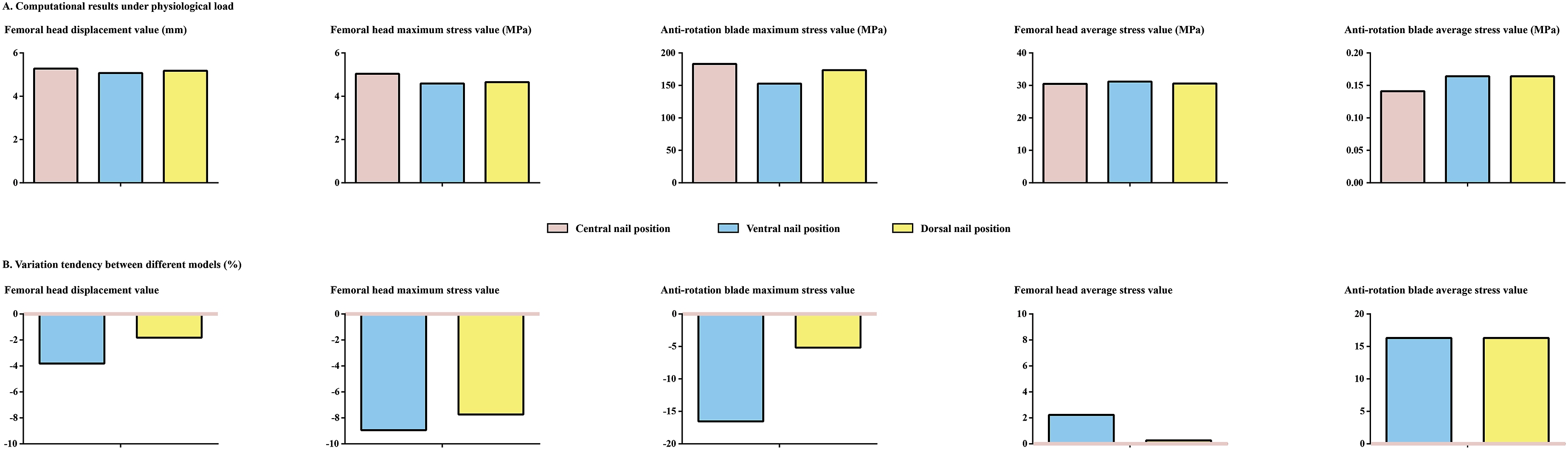
Discussion
Stable fixation is an essential foundation for fracture healing. 23 Any instability resulting from the fixation construct constitutes a potential risk factor for fracture nonunion. 24 Given that changes in the trajectory of fixation devices can affect fixation stability, 25 and the blade trajectory is highly adjustable within the femoral neck, we previously investigated the effect of anti-rotation blade trajectory on fixation stability in intertrochanteric fractures with combined medial and lateral wall defects. The findings indicated that a ventrally positioned blade trajectory increased the risk of femoral head varus, suggesting that the position of the internal fixation device should be carefully considered in such cases. 9
However, intraoperative adjustment of the blade trajectory may prolong operative time. Since patients with intertrochanteric fractures are often elderly and osteoporotic, 2 this additional surgical maneuver itself may increase the risk of perioperative complications. Moreover, although the biomechanical role of medial support in conducting axial compressive stress has been well documented, 3 whether the integrity of the medial wall can offset the adverse effects of a ventrally inserted blade has yet to be investigated.
In this study, based on consistent trends observed in both clinical and biomechanical investigations, we confirmed that in intertrochanteric fractures with isolated lateral wall defects, intact medial support can effectively compensate for the mechanical alterations associated with a ventrally positioned blade. Therefore, our findings suggest that when the medial wall remains intact, there is no need to adjust the trajectory of the anti-rotation blade. 2 This provides a valuable reference for intraoperative decision-making and offers a novel perspective on the biomechanical role of medial support.
Contrary to previously published studies, the current patient series did not demonstrate that TAD reduction resulted in more severe femoral head varus. 26 The adverse effects of a large TAD on fixation stability have been extensively documented. 27 In these studies, an increase in TAD has been associated with a higher risk of fixation failure and the need for revision surgery. Consequently, it is commonly accepted that selecting a longer blade can optimize fixation stability and reduce the risk of complications. 4 Based on these findings, a TAD smaller than 25 mm is recommended for PFNA operations, 14 and all enrolled patients in this study had TAD values below this threshold. However, according to our results, among patients with TAD values less than this threshold, further reductions in TAD do not lead to improved clinical outcomes. Therefore, this study validate the “safety threshold effect” of 25 mm TAD value, provides evidence supporting these conclusions rather than contradicting previously published research.
The strengths and limitations of the current research protocol should be clarified. First, the integration of clinical and biomechanical analyses represents a key methodological strength. 28 Using this approach, we first conducted clinical studies. The results, including fracture classification and blade position measurements, were then used to guide the construction of the biomechanical model, allowing the biomechanical findings to help explain the mechanisms underlying the clinical observations. Consistent trends were observed across both investigations, and this concordance enhances the credibility of our conclusions. 29
On the other hand, the numerical model was constructed based on an artificial standard model rather than on patient-specific imaging data. Individual differences in anatomical geometry and material properties across models can introduce confounding variables that may influence outcomes. 30 Controlling for such variables by using a unified model is an effective strategy to improve study reproducibility. 10 The reference model we used is widely employed in similar research, and the assigned material properties are consistent with those in comparable studies 31 ; its representativeness for osteoporotic intertrochanteric fractures has been broadly acknowledged. More importantly, this unified modeling approach facilitates comparison of conclusions across different studies. Because the current study and our previous research used the same model specifications and implant dimensions, differing only in fracture type, we can effectively rule out potential confounding effects from other variables. 31
However, from another perspective, this advantage also highlights a limitation of the study: it did not account for individual patient differences, such as variations in femoral anatomy and bone density, which may influence fixation stability and clinical outcomes. Since this was a retrospective study, dual-energy X-ray absorptiometry (DXA) was not routinely performed in the enrolled patients, and thus quantitative bone mineral density data are not available. We acknowledge this as a limitation of the current study and have now clearly stated it in the revised manuscript. Nevertheless, several factors may have partly mitigated the impact of this limitation. First, the two study groups (grouped by blade direction) were highly comparable in age and sex distribution, which are key determinants of bone mass; patients of similar age and sex are generally expected to have broadly comparable bone stock. Second, in our computational finite element analysis, we used a uniform elastic modulus for bone to isolate the mechanical effect of blade direction. Under this controlled condition, the resulting stress differences between the dorsal and anterior blade positions were minimal, suggesting that blade direction per se has little influence on local mechanical stress. While this does not replace actual osteoporosis assessment, it indicates that when material properties are held constant, the biomechanical conclusion remains unchanged. Given these considerations, we believe that the absence of DXA data is unlikely to have fundamentally altered the reliability of our main finding. However, we fully acknowledge that this remains a study limitation, and we plan to incorporate bone density assessment in a future prospective study to further validate our conclusion.
Conclusion
Through a clinically informed biomechanical investigation, this study demonstrates that modifying the blade insertion trajectory does not compromise fixation stability or induce elevated stress at the bone-implant interface. Moreover, such directional variations do not increase the risk of femoral head varus progression in unstable intertrochanteric fractures presenting with lateral wall defects when medial wall integrity is preserved. These findings thus provide new insight into the biomechanical relevance of medial support in maintaining fixation stability.
Footnotes
Ethical considerations
Approval for this study was obtained from the Ethics committee of the People’s Hospital of Gaoxian.
Author contributions
Conception and design: Tao Zhong, and Zengru Xie. Acquisition of data: Wenqiang Xu, Yue Xu, Xin Zheng, and Dong Li. Analysis and interpretation of imaging data: Tao Zeng, Lijunpeng Jia, and Wenqiang Xu. Statistical analysis: Tao Zeng, Yue Xu, and Jingchi Li. Manuscript Preparation: Tao Zeng Wenqiang Xu, and Yue Xu. Manuscript revision and modification: Jingchi Li, and Zengru Xie.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Key Project of the National Natural Science Foundation of China Project (82260409).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All the data of the manuscript are presented in the paper.