
Abstract
The Universal Wellbeing Model emerged from a fifteen-year multi-phased, and mixed methods wellbeing research, and evaluation program. Investigations have included traditional, literature, mixed, and practice-based methods, and these have been published. Detailed by the research team, to date have been findings about the effectiveness of both the Whare Tapa Wha, and Whare Tapa Rima, program completion rates in higher education settings. The focus of this paper is on disseminating the unpublished outcomes of a Case Study Impact Evaluation that examined the overall value, and impact of the past investigations to give a voice to the adult higher education students, teaching/research staff, and professional pastoral care/wellbeing practitioners involved. The participatory method used examined the value and impact of these investigations on the three participating groups. This method also considered both the intended, and unintended consequences over time. The evaluation revealed not only unexpected ethnic, and cultural perspectives of the students, teacher/research staff and professional pastoral care/wellbeing practitioners involved but also their willingness to be part of solutions to the challenges identified. Their perspectives have progressed understandings of the complexities, challenges, and ethical dilemmas for those using and providing academic and pastoral care, and wellbeing support services to diverse students in higher education settings globally. The evaluation revealed the intended and positive experiences and consequences, as well as the unintended and negative ones. The analysis of evaluative data gathered reveals the unique capacity of a case study impact evaluation to contribute significantly to the creation of new knowledge, understandings, and practices. These insights then unexpectedly catalysed further discovery, enabling researchers to locate the final pieces of a larger theoretical puzzle under investigation: the nature of wellbeing and ways students and others can empower themselves to transform their wellbeing.
Keywords
• Wellbeing models without theoretical and evidence bases are implemented widely in higher education and other sectors. • Wellbeing programs can improve higher education student program completion rates. • Understandings of evidence-based multi-disciplinary and authentically holistic wellbeing models designed to support human potential, thriving and flourishing is limited.
• Strengthens the case for more robust theoretical and evidence-based wellbeing model development in higher education and other fields. • Highlights the potential for serious harms to result from implementation of inadequately researched and developed wellbeing models. • Identifies the potential for harms to occur when a wellbeing model underpinned by a single ethnic/cultural or discipline perspective is implemented with diverse populations.What We Already Know
The Original Contribution the Article Makes to Theory And/or Practice
Background
This article focuses on the outcomes of a case study impact evaluation with three participant groups in two research investigations (Scholfield et al., 2011; Fielden et al., 2020a). This evaluation critically examined and revealed key themes that emerged on the value and impact of these investigations on three participant groups who took part in these studies: students, staff/researchers, and professional pastoral care/wellbeing practitioners. Researchers also triangulated and synthesised the emerging themes from this evaluation to detail the collective value and impact of participants’ perspectives over time, showing how their insights became the catalyst for what would become the most significant outcome of an ongoing fifteen-year wellbeing research and evaluation program: the emergence of the Universal Wellbeing Model.
In 2008 teaching, research and professional pastoral care/wellbeing practitioners in a higher education institution in South Auckland, New Zealand, were faced with a new challenge. They needed to support a cohort of largely indigenous and diverse Pacific Island adult students who did not choose freely to enrol in the education programs they entered. Most enrolled to maintain financial support from the government of the day. Despite the practitioners at the host institution being recognised nationally for their effectiveness in supporting adult students to achieve program completions, the new cohort brought many complex and new needs with them for staff to address.
To meet the new academic and wellbeing needs of this cohort of adult students, staff sought a model and approach to guide and enhance their practice with these students. Staff aimed to improve program completions, credit achievements, and retention rates, and to reduce students’ withdrawals, and terminations. Staff also sought to improve students’ wellbeing with empathetic, compassionate, and culturally safe practices (Papps, 2002; Ramsden, 2002) using a wellbeing literacy-orientated approach (Oades et al., 2021). The initial theoretical model located and implemented by the staff to enhance and guide their student support practices was the Whare Tapa Wha – the Four-Sided House (Durie, 1994).
This model, originally developed and published to assist non-indigenous health workers to support indigenous patients in health care settings included four dimensions: Social-Whanau, Intellectual/Emotional-Hinengaro, Spiritual-Wairua and Physical-Tinana.
Keen to trial this model, staff applied for and gained national research funding to investigate its effectiveness in terms of their practice objectives. The investigation was planned, conducted and duly reported (Schofield et al., 2011). The objectives sought by the staff were all achieved. Participants provided feedback on the first investigation, which prompted the team to conduct a second investigation aimed at further improving outcomes. This subsequent study introduced a new model, included a much more diverse adult student population, and involved the entire organisation and a broad range of staff, using a ‘whole of organisation’ approach (Stevenson & Zagala, 2021;Stevenson, Gurung, & Zagala, 2024).
The expanded population included indigenous, national, and diverse international adult higher education students. The teaching/research and pastoral care/wellbeing practitioners were also more diverse in this investigation. A new, more comprehensive and inclusive Whare Tapa Rima – the Five-Sided Home Model (Moeau, 1997) was selected for implementation in this second investigation. This model included the same four dimensions as Whare Tapa Wha, but it also included a new fifth dimension Identity-Whenua, which required students and staff to attend to and consider both their ethnic and cultural identities.
The new ethnic and cultural lenses of the Whare Tapa Rima-the Five-Sided Home Model, led to the provision of new ethnic and cultural supports for student learning and wellbeing, and consideration of personal ethnic and cultural perspectives. Despite the second investigation being affected by COVID-19 lockdowns, staff developed innovative ways to continue providing the holistic support they had planned. The second model proved more effective in achieving the staff objectives to increase program completions, credit achievements, and retention rates, and reduce withdrawals, and terminations. The eventual level of objective achievement was especially surprising to the researchers given the interruptions and even more diverse staff and students involved. This second investigation was again partially funded by a national grant and published (Fielden et al., 2020a; 2020b)
The initial investigations pursued the location and implementation of evidence-based wellbeing models that could empower research participants to be more effective in achieving their stated objectives. In 2023, Stevenson et al., stated that their program of wellbeing research had changed to include ‘a long-term vision to build a robust underpinning philosophy and theory base for wellbeing research and practice that would progress and become more effective over time’ (p.104). The outcomes of the case study impact evaluation that led to the research program vision change however were not reported.
Methodology
The case study impact evaluation method was selected to identify the value and impacts of the two investigations over time. The evaluation included the following phases (1) identification of sub themes emerging from responses to the questions posed with both 2011, and 2020 participants, (2) triangulation of the sub themes identified in (1) (McLeod, 2024; Patton, 1990); then (3) synthesis of the triangulated themes in 2), to produce the final themes in order to respond to the three evaluation questions posed, and to identify further insights into the value and impact of participation in the original investigation programs over time.
This method was selected to identify the value and impacts on the students, teaching/researcher, and professional pastoral care/wellbeing practitioners involved. While this method is associated strongly with evaluating large-scale, and global development initiatives. Its inception is credited to the World Bank (Bamberger, et al., 2010; Legovini, 2010; Gertler et al., 2011; Ma & Agnew, 2022). Other evaluators are also utilising this method (Gattenhof, 2024). This evaluation method was selected due to its capacity to assess (a) the value of the models and participation in the investigations, (b) the impact of both intended and unintended experiences on participants, and (c) the overall impact on research participants’ perspectives on solving student wellbeing support challenges over time.
A further reason for selecting this method was its capacity to extrapolate what might have or could have continued to happen had the evaluation not occurred. The researchers conducted the case study impact evaluation because they recognised that conventional quantitative reporting, while addressing research questions and meeting funders’ requirements (Schofield et al., 2011; Fielden et al., 2020a & 2020b), failed to articulate or give voice to the rich and significant contributions of the three groups who participated in the previous investigations.
The case study impact evaluation design included the thematic analysis (Braun et al., 2019; Creswell & Clark, 2007; Creswell, 2009; Terry & Hayfield, 2021; Trainor & Bundon, 2021), of questionnaires, interviews, and focus group data gathered from research participants after each of the investigations. The first investigation was completed in 2011 and the second in 2020. Open-ended questions (Scriven, 1991) were asked, and interactive and iterative dialogues were undertaken to respond to the impact evaluation style questions posed that focussed largely on student support practice advances as discussed by Bledsoe and Graham (2005).
Participants
A total of 120 people participated in the two original investigations conducted. In 2011 they included the following: indigenous Māori (from diverse tribes), Pacific Island (from sixteen different nations) and those with English as a second language migrant students (N = 30), teaching/research (N = 5) and pastoral care/wellbeing practitioner staff (N = 5).
In 2020, participants included international students (N = 60), teaching/research (N = 10), and professional pastoral care/wellbeing practitioner staff (N = 10). After dissemination of email and telephone invitations to participate in the impact evaluation, 108 of the original investigations’ participants consented to participate. All were invited to respond to the impact evaluation questions posed and did so through (a) face to face groups (N = 81) or individual meetings (N = 3) or (b) via telephone (N = 5), or online meetings (N = 19). After these data gathering processes, the outcomes of the thematic data analysis conducted were reported back to participants for correction or comment. Seventeen participants provided feedback. All comments received were supportive of the research and the researchers, and no corrections were requested. This participant feedback was reported back, and a further invitation to feedback/contribute to ongoing dialogue about it provided.
Those participating were encouraged to draw retrospectively on their reflections on and in action (Schön, 1983) during the investigation experiences. Researchers collectively subjected all the evaluative data to thematic analysis to address the three evaluation questions posed. They also identified findings about whether intended outcomes were achieved and whether unintended consequences emerged over time (Patton & Campbell-Patton, 2021).
Wenger-Trayner and Wenger-Trayner’s (2020, 2021) writings on value creation and the recognition of social aspects in knowledge creation and sharing also informed the method design. They included dialogues, korero-talk, and talanoa-conversations within the participant groups to acknowledge the contributions of these social processes.
Impact Evaluation Questions
The three case study impact evaluation questions posed were as follows: (a) What value did the wellbeing model Whare Tapa Wha or Whare Tapa Rima contribute to the research participants? (b) What was the intended and unintended impact of Whare Tapa Wha or Whare Tapa Rima on the research participants? (c) What impact did implementation of Whare Tapa Wha or Whare Tapa Rima have on research participants’ views on solving wellbeing support challenges over time?
Ethics Approval
The case study impact evaluation received ethical approval from the New Zealand Career College (NZCC 1-18-1-2008), and New Zealand Curriculum Design Institute (NZCDI-1-17-8-2018) with Māori and Pacific Island Advisory Group support.
Findings
Phase One – Thematic Analysis Findings
Sub themes emerging from research participant responses to evaluation questions: (a) What value did the implemented wellbeing model Whare Tapa Wha and Whare Tapa Rima contribute to research participants? (b) what was the impact of implementation of Whare Tapa Wha and Whare Tapa Rima both intended and unintended on research participants?
Phase One: 2011 Questions (a) and (b) Sub Theme Summaries (Model implemented was Whare Tapa Wha - WTW)
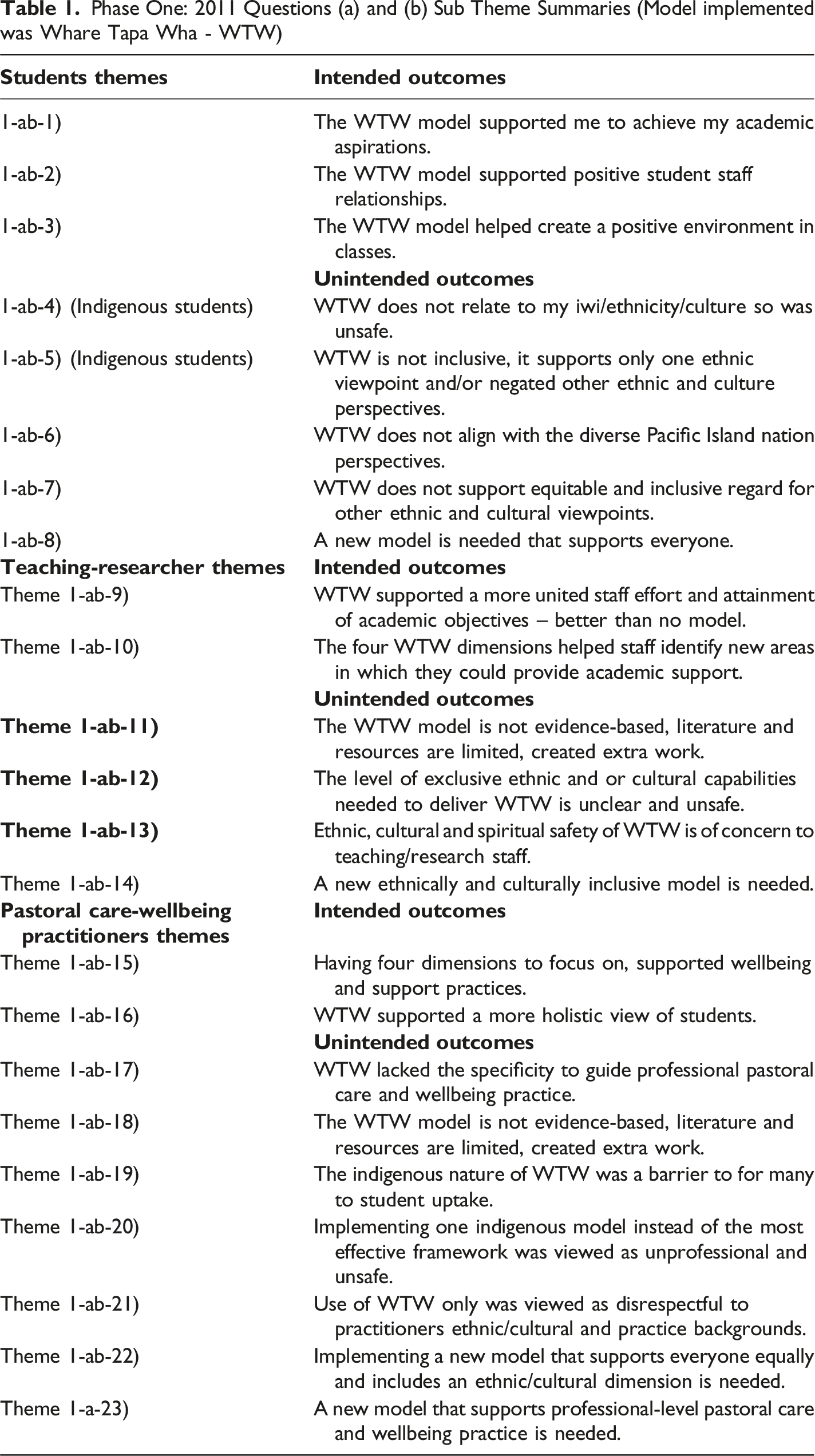
Table 1 shows the outcomes of the thematic analysis of all evaluative data gathered in 2011 about the Whare Tapa Wha model implementation related to evaluation questions. The analysis identified 7 intended and 16 unintended outcome sub themes.
Changes between the 2011 and 2020 model implementation included (i) a change from using the Whare Tapa Wha - Four-Sided House model to the Whare Tapa Rima – Five-Sided Home model, (ii) the change from a largely indigenous/Pacific Island student population in 2011 to a highly diverse student population in 2020, (iii) the shift from implementation of a wellbeing literacy approach to a more extensive whole of organisation approach in 2020 that included all teaching/research and pastoral care and wellbeing staff.
Table 2 shows the outcomes of the thematic analysis of all evaluative data gathered in 2020 about the Whare Tapa Rima - Five-Sided Home Model implementation related to evaluation questions: (a) What value did the implementation of the wellbeing models Whare Tapa Wha - Four-Sided House or Whare Tapa Rima-Five-Sided Home Model contribute to the research participants? (b) What was the impact of Whare Tapa Wha-Four-Sided House Model or Whare Tapa Rima-Five-Sided Home Model implementation – both intended and unintended – on the research participants in the investigations? Phase 1: 2020 Questions (a) and (b) Sub Theme Summaries (Model implemented was Whare Tapa Rima - WTR)
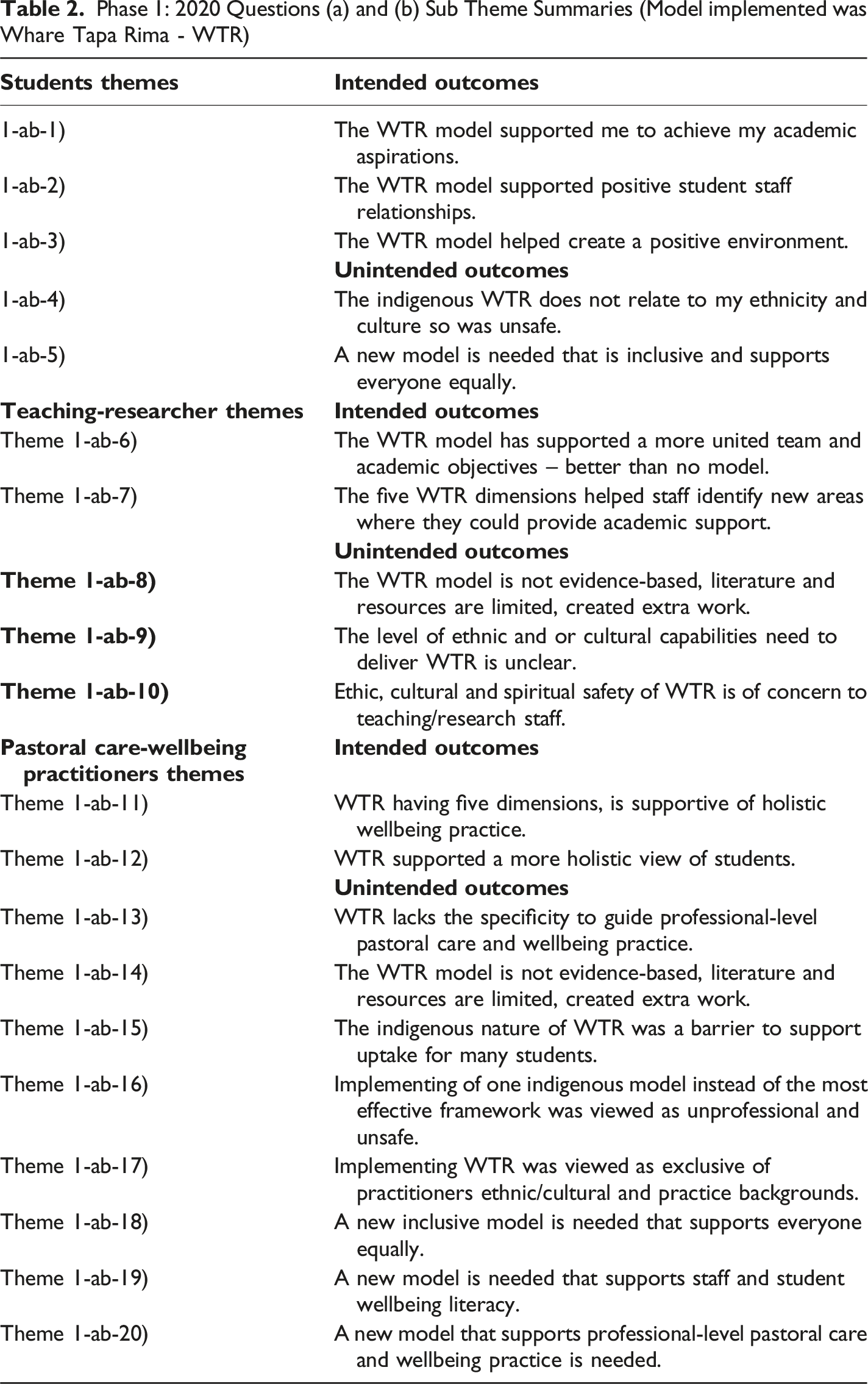
The thematic analysis identified 7 intended and 13 unintended outcome sub themes.
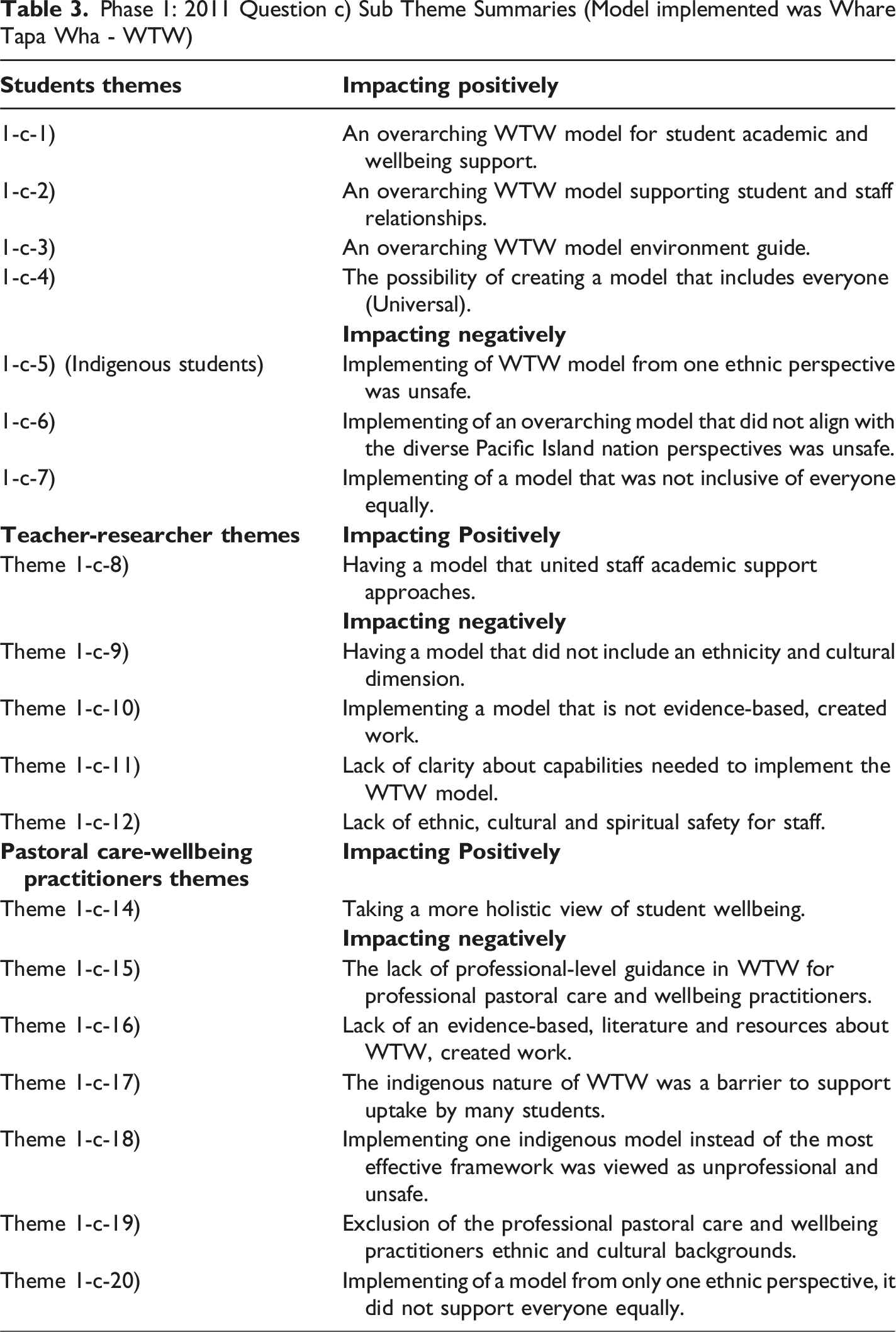
Phase 1: 2011 Question c) Sub Theme Summaries (Model implemented was Whare Tapa Wha - WTW)
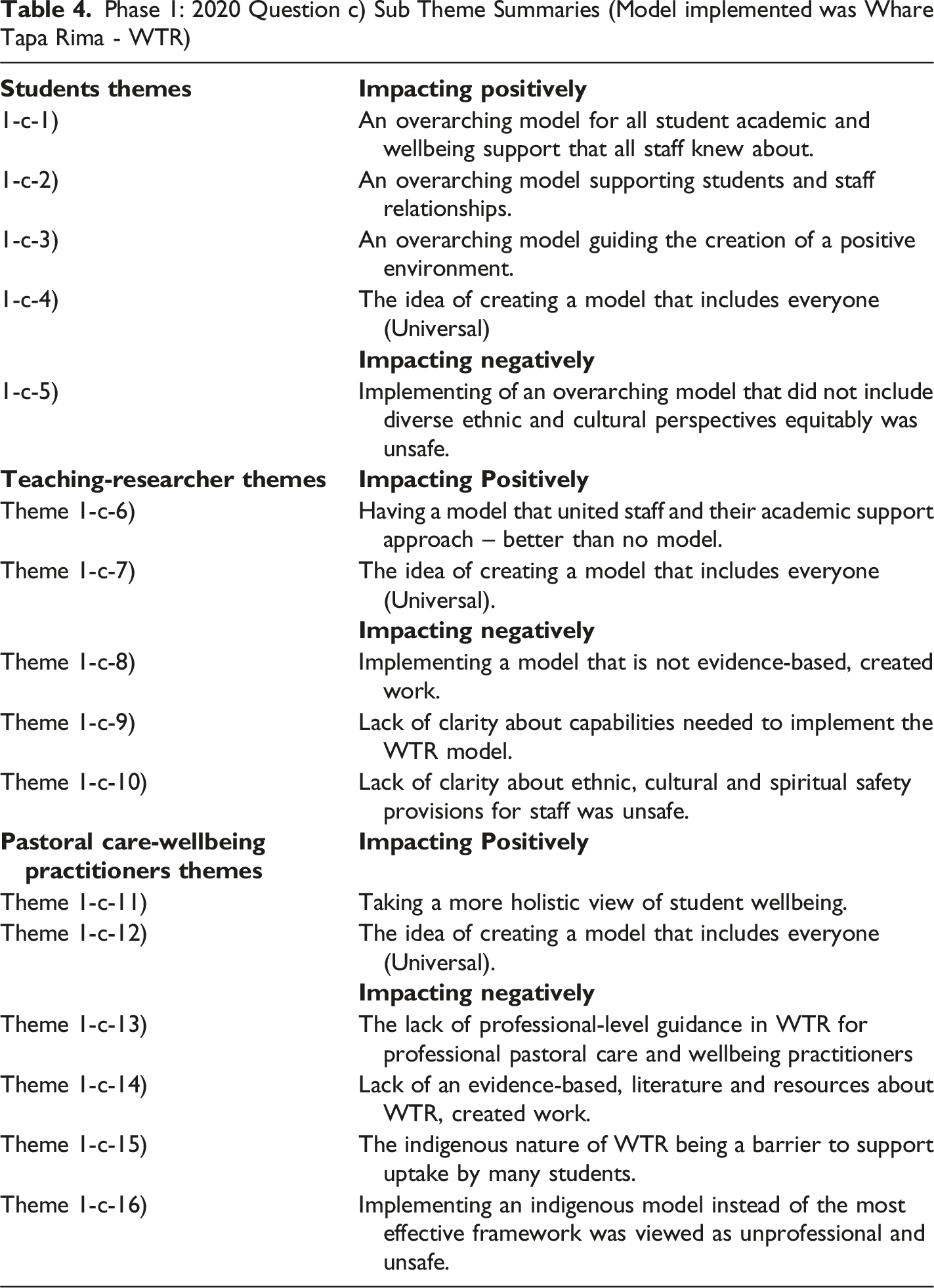
Phase 1: 2020 Question c) Sub Theme Summaries (Model implemented was Whare Tapa Rima - WTR)
Phase Two – Triangulation
Triangulation of Themes Addressing Questions a) and b)
Phase Two: Final themes emerging from the triangulation of 2011 and 2020 evaluation questions (a) and (b) data
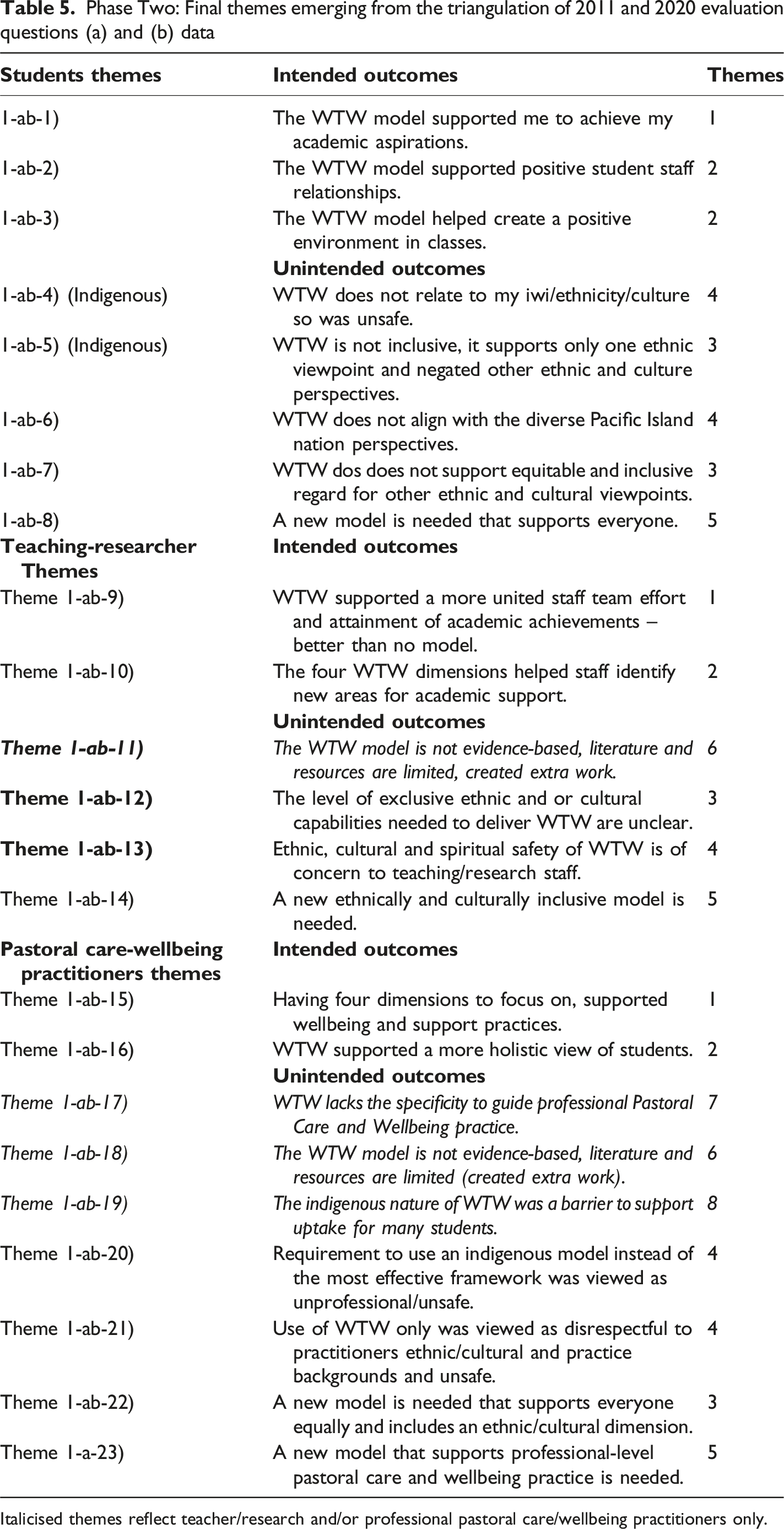
Italicised themes reflect teacher/research and/or professional pastoral care/wellbeing practitioners only.
Phase Two – Triangulation
Triangulation of Themes Addressing Question c)
Phase Two: Final triangulation themes emerging from the triangulation of 2011 and 2020 evaluation question c) data
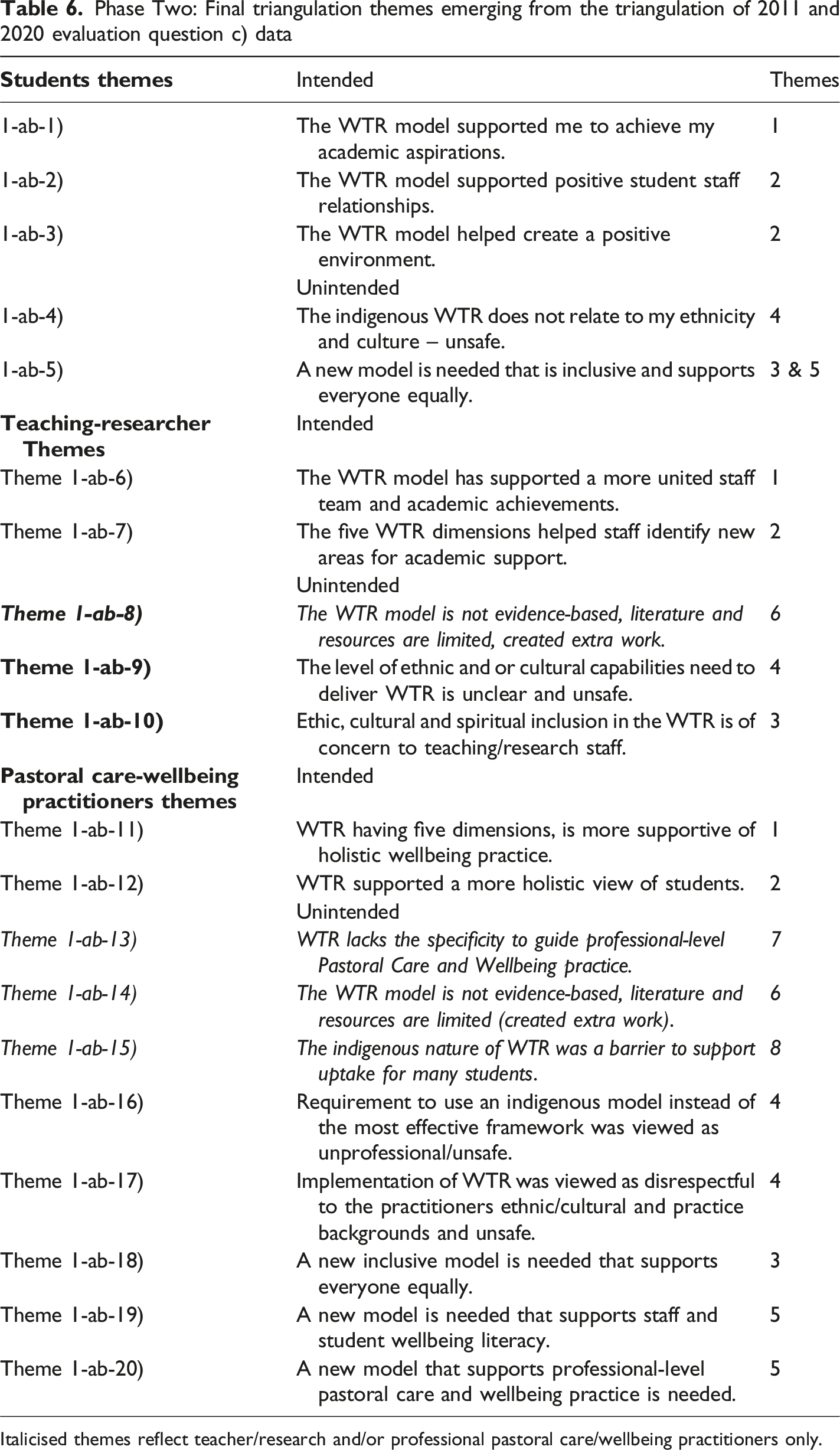
Italicised themes reflect teacher/research and/or professional pastoral care/wellbeing practitioners only.
Phase Three – Synthesis
A synthesis of the themes that emerged from the triangulation process is set out in Tables 5 and 6. The triangulated themes show the synergy between the three groups participating in the case study impact evaluation and their responses to evaluation questions (a), (b) ( Table 5) and (c) (Table 6). The final themes emerging from responses to questions (a) and (b) show a high level of agreement despite the implementation of two different wellbeing models in 2011 and 2020. In 2011, 7 intended themes were identified, and 16 unintended themes.
In 2020 when the Whare Tapa Rima model was implemented; the number themes were the same but in 2020 but the number of unintended themes was reduced by 3 indicating this model had fewer Unintended outcomes than the Whare Tapa Wha-Four-Sided House Model used in 2011. The 3 unintended outcomes disappearing related to a lack of inclusiveness, and support for different ethnic and cultural perspectives for the participating students, and the reduction of one similar unintended consequence for teachers/researchers. There was however an increase of 1 in the Unintended outcomes experienced by the pastoral care/wellbeing practitioners, relating to the need for more specific wellbeing literacy support from the model used.
The final themes emerging from responses to question (c) What impact did implementation of the Whare Tapa Wha-Four-Sided House Model or Whare Tapa Rima-Five-sided Home Model have on students, teaching/research staff, and professional pastoral care/wellbeing practitioner views have on solving wellbeing support challenges over time? Are less similar. In 2011, 6 intended themes were identified across the groups and 14 unintended themes. In 2020 the year the Whare Tapa Rima-Five-Sided Home Model was implemented the number of intended impacts increased by 2 themes to 8 and the unintended impacts decreased from 14 to 8 themes again indicating there were fewer Unintended impacts with the Whare Tapa Rima-Five-Sided Home Model implemented in 2020.
The above synthesis supports the view that the Whare Tapa Rima-Five-Sided Home Model implemented in 2020 was viewed as being both more valuable and having more impact over time than the Whare Tapa Wha-Four-Sided House Model implemented. The implementation of a model that included Wairua-Ethnicity/Cultural identity dimensions was more effective. This finding is also supported by the past student program completion achievement rates. Other factors possibly influencing the above findings were the more diverse teaching/research and professional pastoral care/wellbeing practitioner staff involved and the different 2011 and 2020 student population profiles.
Five final themes emerged from the theme triangulation process (see Tables 5 and 6) and were supported in both 2011 and 2020 by all three participant groups, see below:
Intended Outcomes
Theme One – Achievement Supporting
This final theme recognised that the model implemented in both 2011 and 2020 added value for all three participant groups in terms of their efforts to improve program completions.
Illustrative Quotes
Student – ‘Whare Tapa Wha helped me to learn differently, it’s not just as head stuff’ (P-5-2011)
Teacher/Researcher – ‘The model helped me to look at new things impacting student learning’ (P-2-2020)
Pastoral Care/Wellbeing Practitioner – ‘Thinking about the students more holistically was helpful, some had hugely challenging past experiences’ (P-10-2020)
Theme Two – Relationship and Environment Supporting
This final theme recognised both models implemented added value for all three evaluation groups by improving relationships and the environment for all involved.
Illustrative Quotes
Student – ‘The staff are great, and the atmosphere is positive. I think the model helps that’ (P-10-2011)
Teacher/Researcher – ‘The model helped me to consider new things that might be impacting my student’s learning’ (P-5-2020)
Pastoral Care/Wellbeing Practitioner – ‘Everyone understanding Whare Tapa Rima helped us to collectively create a more positive and caring student environment’ (P-1-2020)
Unintended Outcomes
Theme Three – Not Inclusive
This final theme recognised that both models were perceived as not being inclusive and having negative unintended outcomes for all in terms of efforts to improve student learning.
Illustrative Quotes
Student – ‘The creator of this model is not from my iwi, we have a better model, I can’t relate to this model’ (P-1-2011)
Teacher/Researcher – ‘The model looking at the world from one ethnic/cultural perspective was problematic for many, I think we all felt excluded to some extent’ (P-3-2011)
Pastoral Care/Wellbeing Practitioner – ‘I migrated to NZ and never expected after all I had heard about New Zealand that the country might not welcome and want to use my expertise and training, I felt like I/me was not genuinely welcome. It was very upsetting’. (P-8-2020)
Theme Four – Not Safe
This final theme recognised that both the models implemented were perceived as not ethnically, culturally, intellectually or spiritually safe and had negative unintended outcomes for all three groups in terms of supporting efforts to improve student program completions.
Illustrative Quotes
Student – ‘I’m a Christian and the Ten Commandments require us not to put any other God before ours, I don’t feel spiritually safe with the Māori idea of Wairua’ (P-8-2020)
Teacher/Researcher – ‘The teaching/research team have not been able to get any clarity about the level of understanding we need to have to implement a Māori model, even the Māori Advisory Board can’t agree, it’s frustrating, I feel unsafe using a Māori model’ (P-9-2011)
Pastoral Care/Wellbeing Practitioner – ‘I never thought all my years of clinical education could be sidelined by a model that has no evidence, or resources, it’s offensive and puts us all in an unsafe place. Some students have not come for help when they needed to because, despite all our efforts, they think a service named in a particular language is only for the people who use that language, this situation is dangerous for some students’ (P-4-2011)
Underpinning for the teaching/researcher and professional pastoral care/wellbeing practitioners were their professional ethical requirements to (a) do no harm, (b) equitably support access to student services, and (c) provide inclusive and safe services. Feedback received demonstrated that many staff believed they could not fully and inclusively practice their ethical principles using the indigenous models implemented, for many this left them facing a challenging ethical dilemma. Should they continue using one ethnicity/culturally based model if they believed it was unethical on safety grounds to do so?
Theme Five – New Model Needed
This final theme recognised that evaluation participants viewed the location or creation of a new model as being needed to support student learning/program completions.
Illustrative Quotes
Student – ‘We need a model that everyone can relate to, something that is Universal, people are people’ (P-24-2020)
Teacher/Researcher – ‘The model we’ve used has problems, we need an inclusive model that supports everyone, the model we’ve used needs huge development’ (P-10-2020)
Pastoral Care/Wellbeing Practitioner – ‘The model does not support all students. In my role, I have to support everyone who comes for help equally. I think we need a new professional-level model that supports our practice in detail, not a public health model. The model needs to include things people can change themselves, it needs to be strength-based and empower students’ (P-5-2011)
Participants from all three evaluation groups in both 2011, and 2020 stated a new model was needed. Diverse participants in both 2011 and 2020 suggested it be ‘Universal’.
Teaching/Researcher and Pastoral Care/Wellbeing Practitioner Only Theme
Theme Six – Absence of an Evidence Base and Specificity
A common final theme in both 2011 and 2020 was a professional concern about the lack of an evidence-base, literature and resources about the model being implemented and the inability of these models to support practice advances. Note this final theme also recurs in the Pastoral Care/Wellbeing Practitioner summary below.
Illustrative Quote
‘The lack of an evidence base, and resources to support the model is a real problem, it means we have to fill these gaps and creates a lot more work at an already challenging coal face, I can’t believe we use this in the national curriculum and that teachers have so little to support their students and practice’ (P-8-2011).
Theme Seven – The Barrier Effect
A common final theme was the barrier effect reported; it involved students not seeking support because they thought the indigenously named support services were for students of that ethnicity only.
Illustrative Quote
‘A model with an indigenous name looks like it’s only for students from that ethnic group, it puts other students off seeking help, which could be dangerous, I’ve had students at risk of violence and suicide put off getting support, we can’t have that’ (P-9-2020).
The use of an indigenous name only made the challenges of communicating to all students that there were support services available to them more difficult. These concerns escalated with the more diverse student population in 2020. Concerns remained high about the exclusive appearance of the models/support services despite name translations and a range of activities designed to encourage all students to use the services in 2011 and 2020.
Pastoral Care/Wellbeing Practitioner Only Themes
Theme Six – Absence of an Evidence Base and Specificity
Emerging again this final theme emerged from Practitioners in both 2011 and 2020 expressed consistent concern about the capacity of the model they experienced to shed light on: what exactly wellbeing is, how it is influenced it, and how all students can be empowered (with their support) to implement such wellbeing literacy understandings. They also voiced the need for a professional-level model to guide and advance their student support practice.
Theme 8 – Use of One Indigenous Model
The final theme emerging from the professional pastoral care and wellbeing practitioners working at the ‘coal face’ of student support services related to ongoing challenges trying to use one indigenous model to guide their practice with diverse students. The practitioners questioned whether the use of one indigenous model was the most inclusive, effective, and appropriate way to work with the diverse students they encountered. They experienced the need for the flexibility and space to customise and employ the most suitable model(s) to frame their practice as they worked with diverse students with complex challenges.
Many expressed the view that an indigenous model could help some students, while other students might benefit more from a different indigenous model such as Te Wheke (Pere, 1982, 1988, 1991), or from models like the Fale Fono (Fuimaono, 2021), the Koran-based model (Hassan, 2015), or other more universal or clinical frameworks, which might offer greater value, impact, and effectiveness in practice.
Discussion
Emanating from the above synthesis was a clear answer to evaluation question (a) what value did implementation of the wellbeing model Whare Tapa Wha-Four-Sided House Model or Whare Tapa Rima-Five-Sided Home Model contribute to the research participants? The final themes show that implementation of wellbeing models was regarded as being of value by all three participant groups in both 2011 and 2020. Areas where the models were regarded as adding positive value for all parties were related to (i) supporting student learning and program completions, (ii) positive student/staff, and staff/staff relations and (iii) a positive learning-supporting environment.
Final themes were more diverse about evaluation question (b) what was the impact of implementation of Whare Tapa Wha or Whare Tapa Rima both intended and unintended on the research participants in the investigations? The Intended and positive outcomes of the models are captured in Table 6. Participants’ responses from all three groups reflected in detail the positive impact both models used in 2011 and 2020 had on students learning/program completions, relationships and the learning environment. The level of positive impact was higher in 2020 when the Whare Tapa Rima-Five-Sided Home Model (Moeau, 1997) was implemented.
Responses revealed that participants from the three groups considered the Whare Tapa Rima-Five-Sided House Model more inclusive than the Whare Tapa Wha-Four-Sided House Model their key reason for this view was its inclusion of a Whenua-Ethnic and Cultural Identity component. Another reason this model has a higher level of support despite the student population in 2020 being significantly more diverse than in 2011 was the whole of institutional approach implementation which included the higher-level involvement of staff.
Staff provided a higher level of involvement in the whole institutional approach, which helped the model gain more support – even as the student population in 2020 grew significantly more diverse than in 2011.
Final theme findings related to unintended impacts which included the negative and are more complex.
Two final themes emerged reflecting negative and unintended impacts associated with the implementation of the models. Firstly, most participants in all groups reported experiences of thinking, being, and feeling excluded or not being included. Responses showed some regarded the use of the indigenous language model names (though also provided in English) as flagging an exclusive by Māori for Māori perspective.
Indigenous and non-indigenous students, teaching and research staff, as well as pastoral care and wellbeing practitioners, actively expressed their negative experiences with the indigenous wellbeing models. They voiced particular concern about the potential for harm and exclusion affecting others in the learning community.
While many stated that the implementation of a model was ‘better than no model,’ both models were viewed as being exclusive of students and staff on ethnic, cultural, intellectual, and spiritual grounds and this was regarded as unacceptable on iwi, spiritual, ethnic, cultural, ethical, intellectual, and professional grounds. The impact of the above perceptions was negative, Unintended and unexpected, the impact of this theme was serious and according to recent more holistic understandings of the ethical ‘do no harm principle’ which includes the physical, psychological, emotional, economic, reputational and legal (Gençten, 2021); harm was clearly experienced by some participants. The second Unintended outcome final theme related to participants’ safety. The impact of this theme was also serious, included all groups and was also found to be harmful (as described above) to some participants. Participants’ responses revealed negative impacts in all groups relating to ethnic, cultural, spiritual, professional, intellectual, and ethical safety.
Students, staff and researchers, along with wellbeing practitioners, shared in focus group discussions that while some indigenous students resonated with the models, others did not support them due to differing iwi-tribal links. Many other students, teaching/research staff, and pastoral care/wellbeing practitioners also withheld support for the models.
The indigenous models were unsuccessful in meeting the diverse Pacific Island students’ needs, many of whom could not relate to a wellbeing model that did not include a Christian spiritual element. Other diverse students also questioned if the models were (i) ethnically, culturally, intellectually, and spiritually appropriate; (ii) the level of understanding of the indigenous models required, and (iii) exactly who the model was intended to support, and if it was genuinely inclusive of all students and staff.
While holistic safety had been a consideration from the outset of the research investigations and appropriate ethical permissions had been gained; this evaluation exposes major inadequacies in initial ethical considerations in two key areas. Firstly, the ethical considerations did not holistically consider ethical principles, as described by Gençten (2021). For example, they did not consider spiritual, ethnic, intellectual, and cultural dimensions of safety in detail, and secondly, they did not equitably examine the safety of the teaching/research, and pastoral care/wellbeing practitioners, or their personal, intellectual, professional ethical obligations alongside the safety of the students.
When discussing ethnic and cultural responsiveness, most people in teaching and research focus on how to proactively address the emerging needs of those they work with. Indigenous Allied Health Australia (2019) emphasises that true responsiveness involves actively pursuing systematic change. In contrast, achieving ethnic and cultural competency requires individuals to actively acquire knowledge, skills, beliefs, values, and understandings (Frawley et al., 2020). This process is lengthy and often unrealistic for those who work daily with students from a wide range of ethnic and cultural backgrounds.
The approach selected during the investigations was that of ethnic/cultural safety as described by Ramsden (2002).
Ramsden stated that ‘In particular, Māori models of health need to apply to reality just as any other model should’ and that ‘they are not an ancient whakatauki-understandings’ (p.105). She further advocated for Māori health models to advance for them to be considered in such matters as poor education, as occurred in both investigations now being evaluated. Ramsden’s view of safety placed an obligation on the teachers/researchers and pastoral care/wellbeing practitioners to provide student support within a framework that recognised and respected their differences. Her view also notes that it is not for staff or professionals to determine what is safe but the place of the student/client, or patient who was the subject of the support, and indicated that at the base of safe interactions was the building of and presence of trust.
The view of ethnic/cultural safety that emerged from Ramsden’s work gives primacy to the student/client, or patient who is the subject of the support. The unexpected and negative themes related to exclusion and safety emerging in this case study impact evaluation however raise troubling questions about whether consideration of the recipient of the support services alone is adequate. For example: • Is the relationship between adult students, teachers/researchers and pastoral care/wellbeing practitioners hierarchical, or equitable? • Might all three participant groups need to be kept safe, or is it acceptable for the professionals providing support to be made unsafe by a workplace requirement to use a specific ethnic or cultural model in their practice? • Might such professionals have a right to appropriate education before such a requirement is made? And • Do teachers/researchers, and pastoral care/wellbeing practitioners have a right to ethnic/cultural/spiritual and intellectual safety in their workplace?
The unintended final themes identified in this case study impact evaluation highlight both harms and barriers to the building of trusted relationships between students, teachers/researchers, and professional pastoral care/wellbeing practitioners. Kearns (1997) seems to identify a way forward when advocating that there should always be a legitimate space for negotiation between those being supported and those providing support that is cognisant and respectful of power imbalances. The themes that have emerged point to all three participant groups being caught in a state of what Land (2011), refers to as liminality where they are ‘betwixt and between’ what they know and their familiar ethnic, cultural, spiritual, ethical, intellectual, and professional ways of operating in the world and any new ones they meet such as models from another ethnic/cultural reality.
The participants proposed a solution to the above negative and unintended outcomes in their responses to evaluation question ( c) what impact did the implementation of Whare Tapa Wha-Four-Sided House Model or Whare Tapa Rima-Five-Sided Home Model have on students, teaching/research staff, and professional pastoral care/wellbeing practitioner views on solving wellbeing support challenges overtime? The final theme emerging from the triangulation of evaluation themes and supported by all evaluation groups was the need to locate or create a new wellbeing model without the negative and unintended outcomes identified.
While some researchers elect to interpret findings in different ways, and for different or political purposes, the authors of this paper have sought to disseminate the views and voices of those participating as directly as possible and without filters, hence the inclusion of so many quotes.
The conclusions reached and reported have been informed or are directly those of the participants: students (these are identified in the paper), the teaching/research staff, and the pastoral care and wellbeing/clinical staff. All the above participant groups have included Māori, Pacific Island, and diverse ethnic and cultural others.
Participants provided feedback, which the paper then triangulates to demonstrate both the synergy in perspectives and the areas where views diverged.
Note also the findings have also been during the first, second and impact evaluation reviewed and their interpretations advised on by three different Institutional Māori and Pacific Island Advisory Boards who guided the researcher’s interpretations and reporting.
The new model suggested has now been developed through a multi-year research program and the researchers have moved from a state of being ‘betwixt and between’ to a clear four component Universal Wellbeing Model which was published first in 2023 (Stevenson et al.). This new model, whose name was suggested by some of the participants in this investigation, has been well received and is now being increasingly widely disseminated and implemented. Furthermore, publications on the research underpinning this new model, and its implementation are being published as completed to increase Universal Wellbeing Literacy and resources for professional Pastoral Care and Wellbeing practitioners and other researchers.
Finally, we acknowledge that like many before them the research participants who implemented the indigenous wellbeing models did so from a genuine desire to improve student program completion rates and equity levels. The method they selected for achieving this was very much influenced by the social, and political environment of the day, and was retrospectively naïve. Awareness of the differences and synergies between the research participant groups were not apparent before this case study impact evaluation. As Wenger-Trayner and Wenger-Trayner (2020, 2021) state, however, empathetic understandings and learning unfold from the iterative dialogues within, and between those involved, and they resulted in a high level of consensus and support for the themes and conclusions that appeared.
Conclusion
In conclusion, this case study impact evaluation showed that as well as the models implemented contributing as intended to the achievement of nationally outstanding program completion rates (2011 – 87%) and (2020 – 98%) plus student learning, relationships and the learning environment, they also resulted in unintended and harmful outcomes. The two key areas where unintended and harmful outcomes were revealed relate to exclusion and a lack of safety for those in the three participating groups. As Petrosini et al. (2020) warned, transformative approaches can have unintended and harmful effects. This Case Study Impact Evaluation also identified a final theme that pointed to finding a better way forward.
The evaluators learnt critical lessons, firstly, as Winkler (2023) said ‘assumptions are the termites of relationships,’ in other words, the making of unexamined assumptions and following these is dangerous and can lead to serious harmful consequences for relationships between those who aim to support and those to whom support is provided. Two assumptions were made by the researchers at the outset of the initial investigations conducted. The first was assuming implementing an indigenous wellbeing model would be the best way to improve indigenous and other students learning and program completions. They were encouraged to take this view by the inclusion of their initially selected model in New Zealand’s national Health and Physical education curricula.
The researchers were surprised however to find that the model was not an evidence-based choice, and there was virtually no literature, resources, or guidelines available about the capabilities needed by those who might implement this model. A second assumption made was that the appearance of the wellbeing models (especially Whare Tapa Wha-Four-Sided House) in the above curricula suggested their appropriateness for use in an educational context. Further examinations found instead that the model was Public Health, ecological/whole of society orientated and not fit for underpinning student empowerment orientated supports and services. That is, these models did not explain what wellbeing is, how it is influenced or specify how individuals could make changes to improve their wellbeing in a professional and practice-supported manner. The misalignment between the Public Health orientated models selected and the educational purposes for which one was sought, that is, student empowerment could not be reconciled at a professional-level.
The final theme emerging from the triangulation process was the new model need. This theme prompted actions by the evaluators and researchers. Initially, they embarked on an extensive global and multi-disciplinary theory review to locate evidence-based wellbeing models. Encountering little success in this endeavour, and after time and reflection, they commenced the complex and daunting process of creating a new theoretical wellbeing model that would be evidence-based, fit for purpose, and without the unintended and harmful outcomes identified.
To ensure the success of any new wellbeing model, it must clearly define wellbeing, identify its influencing factors, and empower people to enhance their own wellbeing and prevent the often dire consequences of poor wellbeing outcomes.
Requirements of the new model were that it be: - Evidence-based - Supported by a body of research and evaluation - Inclusive - Holistically safe - Guide high level and practice advances and - Include flexibility in the way it was applied so that it could be combined with other models, frameworks and perspectives as and when appropriate.
Three terminological developments also emerged from this case study impact evaluation. Supported was terminology already in draft form, (i) ethnicity is genetically (DNA) determined and therefore largely unchangeable, (ii) culture may be dynamic and includes all selected aspects of a person’s lifestyle, (iii) wellbeing that was often shown historically with a hyphen due to its initial psychology/medicine field base and use of the APA referencing, was dispensed with as the evaluators sought to advance a authentically holistic, inclusive, and multi-disciplinary evidence-based wellbeing concept, and finally, (iv) the concept of Universal Wellbeing was born, and work in its definition and precise theoretical form commenced.
While it is possible that the findings emerging could be viewed as unpopular opinions Kierstead (2024), facing wicked problems (Tsey, 2019), they are underpinned by an iterative 15-year wellbeing research and evaluation program from which new knowledge and practices are emerging like a 3D item from a printer. The items emerging are valuable in terms of their impact, support to theorising, and significance to professional wellbeing practice (Habermas, 1987). Had this case study impact evaluation not been undertaken those working in student support nationally and globally might never have had cause to re-examine the potential unintended and harmful impacts of the models they elected to use on both their students and clients or on the staff providing these supports. Other researchers such as Petrosino et al., 2000, have also identified wellbeing programmes that have been harmful. Further research, evaluation and debate are needed about whether equity can or is achieved when implementing it through a pathway that simply brings forth new inequities or harm to others.
Finally, this case study impact evaluation has ensured the ethnic and cultural perspectives of all three participant groups have had a cathartic, and catalytic effect on the Universal Wellbeing Model development journey. Without these findings, it is unlikely a new wellbeing model would have emerged with the positive intended outcomes, and without the unintended and harmful outcomes identified. For those engaged in a practice that supports the wellbeing of others, this evaluation marks a seismic shift in prevention-orientated wellbeing thinking and actions being conducted in higher education and many diverse settings and with many diverse recipients and providers of that support.
‘If we try to secure the wellbeing of others, we will, at the same time create the conditions for our own’. (Dalai Lama, nd)
Acknowledgements
The authors wish to express a special thanks to those attending the Herdsa Conference 2024 Work-in-Progress Round Table which focussed on: sharing work-in-progress and seeking feedback and input with the view of shaping, refining and progressing the findings detailed in this article. The publication of this article is due in no small part to their enouragement and support.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Further Research and Evaluation
Further research and evaluations are currently underway to report on the completion, and implementation of the Universal Wellbeing Model that has emerged in education, health, community, business and other settings (Stevenson et al., 2023).