
Abstract
Objective:
The aim of this study was to explore the views of women diagnosed with a mood disorder about children, medication and pregnancy.
Method:
Female patients from the Black Dog Institute were invited to complete a questionnaire regarding their views about pregnancy, children and medication during pregnancy. Diagnostic groupings were derived by assessing DSM-IV criteria for mood disorders. Unipolar and bipolar patient responses were analysed to determine any differences between groups.
Results:
Women with bipolar disorder were more concerned than those with a unipolar condition about the impact pregnancy would have on their mood, as well as the potential for their offspring to inherit a mood condition. Both groups of women expressed concerns regarding the child-rearing environment, and stated that knowing the risk their child could have of developing a mood disorder would encourage them to be more vigilant parents.
Conclusion:
While both groups were concerned about the environment in which they would raise their child and wanted to be vigilant parents, women diagnosed with a bipolar condition expressed stronger opinions regarding the impact that their pregnancy could have on their mood disorder, and passing the mood disorder onto their children.
Bipolar disorder and depression are common in Australian women, with lifetime prevalence rates estimated at 2.7% and 14.5% respectively. 1 For women, the mean age of onset for depression has been calculated at 37 years, 2 compared to 18 years for bipolar disorder. 3 This means that a substantial proportion of Australian women with a mood disorder will require treatment during their reproductive years, particularly if diagnosed with a bipolar condition, given its early age of onset. Many authors have therefore suggested that the possibility of both planned and unplanned pregnancies during this time makes it necessary to educate women about the risks and realities of treating a mood disorder during pregnancy at first presentation.4–6
Being aware of how medication and mood conditions may impact on pregnancy and childbearing is of key importance due to the nature of the medications used to treat such conditions, as well as the converse risks associated with not treating a mood disorder during pregnancy. Risks associated with the use of psychotropic medications include, for example, spontaneous abortion, prematurity, neonatal discontinuation syndrome, neural tube defects, gestational diabetes and poor long term infant development. 5 However, these risks vary greatly in terms of the risk provided by differing medications, with many practitioners now holding the belief that certain medications (such as tricyclic antidepressants and lamotrigine) may be used without teratogenic effects, whilst other drugs 5 (e.g. selective serotonin reuptake inhibitors and lithium) may be considered as having manageable risks if proper monitoring is in place. 7 Despite these exceptions, the risks associated with several medications are serious and should not be discounted. For example, inappropriate dose monitoring of lithium during delivery is potentially fatal as blood and serum levels can vary dramatically at this time (see Galbally et al. 5 for a full review, and for a more detailed explanation of mood stabiliser monitoring during pregnancy, see Galbally et al. 7 ). Unfortunately, the unequivocal safety of any psychotropic drug during pregnancy is yet to be adequately demonstrated. The Australian Therapeutic Goods Administration classifies medications ‘safe’ for use during pregnancy for both mother and foetus as category A (extensively studied with no risk found), 8 yet the most commonly prescribed antidepressants are currently classified as category B2, B3 (animal models indicate risk, without clear evidence in humans) or C (suspected risk with possibly reversible effects). Most commonly prescribed mood stabilisers are categorised as C or D (suspected risk with irreversible effects). 8
Concerns about psychotropic medication use during pregnancy inevitably give rise to consideration of its discontinuation, where there is potential for harm both in relation to the high relapse rates in pregnant women who choose to discontinue medication6,9 and the impact of any such mood disorder on the final stages of pregnancy and the early post-natal period. The negative effects of untreated depressive episodes during pregnancy are severe for both mother and foetus, and include suicide, premature delivery, gestational bleeding and high foetal cortisol levels at birth. 10 In bipolar disorder, the dangers of depressive episodes are of the greatest concern, with the prevalence of a depressive or mixed state being four times greater than the prevalence of manic or hypomanic episodes. 9
Although there are large variations in the estimated heritability of mood disorders, the general consensus is that offspring of parents with a mood disorder are at an increased risk of developing a mood disorder. For example, a review conducted by DelBello & Geller 11 reported that the offspring of parents diagnosed with bipolar disorder had a 5–67% likelihood of developing a mood disorder. According to the authors, this sizeable discrepancy is primarily attributable to difficulties in diagnosing bipolar disorder in a younger sample. Heritability rates reported for offspring of parents with a unipolar disorder are more consistent, with Lieb and colleagues 12 quantifying a 32% likelihood of the child developing a mood disorder, while in the same studies,11,12 the offspring of healthy cohorts had risks of 0–25% and 14% of developing bipolar disorder or depression, respectively.
Given what is currently known about the prevalence and heritability of mood disorders, combined with the complications of drug treatment during pregnancy, the present study was devised to explore the perceptions of women with unipolar depression or bipolar disorder regarding pregnancy, medication and childbearing. Although research has been conducted into the knowledge of health professionals 13 and their opinion about medication use in pregnancy, 14 we are not aware of any previous research directly comparing the opinions of women diagnosed with a bipolar condition with women diagnosed with a unipolar condition.
Given the higher heritability rates of bipolar disorder relative to unipolar conditions, and the increased teratogenic effects of mood stabilisers relative to antidepressants, it was hypothesised that there would be distinct differences in opinions between groups of women diagnosed with unipolar and bipolar conditions.
Methods
The Sydney-based Black Dog Institute Depression Clinic provides a state-wide diagnostic and management service for patients referred by health professionals. Prior to their clinical assessment, patients were invited to complete a number of self-report questionnaires, one of which contained statements examining women’s views on pregnancy, child-rearing and mood disorders. This questionnaire comprised eight statements, with a five-point rating scale (‘Strongly Disagree’, ‘Disagree’, ‘Neither Agree nor Disagree’, ‘Agree’, ‘Strongly Agree’). Where applicable, patients were asked whether they had made the decision to discontinue their mood disorder medication whilst pregnant. All patients provided voluntary, written informed consent, as approved by the University of New South Wales Human Research Ethics Committee. Questionnaires were analysed from patients referred to the clinic over the 2008–2011 period. All patients underwent a semi-structured diagnostic interview – the Mini International Neuropsychiatric Interview (MINI), 15 assessing DSM-IV 16 criteria for mood disorders – to determine study groupings. Participants were excluded from the sample if diagnosed as having a unipolar depression with sub-threshold hypomanic episodes (defined as the presence of three or more DSM-IV [hypo]manic symptoms, that did not meet duration criteria for a ‘high’); had language or cognitive difficulties; or were under 18 years of age.
Results
Of the 1,793 patients assessed at the Black Dog Institute over the study interval, 402 (22%) completed the relevant questionnaire, were female, and met study inclusion criteria. The mean ages were 41 (SD=14) and 34 (SD=10) years for patients with unipolar and bipolar conditions, respectively. A total of 59 (15%) patients provided information on how they had approached the issue of medication during their pregnancy. Of these, 25 (42%) continued taking their mood disorder medication and 34 (58%) ceased medication during their pregnancy. The small sample size disallowed statistical comparison of unipolar and bipolar groups in terms of medication continuance during pregnancy. We examined their responses to a number of structured questions, contrasting ‘disagree’ and ‘strongly disagree’ (coded as 0) with ‘agree’ and ‘strongly agree’ (coded as 1), with neutral responses disregarded at this stage. Chi-squared tests were undertaken to examine for differences between diagnostic categories (unipolar or bipolar conditions) and responses. For differences reaching statistical significance, t tests contrasting mean responses on the original five-point scale were undertaken to determine whether diagnosis (unipolar vs. bipolar) accounted for the variation, and to quantify the size of the difference, with results detailed in Table 1.
Responses to statements about pregnancy and medication comparing women diagnosed with unipolar depression and bipolar disorder
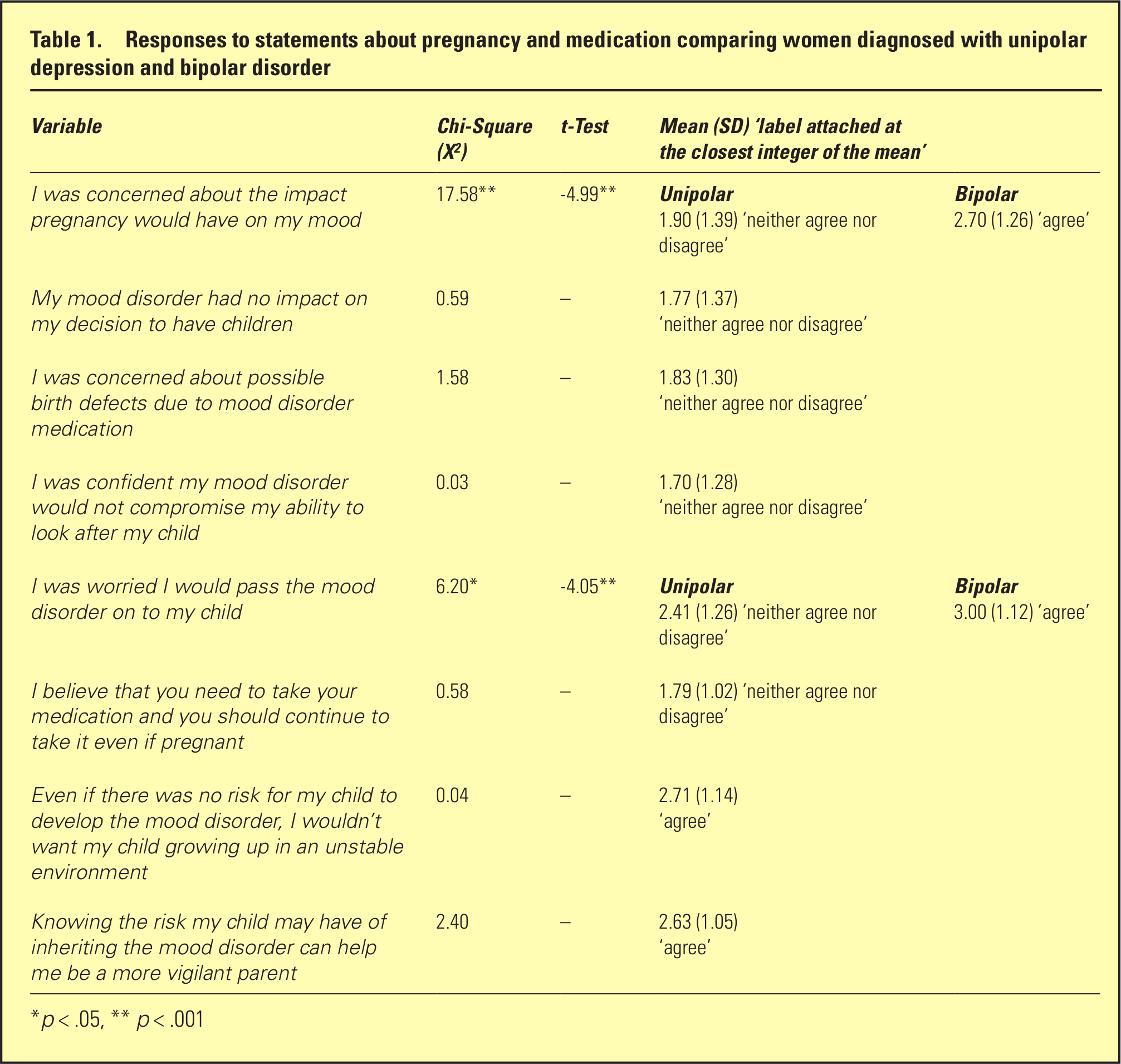
p < .05, ** p < .001
Women diagnosed with a bipolar condition were more concerned compared to women diagnosed with a unipolar condition on two items. Specifically, they were more concerned about the impact pregnancy would have on their mood, and more concerned about passing on their mood disorder to their child. Both women diagnosed with a bipolar condition and women diagnosed with a unipolar condition wanted their child to grow up in a stable environment, and indicated that knowing the risk their child could have of developing a mood disorder could help them to be more vigilant parents. Three items evoked neutral responses from both women diagnosed with bipolar disorder and women diagnosed with unipolar depression, and concerned birth defects due to medication, the impact of their mood disorder on their decision to have children and whether their mood disorder could compromise their ability to look after their child.
Discussion
This study suggests that women with bipolar disorder were more concerned regarding the impact of their mood disorder on their pregnancy and on their children compared to women with a unipolar condition. They were more likely to agree with the statement, ‘I was concerned about the impact pregnancy would have on my mood’ while women with unipolar depression were ‘neutral’ in their response. This may reflect the well-documented differential risks for women with bipolar disorder compared to women with unipolar depression, with reports quantifying relapse rates during pregnancy of 43% and 71% for women with unipolar and bipolar conditions, respectively.6,9 Alternatively this could reflect the differing role that stress (including a role change) plays in illness trajectory, with stress increasing the risk of a mood episode in bipolar disorder. 17
Additionally, these reports6,9 quantified the risk of relapse in the event of medication discontinuation during pregnancy. In women with unipolar depression who maintained their medication, 26% relapsed during pregnancy compared to 68% who discontinued their medication. The risks were greater for bipolar disorder, with 37% of women who continued their mood disorder medication experiencing a relapse compared to 85% of those who did not continue their medication. Given such findings, it is surprising to note that, while women with bipolar disorder were concerned about the impact of pregnancy on their mood, relatively neutral responses were obtained from both diagnostic groups in terms of the need to maintain mood disorder medication whilst pregnant, and about possible birth defects associated with mood disorder medication. This is reflected in the relatively equal proportions of women deciding to maintain versus discontinue their mood disorder medication. Our findings suggest that the public is relatively unaware of such literature findings.
It is unclear what proportion of women in this sample received formal counselling regarding the effects of psychotropic medication – or the potential risks associated with medication abstinence – during pregnancy. It is plausible that the neutral responses obtained reflect a lack of knowledge as opposed to a lack of opinion. The service ‘Mothersafe’ is designed to address women’s concerns about exposure to medications during pregnancy. Between 2005 and 2007, 9% of calls made to this service concerned the safety of psychotropic medications, 7.7% of which were antidepressants. 18 Clearly, many women with mood disorders are not adequately informed about their medication, again highlighting the importance of education for women prescribed mood stabilisers and antidepressants,4,5 and of services that provide up to date information for women and for managing medical practitioners.
Considering the significant heritability of mood disorders, it is interesting that responses of both diagnostic groups to the item ‘My mood disorder had no impact on my decision to have children’ were neutral. It should be noted, however, that women with bipolar disorder expressed agreement with the statement that they were worried they would pass the disorder on to their child. Given the complexities involved in such decision making – and the apparent under-recognition of risks by the public – more detailed qualitative studies would appear warranted.
A possibly encouraging finding was the emphasis women placed on engaging in attentive and vigilant parenting behaviours. In general, women with both bipolar and unipolar conditions endorsed the statement that ‘knowing the risk my child may have of inheriting a mood disorder can help me be a more vigilant parent’. This is important since vigilant, attentive parenting – in conjunction with a stable and nurturing home environment – can have an attenuating effect on a child’s risk of developing a mood disorder. 19 Such a response is assisted by organisations that work with children, parents and their families. The Post and Antenatal Depression Association (PANDA) 20 provides a national helpline for women who have depression during pregnancy, and ‘Beyondblue’ provide information and advocacy for women who experience post or antenatal depression through their specialised component ‘Beyond Babyblues’. 21 Although support groups may exist for women diagnosed with bipolar disorder during their pregnancy, there are no dedicated organisations for this condition. If, however, such attentive parenting is overly-vigilant, and low in affection – the so called ‘affectionless-control’ parenting style – the parent may falsely attribute normative developmental changes in their child as signs of an incipient mood disorder, with any such false alerts likely to be counter-productive. 22
This study highlights the strong views women have about their mood disorder, children, medication and pregnancy – especially for those women with a bipolar disorder. The perceived risk of their children inheriting a mood disorder and the expressed desire to engage in vigilant, attentive parenting behaviours are notable findings. Future research could focus on the association between the desire to be a vigilant parent, and the actual parenting behaviours enacted by parents with a mood disorder, with the focus extended beyond women to better understand the views of their partners. It would be particularly important to examine the response patterns of parents fully informed about differential risks and those who have not been so provided, as findings from this study suggest that quite different patterns could be elicited.
Footnotes
Acknowledgements
The researchers would like to thank Belinda Horton, CEO of the Post and Antenatal Depression Association (PANDA) for her expertise and assistance.
Funding
This study was funded by National Health and Medical Research Council Program Grant 510135 and an Infrastructure Grant from the NSW Department of Health.
Disclosure
The authors report no conflict of interest. The authors alone are responsible for the content and writing of the paper.