
Abstract
Objectives:
Community treatment orders (CTOs) allow clinicians to provide unconsented outpatient treatment to people living with mental illness. Though controversial and of uncertain efficacy, CTOs are used throughout Australia and internationally. We sought to determine the prevalence of CTO use in Australian states and territories, and to examine changes in the pattern of use over time.
Method:
Australian state and territory mental health review tribunals and health departments were surveyed for the most recent annual data on the total number of CTOs made and the total number of individual people placed on a CTO.
Results:
Rates of CTO use range from 30.2 per 100,000 population (in Tasmania) to 98.8 per 100,000 population (in Victoria). Use of CTOs in Australia is high by world standards, appears to be increasing over time, and varies significantly across jurisdictions.
Conclusions:
The high (by world standards), increasing and variable use of CTOs in Australia is concerning and raises important implications for mental health policymakers and legislators. Current mental health policy activity, particularly the new National Mental Health Commission, provides a unique opportunity to enhance transparency and accountability if regular and nationally uniform CTO data are collected and publically reported.
Keywords
Most of the care of serious psychiatric illness is delivered in the community, rather than the inpatient setting. 1 In 2008, community based care accounted for 53% of total mental health spending in Australia. 1 To facilitate such community care, all Australian state and territory mental health acts provide for the use of community treatment orders (CTOs) to enable unconsented outpatient psychiatric treatment. A CTO may be instituted on grounds similar to those that justify involuntary inpatient treatment. Once in place, patients who are subject to a CTO must submit to psychiatric treatment regardless of whether or not they have consented to the treatment and regardless of their capacity to refuse such treatment.
Despite having been in use for more than two decades, the value of CTOs in terms of their efficacy2 –6 and acceptability7 –9 remains subject to debate. With a few very rare exceptions, no other Australians may be forced to take medical treatment despite a competent refusal. Indeed, people who retain the capacity to refuse medical treatment may do so even if their decision may be regarded as irrational and might cause them serious harm or even bring about their death. 10 There might be some justification for this special exception applying to people who live with mental illness if CTOs were more effective than standard voluntarily negotiated care. However, the evidence base for the efficacy of CTOs is small and contradictory.2 –5
Nonetheless, the use of CTOs is common. From 2008–09, more than one million of the 6.37 million service contacts with community mental health services in Australia were classified as involuntary. 11 Those most likely to be subject to CTOs are those with severe and persistent mental illnesses, such as schizophrenia, bipolar disorder and major depression. 2
Rates of CTO use vary significantly around the world. A 2005 review of CTO use internationally by Lawton-Smith found rates of use ranged between two per 100,000 population (Ontario and Saskatchewan in Canada, and New York State in the United States) to 40–60 per 100,000 population (in the Australian states of Queensland and Victoria, and the District of Columbia in the United States, and New Zealand). 12 The general pattern was of fewer people being placed under community-based involuntary psychiatric treatment in Canada, high numbers in Australasia, and ‘a very mixed picture in the United States’. Lawton-Smith also observed: ‘Whatever the jurisdiction, the number of people placed on community-based orders almost universally increased year on year’. 12 The review also noted that there is little published international data on the number of people placed on CTOs, and what data is available is limited by differences in CTO frameworks and data collection systems and by incomplete public records.
The Commonwealth Government recently committed to both improving community-based mental health services for people suffering with severe and persistent illness, and creating greater accountability and transparency in the mental health system.13–14 In light of these reforms, it is crucial that there is a clear picture of rates of use of CTOs in Australia. We report the results of an Australian audit of CTO rates.
Methods
Australian state and territory mental health review tribunals and health departments were contacted by email from January to March 2012 and asked to provide the most recent annual data (for 2010–11) on the total number of individual people placed on a CTO, and/or the total number of CTOs made.
Tribunals and departments were contacted by email and/or telephone from February to March 2012 to follow up initial inquiries where necessary. Where no response was received, the annual reports of tribunals and health departments were accessed online and hand-searched for published CTO data.
The figures collected were then compared to previously published data on the number of people subject to community-based orders per 100,000, including four Australian states. 12 Lawton-Smith’s 2005 study drew on responses from international jurisdictions to a questionnaire asking for data on the number of people subject to CTOs, and on interviews and a review of published literature. Of the four Australian states included in that study, CTO rates of use ranged from 17.6 per 100,000 in Western Australia, 15 to 37.4 in NSW, 16 42.9 in Queensland, 17 and 55 in Victoria. 18
Results
Figures on CTO rates were compiled for all states and territories from a combination of database or annual report extracts provided by tribunals or departments, or information found in published annual reports.
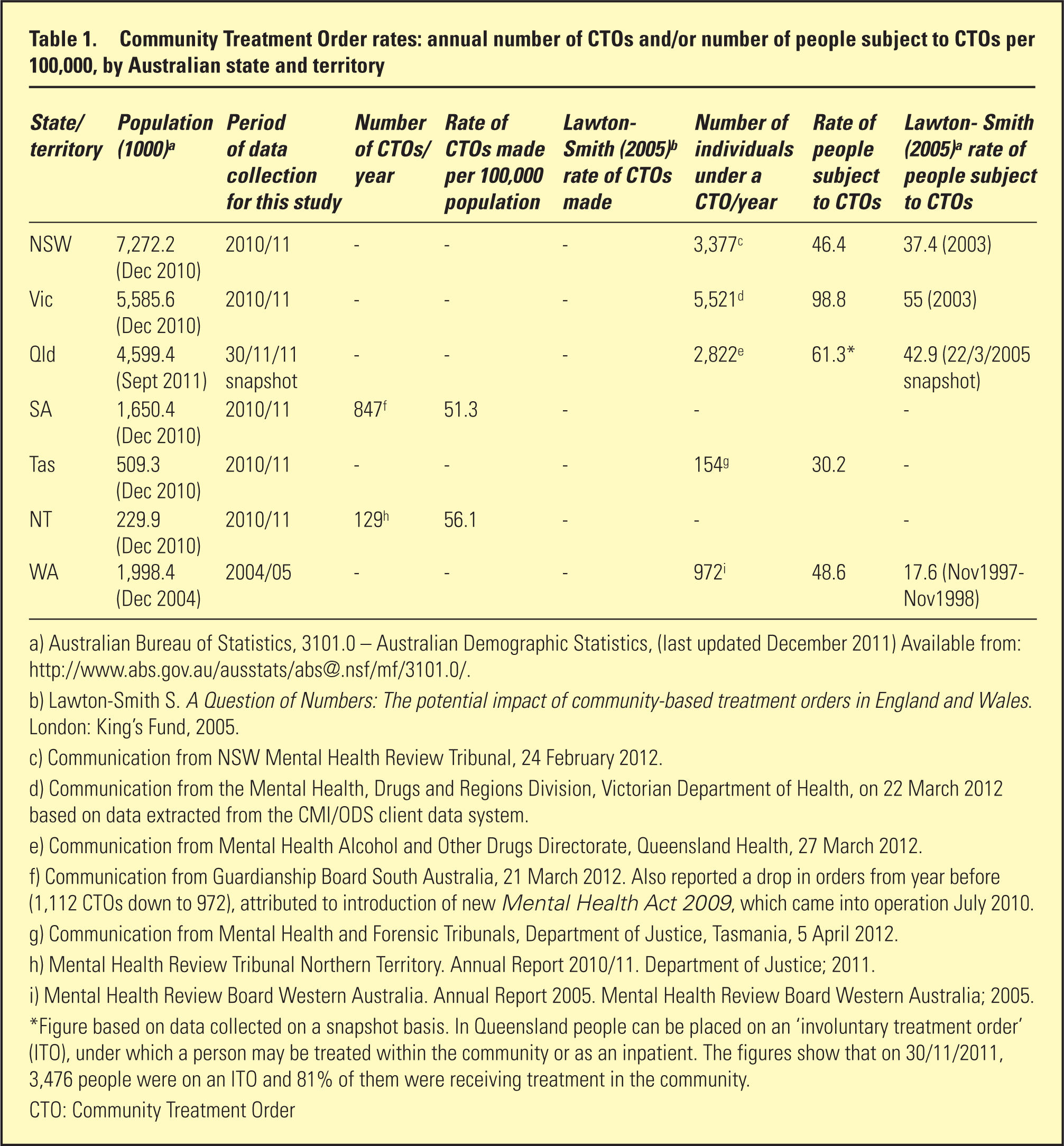
Table 1 details the data collected on the number of CTOs made in a year and the number of individuals under a CTO in a year. It also compares current rates of CTO use per 100,000 with the figures published in Lawton-Smith’s 2005 analysis of CTO use in four Australian jurisdictions. Not all jurisdictions were able to provide an annual count of CTOs or individual persons on CTOs. It was not possible to include data from the Australian Capital Territory (ACT) in the analysis. ACT Health reported there were 884 psychiatric treatment orders from 2010 to 2011; however, it was not possible to determine from the data available the proportion of orders that were community or inpatient based. In the ACT, as in Queensland, legal frameworks enable a single involuntary treatment order to allow community-based or inpatient treatment, or both. ACT Health advised that, at any given time, the majority of people on orders would be treated in the community setting.
Community Treatment Order rates: annual number of CTOs and/or number of people subject to CTOs per 100,000, by Australian state and territory
Australian Bureau of Statistics, 3101.0 – Australian Demographic Statistics, (last updated December 2011) Available from: http://www.abs.gov.au/ausstats/abs@.nsf/mf/3101.0/.
Lawton-Smith S. A Question of Numbers: The potential impact of community-based treatment orders in England and Wales. London: King’s Fund, 2005.
Communication from NSW Mental Health Review Tribunal, 24 February 2012.
Communication from the Mental Health, Drugs and Regions Division, Victorian Department of Health, on 22 March 2012 based on data extracted from the CMI/ODS client data system.
Communication from Mental Health Alcohol and Other Drugs Directorate, Queensland Health, 27 March 2012.
Communication from Guardianship Board South Australia, 21 March 2012. Also reported a drop in orders from year before (1,112 CTOs down to 972), attributed to introduction of new Mental Health Act 2009, which came into operation July 2010.
Communication from Mental Health and Forensic Tribunals, Department of Justice, Tasmania, 5 April 2012.
Mental Health Review Tribunal Northern Territory. Annual Report 2010/11. Department of Justice; 2011.
Mental Health Review Board Western Australia. Annual Report 2005. Mental Health Review Board Western Australia; 2005.
Figure based on data collected on a snapshot basis. In Queensland people can be placed on an ‘involuntary treatment order’ (ITO), under which a person may be treated within the community or as an inpatient. The figures show that on 30/11/2011, 3,476 people were on an ITO and 81% of them were receiving treatment in the community.
CTO: Community Treatment Order
The data show rates of CTO use vary enormously between Australian jurisdictions, ranging between 30.2 per 100,000 in Tasmania and 98.8 per 100,000 in Victoria. The data also show that rates of CTO use in Australia continue to be relatively high compared to international rates of use and suggests that rates have increased in states where there are previously available figures.
Discussion
This study provides the most comprehensive national picture of the rates of CTO use in Australian states and territories. It updates previously published rates for four states, finding that rates of use, already considered relatively high, have likely been increasing, and that rates between jurisdictions vary widely.
All Australian states and territories except Tasmania have rates of CTO utilisation that are now within, or exceed, the highest jurisdictional rates of 40–60 per 100,000 identified by Lawton-Smith’s 2005 international analysis. Recent data for some of the jurisdictions reported in Lawton-Smith’s 2005 study reveal persistent variation across jurisdictions and increasing rates of CTO utilisation over the past decade. For example, New Zealand’s comparatively high rate in 2003 of 44.2 per 100,000 in Lawton-Smith’s review 12 rose to 77 per 100,000 in 2010. 19 From 2000–2001, New York State had a lower rate of 2.1 per 100,000. 12 Published figures show 2,976 CTOs were made in New York State during the past 12 months 20 within a population of almost 19.5 million, 21 equal to a rate of 15.2 per 100,000.
As was the case with Lawton-Smith’s review, 12 our analysis was limited by jurisdictional differences in: data collection systems and availability; data collection timescales; and the categorisation of CTOs in legal frameworks. Comparisons across jurisdictions therefore need to be treated with caution. Despite these limitations, this audit provides the most complete and consistent picture of Australian CTO use published to date, enabling comparisons between jurisdictions and across different periods.
The exact reasons why CTOs are so prevalent in Australia and why their use is increasing, both in Australia and internationally, are unclear. As Dawson has noted, the factors influencing CTO use are dynamic and fluid so ‘widely varying rates of use of CTOs can develop in different jurisdictions with otherwise similar legal traditions, and rapid changes can occur in the rate of use of CTOs, over time, even within a single jurisdiction, without any change occurring in the law.’ 22
Changing rates of CTO use may therefore be attributed to a range of different influences, including: the attitude of clinicians; the powers provided to treat involuntary outpatients; the threat of clinicians being liable for the conduct of patients in the community; the perceived impact of coercion on therapeutic relationships; perceptions that persons with mental disorders in the community pose a public risk; a greater number of people receiving a less restrictive method of treatment than involuntary hospitalisation; and the adequacy of system resourcing and structures to respond to recurrent or chronically disabling disorders.9, 12, 22 –24
The potential explanation for the wide variation of rates of use of CTOs in different Australian jurisdictions may entail subtle differences in mental health acts across states and territories, differences in the resourcing of community compared to inpatient mental health services across jurisdictions, or the differential effects of the intercession of third parties such as state coroners or statutory bodies. In NSW, for example, Dawson’s 16 review found that CTOs appear to be used as something of a ‘safety valve’ for mental health and criminal justice systems under considerable pressure, much of which has arisen from the rapid deinstitutionalisation of services during the 1980s and 1990s that occurred without sufficiently rapid developments in the infrastructure of community mental health care. The need for further work to determine the factors driving increasing use is identified in a Victorian mental health reform strategy, which also notes that although CTOs are ‘an important element of community-based treatment, their increasing use is a cause of some concern’. 25
The higher, increasing and variable use of CTOs identified in this study is relevant to ongoing deliberations in Australia about policy and system responses to people living with mental illnesses and the use of involuntary treatment in the community setting. As has been argued elsewhere, 5 the current invisibility of CTOs in mental health policy potentially marginalises the people subject to such orders and limits the transparency and accountability of the system and our understanding of whether the differences in rates of CTO use relate to local laws, practices, or system funding and organisation. The involuntary care and treatment of people with mental illness is ‘too important a matter not to be informed by reliable data’ about the experiences of people subject to it and the processes and orders they undergo.26, p. 306–307
It is only where data is available on CTOs that steps can be made to critically examine the involuntary care of people with mental illness in the community. The report prepared by the Care Quality Commission (CQC) on the use of the Mental Health Act in England provides an illustration of the ability of data to examine how a mental health care system is working and to keep it accountable. The commission has a statutory duty to monitor how mental health services exercise powers until the Act, to provide a safeguard for patients. In preparing the 2010–11 annual report, commissioners made 1,565 visits to services and met more than 4,700 patients. 27 The CQC found that the use of CTOs, which were introduced in November 2008, rose by 29% in a year,27,28 with 4,291 people subject to a CTO during the reporting year 27 (with a population of 52.5 million, 29 this is equal to a national rate of CTO use of 8.1 per 100,000). Publication of the Commission’s figures enabled public examination of how CTOs are being applied and why the rates may be increasing.27,28 It found that even though there had been a 29% increase in the number of people subject to a CTO, there were fewer new CTOs started during the year. ‘This suggests that CTO powers, once implemented, may last for quite some time, and that the population subject to CTO will continue to grow.’27, p. 2 It also reported that it continued to find evidence that some providers misunderstood the legal powers of CTOs.
The current activity in mental health policy in Australia – particularly the establishment of the first National Mental Health Commission and its plans for an annual mental health report card – provide a unique opportunity to increase transparency and accountability with the inclusion of regular and nationally uniform CTO data. In a review of mental health commissions, Rosenberg and Rosen conclude that ‘nascent and established commissions are delivering real reforms, including in terms of additional resources and influence.’ 30, p. 193. The potential for an independent body, such as a commission, to make a ‘crucial accountability and public policy contribution’ by routinely compiling, analysing and reporting data about involuntary treatment has been recognised in Carney et al.’s research into Australian mental health tribunals. 26
In a public survey on what information should be included in its first and future annual report card (run between 28 April and 8 May 2012), the National Mental Health Commission sought people’s feedback on what kind of information would encourage improvement of services and would make services more answerable for the support and treatment they provide. 31 CTOs are one of the most contentious issues in mental health – their efficacy and ethical justification is unresolved and they raise serious human rights concerns. 5 The available research cannot distinguish between whether it is the coercive component of CTOs, or the increase in intensity of clinic care they facilitate, that may explain any of their putative benefits. Our study found that Australia has high rates of CTO use, which have increased over time, and which vary markedly from jurisdiction to jurisdiction. The Commission cites a vision that its Report Card will be focussed on people’s lived experiences, be rigorous and useful, and a ‘truthful mirror’. If the Commission mandates the regular provision of quantitative and qualitative assessment of the use of CTOs through uniform reporting processes, this would be an important step towards proper oversight of the use of CTOs and contribute towards addressing the scientific and human rights concerns about their utilisation by mental health services.
Footnotes
Disclosure
The authors report no conflict of interest. The authors alone are responsible for the content and writing of the paper.