
Abstract
Purpose
We aimed to find the distinctions between IV and IA TXA concerning intraoperative visual clarity, postoperative pain management during ARCR.
Methods
In our retrospective cohort, propensity score matching study, we included patients who had a history of rotator cuff tears and at least six months of unsuccessful conservative treatment. The primary outcome, visual clarity during surgery, was evaluated using a five-grade arthroscopic visual scale (AVS) by the operating surgeon. This scale ranged from grade 1, indicating optimal clarity, to grade 5, the least clarity necessitating a switch to open surgery. These assessments were made at 10-minute intervals during the review of the operation’s video footage. We also measured postoperative pain levels as secondary outcomes.
Results
IA group included 30 patients and the IV group had 31 patients, with no significant differences in demographics or tear dimensions (p=0.686). The IA and IV groups showed similar irrigation fluid volumes, operation times, and AVS mean scores. IA group had a higher proportion of favorable AVS grades (grades 1–2) compared to IV group (90.0% vs 64.5%, p=0.011). Pain assessment using the Visual Analog Scales (VAS) were lower in the IA group at 24, 48, and 72 hours postoperatively; however, after Bonferroni correction, only the 48-hour difference remained statistically significant (2.7 vs. 4.2, p=0.008).
Conclusions
Both IA and IV TXA may be useful adjuncts in ARCR. In this propensity score-matched cohort, IA TXA was associated with a higher proportion of favorable AVS grades and a modest short-term pain benefit, with statistical significance only at 48 hours after correction for multiple comparisons. Within the limitations of this study, IA TXA may be considered a reasonable alternative, particularly when IV administration is not suitable.
Keywords
Introduction
Arthroscopic rotator cuff repair (RCR) represents a significant advancement in the treatment of full-thickness rotator cuff tears, offering benefits such as reduced complication rates, and expedited return to daily activities.1,2 A critical component in optimizing the outcomes of this procedure is maintaining clear visual fields during surgery, which is directly impacted by the management of intraoperative bleeding.3,4 Despite advancements in surgical techniques and equipment,5,6 the challenge of optimizing visual clarity while minimizing postoperative pain remains a pivotal concern in arthroscopic RCR.
Tranexamic Acid (TXA), known for its well-established hemostatic properties, has become a valuable agent in reducing blood loss and minimizing postoperative complications.3,4,7–9 It has a proven safety profile across various fields of orthopedic surgery, making it a viable option for arthroscopic procedures.10–13 Until now, TXA has typically been administered via intravenous injection prior to arthroscopic surgery, showing improvements in visual clarity. 4 Recently, however, the administration of TXA has the disadvantage of being only limitedly usable in some patients with thromboembolic events. 14 Some studies have indicated that intra-articular TXA injections in patients undergoing arthroscopic rotator cuff repair can also enhance visual clarity. 15 However, the existing literature predominantly investigates the effects of TXA without distinguishing between its modes of administration, specifically intra-articular (IA) and intravenous (IV). 15 This lack of differentiation results in an incomplete understanding for orthopedic surgeons and clinical practitioners on how to fully maximize the benefits of TXA in arthroscopic RCR.
Though prior studies have confirmed the effectiveness of TXA in arthroscopic RCR (8), a more nuanced understanding of its benefits and potential risks, depending on the method of administration; IA and IV, should be required. Therefore, we conduct a detailed comparative analysis of IA versus IV administration of TXA in the context of arthroscopic RCR. The purpose of this study was to elucidate the distinctions between these administration routes concerning intraoperative visual clarity, postoperative pain management, and the incidence of complications. It was hypothesized that compared to IV administration of TXA, IA TXA can more improve visual field clarity, shorten the operation time during ARCR, and more reduce initial postoperative pain, effectively.
Methods
Study design and patient selection
Inclusion and exclusion criteria.
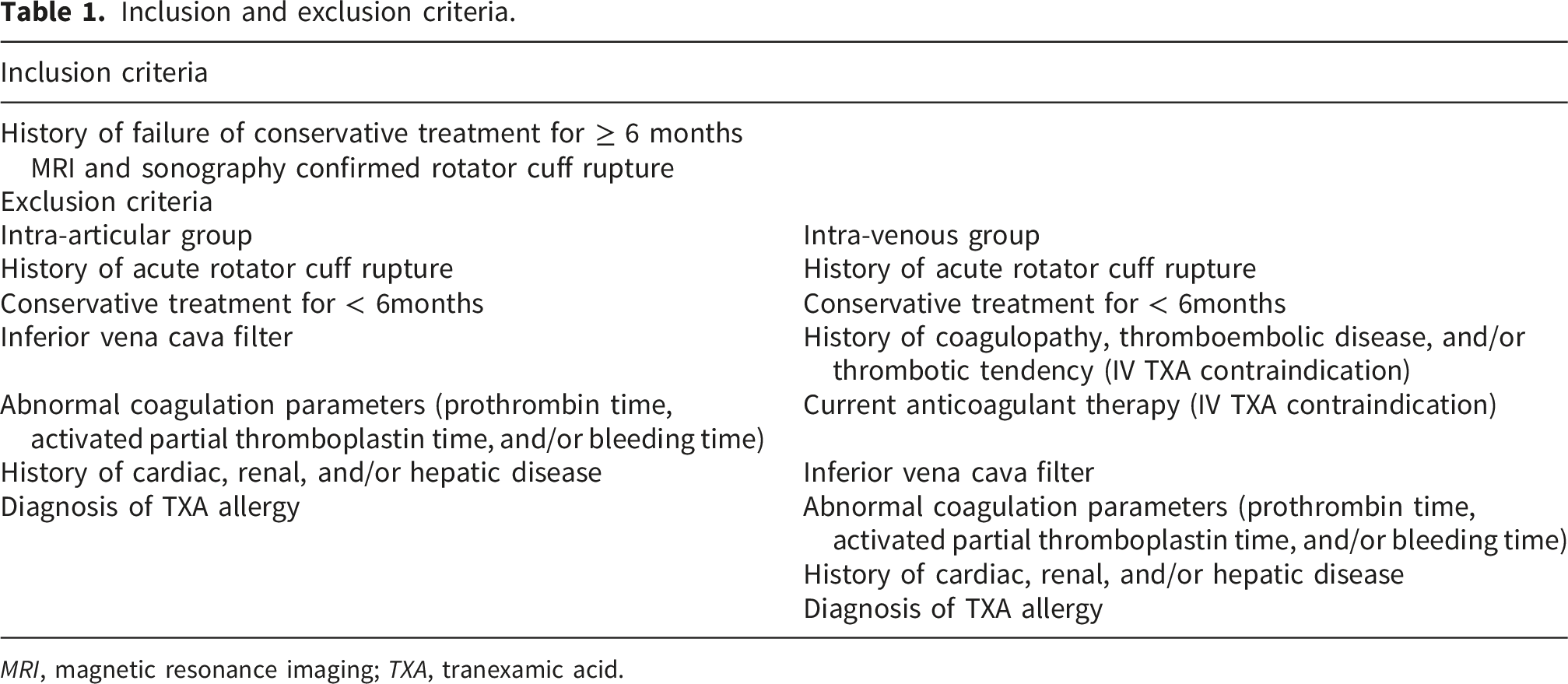
MRI, magnetic resonance imaging; TXA, tranexamic acid.
Preparation of irrigation solution and TXA injection
Three-liter bags of arthroscopic irrigation solution (normal saline) were prepared by the operating nurse. In the IA group, 500 mg of TXA was added to every 3-L bag of irrigation solution, resulting in an approximate concentration of 0.16 mg/mL throughout the procedure (to prevent chondrocyte death and damage to peri-articular tissues as reported earlier.16–18 Thus, TXA was delivered by continuous admixture into the irrigation fluid rather than by a separate terminal intra-articular bolus. In the IV group, the irrigation solution remained TXA-free, and 500 mg of TXA was administered intravenously immediately before surgery. 15 No epinephrine was used in the irrigation solution in either group.
Surgical technique and postoperative management
Each procedure was carried out by the same surgeon, HK., with patients undergoing general anesthesia in lazy lateral position, avoiding the use of regional anesthesia. This standardized approach ensured that the same surgical steps were consistently followed in the same order for every patient, regardless of their allocation to the IA or IV TXA group. The surgical protocol involved a comprehensive assessment of the glenohumeral joint and the rotator interval. In instances where a degenerative biceps tendon was identified, a biceps tenotomy was performed (involving 15 patients from the intra-articular group and 13 from the intra-venous group). Acromioplasty was conducted on all patients across both groups. No additional procedure was undertaken alongside this. The repair of the supraspinatus tendon was executed using a double-row suture bridge technique. A pressure-regulated pump (CONMED comp.) maintained the irrigation solution’s pressure at a steady 60mm Hg throughout the surgery, and no cases involved the use of flush irrigation. The total irrigation volume used during each procedure was also recorded. The anesthesiologist monitored and recorded the mean arterial pressure (MAP) during each operation.
Immediately following the surgery, patients were fitted with an abduction brace and instructed to minimize active shoulder movement and abduction while in the hospital. For pain control, every patient received a 500mg paracetamol injection every 12 hours, consistent across both groups. A suprascapular nerve block was administered to all patients, and paracetamol was the exclusive medication used for pain management. Patients were discharged on the second day after the operation, once their condition was stable and their pain levels were manageable.
Assessment of intraoperative arthroscopic visual clarity and secondary outcome parameters
The entire surgical process of all patients was recorded. To assess the clarity during surgery, a unique arthroscopic visual scale (AVS), akin to the system employed by van Montfoort et al.,
19
was used by the two surgeons, HK. and THO. This AVS comprised five levels: Grade 1signified complete absence of visual obstruction due to bleeding; grade 2 represented mild visual disruption; grade 3 indicated moderate interference; grade 4implied severe disturbance; and grade 5, the most extreme, necessitated a shift to open surgery due to overwhelming visual impairment (Figure 1). The AVS rating for each patient was determined as follows: Surgeons reviewed the video recordings of the arthroscopic procedure post-surgery, noting the AVS every 10 minutes-a chosen interval reflecting the dynamic nature of bleeding in arthroscopy in a blinded for the interventions. Subsequently, an average score per patient was computed. Although grade 5 was an on-the-spot assessment and was intended for postoperative review, it was not applicable in this case. Arthroscopic visual scale grade used to assess clarity of view during arthroscopic procedure: grade 1 (a), grade 2 (b), grade 3 (c), grade 4 (d).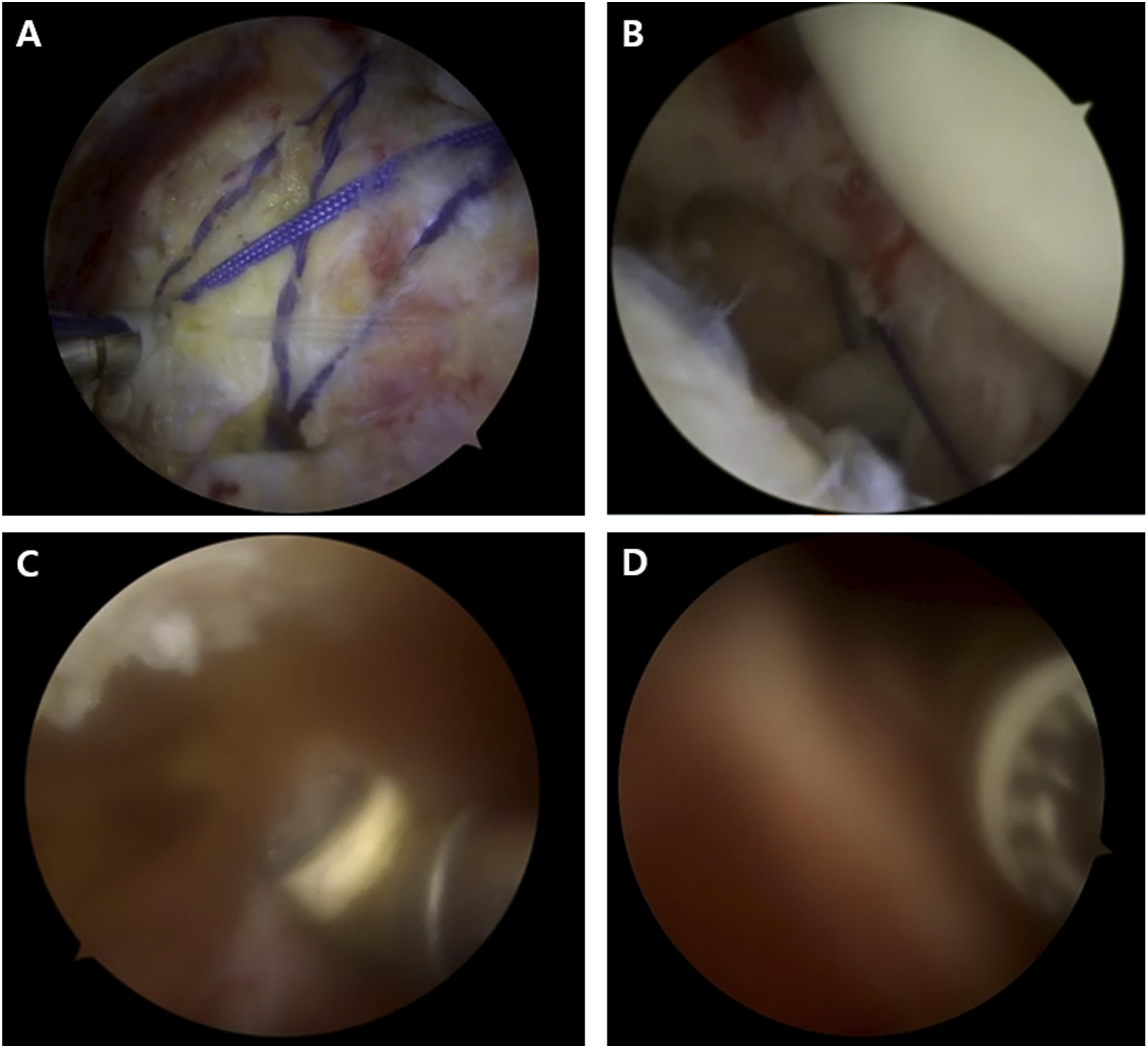
For a comprehensive evaluation, HK. and THO re-watched the videos after two weeks later, and separately reviewed them. The consistency of these observations was confirmed with an intraclass correlation coefficient ranging from 0.81 to 0.97, indicating strong intra-observer reliability. And another orthopaedic surgeon, MSY., watched and reviewed AVS score. The inter-observer reliability of radiographic outcome measurements was determined using the intraclass correlation coefficient, showing values of 0.81-0.97.
Pain levels were measured by ward nurses, who were not aware of the study details, using the visual analog scale (VAS) at 8, 24, 48 and 72 hours after the operation. Additionally, the mean arterial pressure (MAP) and total duration of the surgery were documented. The average values of all these parameters were then compared between the two groups.
Statistical analysis
To calculate the sample size, G*Power software (version 3.1.9.7; gpower.hhu.de) was used prior to the study, and statistical power (1 - β), alpha error, and impact value were calculated as 0.8, 0.05, and 0.8, respectively. As a result of this a priori power analysis model, it was calculated that 26 patients were required in each group. Data analysis was performed using the SPSS software (version 19.0; Chicago, Illinois). Data are expressed as mean standard deviation or as average values. Age, sex, surgery time, mean arterial blood pressure, surgical visualization score (AVS score), and postoperative pain score were compared between group using independent-samples test after 1:1 propensity score matching (PSM). Normality was assessed using Kolmogorov-Smirnov test for categorical variables and the Shapiro-Wilk test for continuous variables. Student’s t test was used to compare continuous variables between IA and IV groups, including age, sex, average tear dimension, MAP, surgery time, AVS score, VAS pain score. Bonferroni correction was applied to account for multiple comparisons across groups, depending on the postoperative time points. The significant p-value was 0.0125 for VAS pain score. Fisher’s exact test was performed to compare the AVS grade distribution ratio. Results were reported at a confidence interval of 95%, and P < .05 was considered statistically significant.
Results
Of the 107 patients who had rotator cuff repair surgery, 31 were excluded based on the inclusion and exclusion criteria (16 were receiving anticoagulant therapy; 7 had a history of cardiac, hepatic, and/or renal disease; 4 had an abnormal prothrombin time or activated partial thromboplastin time at the time of surgery; 2 had acute RCTs). The remaining 76 patients were enrolled in the study (Figure 2). Flowchart of study population. PT, prothrombin time; PTT, partial thromboplastin time; IA, intra-articular; IV, intra-venous.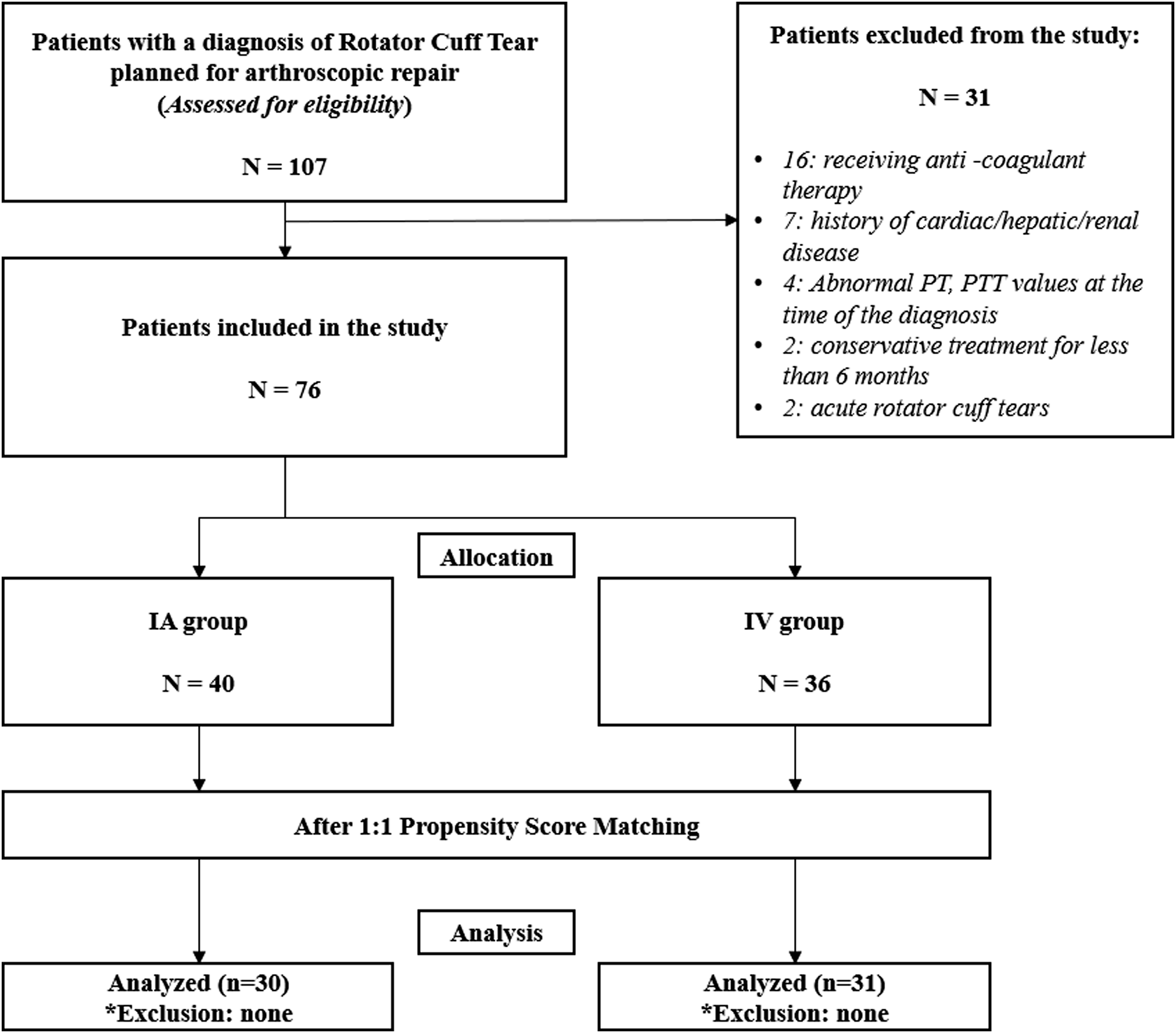
Demographic data of patients and evaluation of intergroup differences.
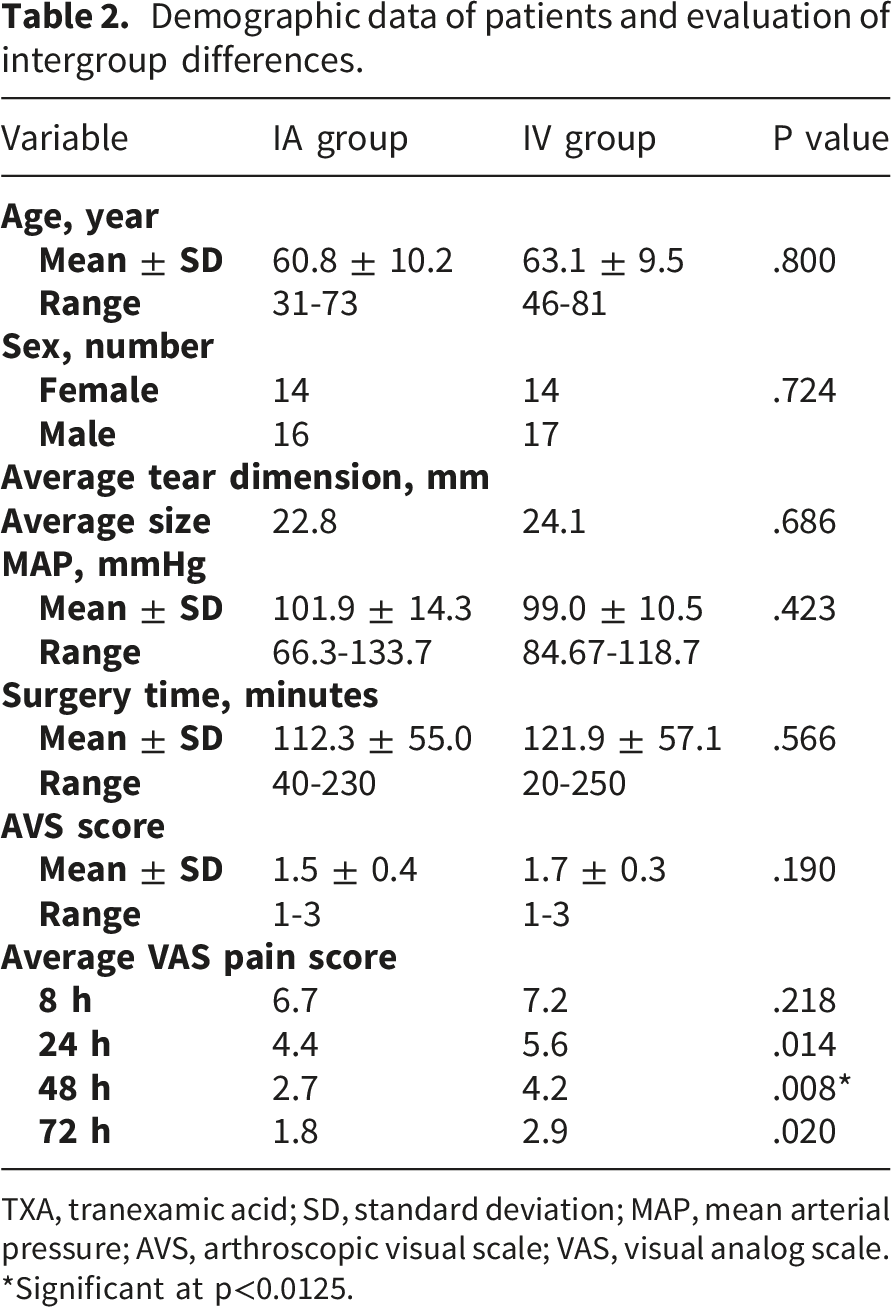
TXA, tranexamic acid; SD, standard deviation; MAP, mean arterial pressure; AVS, arthroscopic visual scale; VAS, visual analog scale. *Significant at p<0.0125.
The mean total irrigation volume used during surgery was 36.9 L in the IA group and 39.2 L in the IV group (p=.751). The mean duration of operation time in the IA and IV group was 112.3 minutes and 121.9 minutes, respectively (P = .566). The mean AVS score in the IA group (1.5 ± 0.4) was not significantly different with the mean AVS score in the IV group (1.7 ± 0.3) (P = .19). IA group was reported to have percentages with AVS score of grades 1-2 (90.0%), grade 2-3 (6.7%) and grade 3 (3.3%). IV group was reported to have percentages with AVS score of grades 1-2 (64.5%), grade 2-3 (35.5%) and grade 3 (0%). No AVS score of grades more than 4 was reported in either group (Table 2). The AVS grade distribution ratio was significantly different between two groups (p = 0.011) (Figure 3). Arthroscopic visual scale grade distribution. *Significant at p<0.05.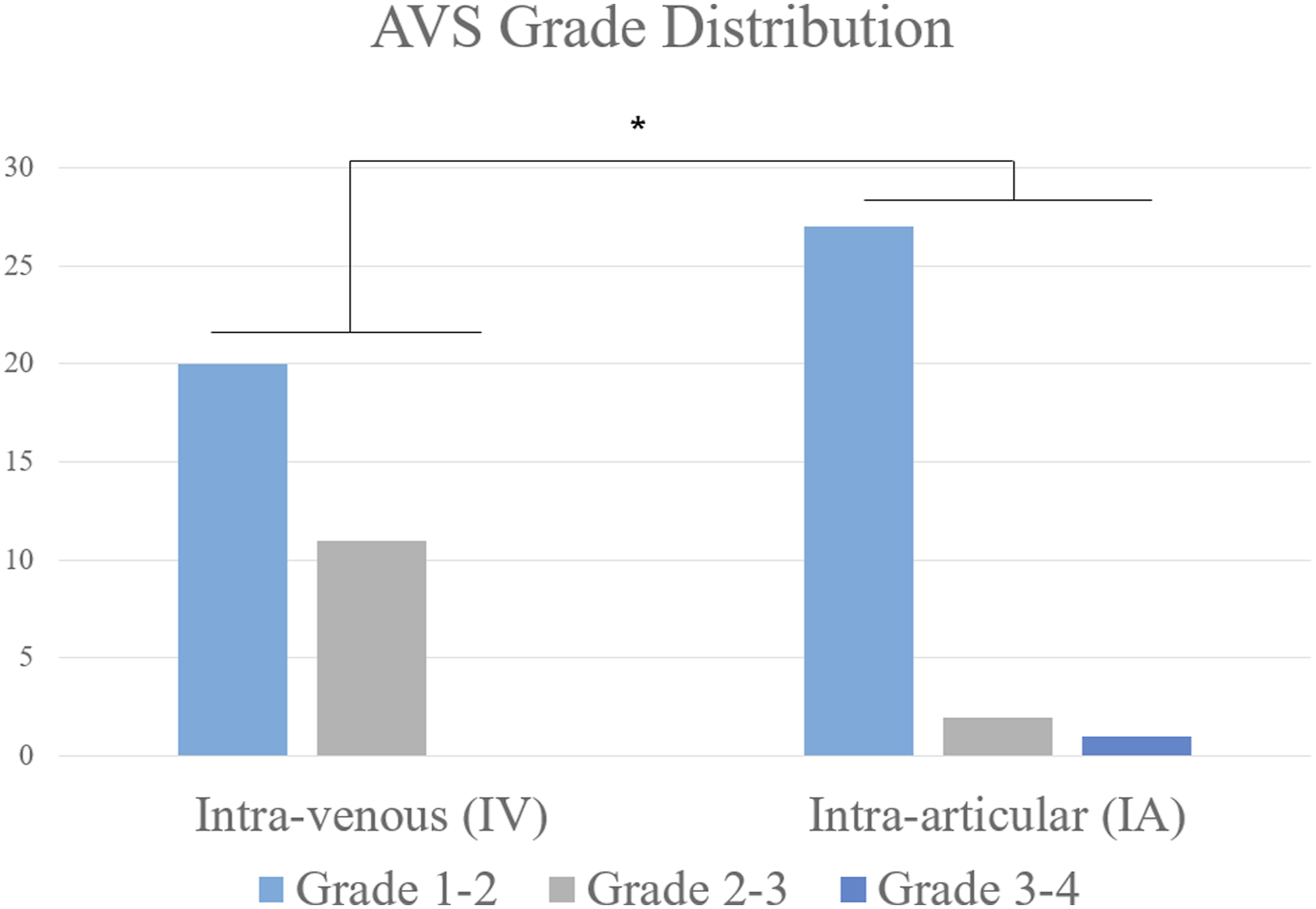
MAP was assessed in both groups to examine its influence on visual clarity. The MAP was noted to be 101.8 ± 14.3 mm Hg in the IA group and 98.9 ± 10.5 mm Hg in the IV group, showing no statistically significant difference (P = .423). The Pearson correlation analysis also indicated no significant relationship between MAP and AVS score (coefficient = 0.16, P = .915) (Table 2).
Analysis of VAS pain scores showed lower scores in the IA group at 24 hours (4.4 vs. 5.6, p=.014), 48 hours (2.7 vs. 4.2, p=.008), and 72 hours (1.8 vs. 2.9, p=.020). However, after Bonferroni correction, only the 48-hour comparison remained statistically significant (p<0.0125). No thromboembolic events or other major complications were observed in either group through discharge. Among the matched patients, 4 in the IA group had IV-specific contraindications, defined as a history of thromboembolic disease and/or current anticoagulant therapy, whereas no such patients were included in the IV group. These 4 patients did not experience thromboembolic events, pulmonary embolism, or seizure until the next outpatient clinic follow-up (Table 2).
Discussion
In our study, IA TXA was associated with a higher proportion of favorable AVS grades and a modest short-term pain benefit compared with IV TXA. Notably, the IA group included patients with contraindications to IV TXA. Although this reflects real-world clinical practice, it also introduces the possibility of residual confounding when directly comparing the two administration routes. Therefore, the comparative findings of this study should be interpreted with caution.
A key observation was that the difference in postoperative pain was limited to the early postoperative period. Although VAS scores were lower in the IA group at 24, 48, and 72 hours, only the 48-hour comparison remained statistically significant after Bonferroni correction. Accordingly, the analgesic effect of IA TXA should be interpreted as modest and short-term rather than as a sustained clinical advantage. One possible explanation is a reduction in postoperative hemarthrosis; however, postoperative blood loss, hemarthrosis volume, and retained intra-articular TXA were not directly measured in this study. Therefore, the observed short-term pain difference should not be interpreted as proof of superior blood-loss control or as evidence of pharmacologic superiority of IA over IV TXA. Previous studies have suggested that TXA may improve intraoperative visualization and reduce postoperative bleeding-related sequelae in arthroscopic procedures. Li et al. 4 reported that preoperative intravenous TXA improved intraoperative bleeding during shoulder arthroscopy, although it did not significantly affect postoperative blood loss or hematologic parameters. Zhu et al. 21 reported that intra-articular TXA during shoulder arthroscopy reduced blood loss and hemoglobin loss, and similar findings have been described in knee surgery.22,23 In addition, intra-articular TXA in arthroscopic anterior cruciate ligament reconstruction has been associated with reduced postoperative hemarthrosis and early pain relief. Taken together, these prior findings may support a possible role of TXA in reducing early postoperative symptoms, but the mechanism underlying the transient pain difference observed in our study remains speculative and requires further investigation. 24
Furthermore, while the mean AVS did not significantly differ between the groups, a higher number of patients in the IA group achieved lower AVS grades (grade 1-2) than IV group. Even though total volume of TXA in each group was totally different, that it was one of our limitations, this difference could be supported from previous study that local injection have more effective to control bleeding in postoperative status.25,26 Although the efficacy of TXA in reducing blood loss and improving surgical visibility in orthopedic procedures is well-documented,10,15,27 the optimal route of administration, particularly in arthroscopic rotator cuff repair (RCR), remains underexplored. Our findings suggest that IA TXA may be a reasonable alternative to IV TXA in arthroscopic RCR, particularly with respect to the distribution of favorable AVS grades. However, the present data do not establish clear superiority of one route over the other. Contrary to our expectations, we found no conclusive evidence to suggest that the improved visual clarity directly translates to shorter surgical times. This aspect warrants further investigation to understand the relationship between visual field clarity and operative duration.
Lastly, the absence of thromboembolic events or other complications in both groups underscores the safety profile of TXA in arthroscopic RCR, aligning with existing literature that highlights TXA’s safety across various orthopedic procedures.13,14 Although no thromboembolic events or other major complications were observed in this cohort, these findings should not be interpreted as establishing superior safety of IA TXA over IV TXA, because patients with IV-specific contraindications were included only in the IA group. This aspect of our findings highlights the need for personalized approaches in the administration of TXA, considering patient-specific risk factors and contraindication. These findings have important implications for optimizing surgical outcomes and patient care in arthroscopic rotator cuff repair, advocating for a tailored approach to TXA administration based on individual patient profiles and clinical circumstances.
It is important to acknowledge the limitations inherent in a retrospective cohort study, including the potential for selection bias and the influence of unmeasured confounding variables. Additionally, the relatively small sample size and single-center design, as well as the absence of a control group like the non-TXA administered group, may limit the generalizability of our findings. Future research should aim to replicate these results in larger, multicenter randomized controlled trials to provide more definitive evidence on the comparative efficacy and safety of IA versus IV TXA administration in arthroscopic RCR. Moreover, there was possibility of risk that IA TXA could have negative effect on articular cartilage. There were some reports that TXA could make chondral injury through chondrocytes apoptosis. 18 Even though we did not confirm there was a negative effect of TXA on articular cartilage by long-term follow-up, we applied IA TXA at low concentration based on the previous finding of Want et al., which TXA concentrations of less than 50 mg/ml in joint could not have toxic effect on chondrocyte. 18
Another important limitation of this study is that patients with IV-specific contraindications, namely a history of thromboembolic disease/thrombotic tendency and/or current anticoagulant therapy, were included only in the IA group. Although this reflects real-world clinical practice, it introduces the possibility of residual confounding that may not have been fully addressed by propensity score matching. Therefore, direct comparisons of safety and efficacy between IA and IV TXA should be interpreted with caution. Lastly, In the IA group, TXA was mixed into every 3-L bag of irrigation fluid. Based on the mean irrigation volume of 36.9 L, the theoretical total amount of TXA mixed into the irrigation system was approximately 6.15 g per case. However, because arthroscopic surgery uses a continuous inflow-outflow system, the retained intra-articular amount and systemic absorption could not be quantified. Accordingly, the present study does not establish the optimal IA dose or demonstrate a pharmacologic advantage of IA over IV TXA. Further pharmacokinetic and dose-finding studies are required.
Conclusion
Both intra-articular and intravenous TXA may be useful adjuncts in arthroscopic rotator cuff repair. In this propensity score-matched cohort, IA TXA was associated with a higher proportion of favorable AVS grades and a modest short-term pain benefit, with statistical significance for pain observed only at 48 hours after correction for multiple comparisons. Because patients with IV-specific contraindications were included only in the IA group and the retained intra-articular dose could not be quantified, direct comparative interpretation should be made cautiously. Within these limitations, IA TXA may be considered a reasonable and safe alternative, particularly when IV administration is not suitable.
Footnotes
Acknowledgement
This research was supported by EMBRI Grants 2023-EMBRIDJ0003 from the Eulji University. This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government(MSIT) (RS-2023-00278547), awarded to HK. The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Ethical considerations
Institutional Review Board of Dajeon Eulji Medical Center, IRB number 2023-07-023.
Consent to participate
The need for consent to participate was waived by an Institutional Review Board (Institutional Review Board of Dajeon Eulji Medical Center) because the study was designed as retrospective cohort study.
Author contributions
MSY analyzed and interpreted the patient data regarding the arthroscopic image visuality. HK and TO performed data analysis and validation and were a major contributor in writing the manuscript. IHJ and KHK gave the conceptualization of this study and design, and KHK finally reviewed. .All authors read and approved the final manuscript
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (RS-2023-00278547), awarded to HK. The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. This research was supported by EMBRI Grants 2023-EMBRIDJ0003.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analysed during the current study are not publicly available due to the ethical issue, but are available from the corresponding author on reasonable request.
IRB protocol
IRB number: EMC 2023-07-023.