
Abstract
Objective:
We aimed to identify the baseline prevalence of cardiac dysfunction in patients commencing clozapine, assess adherence with echocardiographic monitoring recommendations, and evaluate the utility and cost of echocardiographic monitoring for the development of clozapine-associated myocarditis and cardiomyopathy.
Methods:
A retrospective longitudinal cohort study was undertaken of 159 consecutive patients from a major tertiary centre commencing clozapine in the period January 2002 to July 2009.
Results:
Some 73% of patients had a baseline study, and 11% had a six-month follow-up study. Nine patients had abnormal left ventricular function at baseline. Myocarditis was identified in three patients, with all cases occurring within the first month of treatment and suspected on clinical grounds before an echocardiogram was performed. One case of possible cardiomyopathy was identified. The cost of echocardiographic screening in the first year of treatment was estimated at $AUD 209,356 per case of cardiomyopathy detected.
Conclusion:
The prevalence of cardiac dysfunction in patients commencing clozapine is high, and there are challenges in adhering with the recommended protocol for monitoring. Routine echocardiography is not useful in the detection of clozapine-associated myocarditis. Although cardiomyopathy may be identified, it is rare and associated with significant cost. Recommendations for routine echocardiographic monitoring should be re-examined.
The atypical antipsychotic medication clozapine is useful in the treatment of refractory schizophrenia. A tricyclic dibenzodiazepine derivative, its effectiveness has been quoted at up to 30% in this challenging patient population. 1
Although an effective antipsychotic agent, the use of clozapine has been restrained by a range of serious adverse effects. Long known to cause agranulocytosis at an incidence of approximately 1% in the first year of treatment, 2 recent focus has shifted to the potential for cardiac toxicity. Minor cardiovascular side effects such as tachycardia are very common, 3 but of greater concern is the risk of myocarditis and cardiomyopathy, as shown in multiple retrospective studies.
Reported incidences of clozapine-associated myocarditis have ranged from 0.015–1.2% of patients treated.4–9 One difficulty with estimating the incidence of this condition stems from variation in case definition. The true incidence may have been under-reported in early studies, given a lack of awareness of these potential side effects. Furthermore, there may not be a classic presentation of clozapine myocarditis, with a range of possible symptoms and abnormal laboratory investigations. Endomyocardial biopsy could be considered a gold standard for diagnosis, but this is rarely performed, and may miss cases if there is patchy involvement of the myocardium. The role of biomarker testing 10 and newer imaging techniques such as cardiac magnetic resonance imaging 11 remains unclear. A proposal to standardise the case definition and develop a rational monitoring protocol has been published recently. 12
A causative mechanism for the development of clozapine myocarditis has not been established, but there are multiple theories which are summarised in a recent review. 13 The leading hypothesis is that it constitutes an IgE-mediated hypersensitivity reaction with selective cardiac involvement. 5
The entity of clozapine-associated cardiomyopathy is poorly defined. The incidence has previously been reported as one case per 1000 patients treated. 5 It is noteworthy that the prevalence of some cardiovascular risk factors is increased in patients with schizophrenia compared with the general population, which could theoretically lead to an increased risk of cardiomyopathy independent of clozapine use. 14 There is uncertainty as to whether clozapine is more likely than other antipsychotics to result in cardiomyopathy, with one report of autopsy findings showing no difference in cardiac findings between clozapine and risperidone. 15 If clozapine-associated cardiomyopathy does exist as a distinct entity, the mechanism is unclear. Although a direct toxic effect to the myocardium is possible, it may be difficult to establish a specific mechanism beyond a secondary effect from weight gain, tachycardia and the presence of coronary artery disease.
Current recommendations for monitoring of potential cardiac toxicity have been derived empirically and may be neither rational nor cost effective. Monitoring guidelines circulated by Novartis and Hospira suggest an echocardiogram be performed at 6 months after initiation of clozapine. Similar to many centres in Australia, and consistent with the consensus view from major psychiatric facilities of Victoria, Australia, 16 our institution’s policy involves a baseline echocardiogram before clozapine is started, along with yearly echocardiograms following the initial 6-month study. This approach has proven to be costly, time consuming and logistically difficult.
We sought to investigate the baseline prevalence of cardiac dysfunction in patients commenced on clozapine, assess whether current echocardiographic monitoring recommendations are being consistently applied, evaluate the frequency of abnormal findings during monitoring and determine the cost of routine echocardiographic monitoring for the development of clozapine-associated myocarditis or cardiomyopathy.
Methods
We performed a retrospective longitudinal cohort study of 159 consecutive patients commenced on clozapine between 1 January 2002 and 30 June 2009 through St Vincent’s Mental Health Service. Some 37 patients were excluded from analysis on the basis that their medical record was not available for review. Twenty of these patient files were held by correctional health services. A further 17 records were either in current clinical use or could not be collected by Health Information Services during the audit period. A full review of the medical record of the remaining 122 patients was undertaken.
We collected data relating to age, gender, time of clozapine commencement and time of ceasing clozapine. Where clozapine was ceased, the reason for ceasing was assessed and recorded. If the cause of clozapine cessation was identified as either myocarditis or cardiomyopathy, an assessment of the available data was made by the auditing team as to how likely this diagnosis was to be correct. Where necessary, cause of death was also recorded.
A thorough search for all of the available echocardiogram reports for each patient was undertaken. To identify applicable echocardiogram reports, the database of echocardiograms performed by the Cardiac Investigation Unit at St Vincent’s Hospital Melbourne was searched by medical record number. These reports were cross-referenced with echocardiogram reports filed in the patient’s medical record. In the few instances where echocardiograms had been performed by an external service, reports were audited where available in the medical record.
For each echocardiogram report, note was made of the date that the echocardiogram was performed and the left ventricular ejection fraction (LVEF). The date of the echocardiogram was cross-referenced with the date of clozapine commencement. A patient was considered to have had a baseline echocardiogram if an echocardiogram had been performed within the 3 months preceding clozapine initiation. In relation to follow-up studies, a patient was considered to have had a 6-month study if an echocardiogram had been performed between 150 and 210 days after the clozapine commencement date. The data obtained from the echocardiogram reports were analysed further with a focus on the identification of possible cases of clozapine-associated cardiomyopathy. A patient was considered to have possible clozapine-associated cardiomyopathy if they satisfied the criteria of a LVEF of less than 50% on any echocardiogram in the follow-up period, and with at least a 5% decrease from their baseline value.
A simple cost analysis was undertaken with respect to the identification of cardiomyopathy, using the current Medicare schedule of $AUD 230.65 for the performance and reporting of a transthoracic echocardiogram. 17
Results
The patient group was predominantly male (71.3%) with a mean age of 35.9 years (range 16–65). The baseline demographics of the audited group were not significantly different to the non-audited group with respect to age or gender.
Length of time on clozapine was calculated as the time between a patient commencing clozapine and either ceasing clozapine or the end of the audit period. The mean length of time on clozapine was 1360 days (3.72 years). Overall, the audit period encompassed 453.84 patient years.
A baseline echocardiogram had been performed in 89 of the 122 patients (73%) within 3 months prior to the commencement of clozapine. Only 79 patients (65%) underwent at least one echocardiogram in the follow-up period. Only 14 patients (11%) underwent an echocardiogram at the recommended 6-month time-point following commencement of clozapine.
Of the 89 patients with a baseline echocardiogram, the mean ejection fraction was 59%. Nine patients (10%) had abnormal left ventricular function at baseline, defined as a LVEF less than 50%.
In total, 33 of the 122 patients (27%) ceased clozapine during the audit period. Reasons for ceasing are outlined in Table 1. Probable myocarditis was identified as the reason for cessation in three patients. One patient who had a pre-existing cardiomyopathy with a LVEF of 45% on their baseline echocardiogram was identified to have a worsening ejection fraction (35%) on an echocardiogram performed 4 months after starting treatment. One patient died during the audit period. Although the cause of death was unknown, it occurred in a patient in residential care after a prolonged period of cognitive and physical decline, and was not thought to be related to clozapine therapy.
Reasons for ceasing clozapine
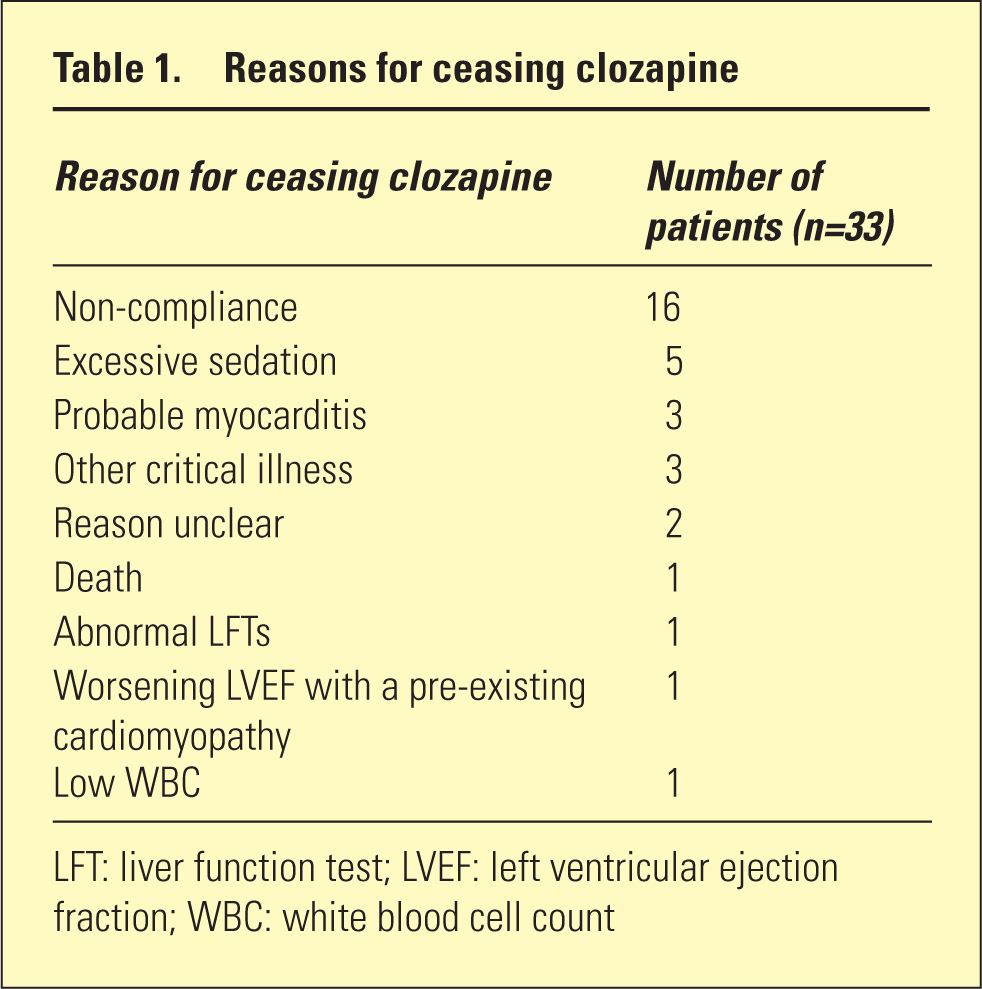
LFT: liver function test; LVEF: left ventricular ejection fraction; WBC: white blood cell count
Myocarditis was identified in three patients at days 13, 17 and 23, respectively, after the commencement of clozapine. In all of the patients with probable myocarditis, this was identified on the basis of symptoms and blood tests, including a full blood count and C-reactive protein (CRP) level. Clozapine had been ceased by the time of echocardiography in all of these patients. A LVEF of less than 50% was documented in two out of the three.
In relation to possible clozapine-associated cardiomyopathy, review of the medical records did not identify any hospital admissions with heart failure during the audit period. Of the 79 patients who underwent a follow-up echocardiogram at any time, six patients were identified who satisfied the pre-defined criteria of LVEF less than 50% and a greater than 5% decline from their baseline study.
After further review of these six patients, only one was considered to have a possible clozapine-associated cardiomyopathy. This was a 24-year-old male with a baseline LVEF of 60%. A decision was made 20 months after starting to wean clozapine in favour of depot antipsychotic treatment because of compliance issues. Four months after weaning was commenced but while still taking clozapine, an echocardiogram showed a LVEF of 40%. Although asymptomatic, this patient was considered to have a possible clozapine-associated cardiomyopathy, and weaning was continued. LVEF was reported at 57% one year after cessation of clozapine.
Of the other five patients, one developed left ventricular dysfunction in the setting of coronary artery disease and aortic stenosis. As noted above, another patient had a pre-existing cardiomyopathy with a LVEF that worsened 4 months after starting treatment. Three of the patients were found to have normal left ventricular ejection on subsequent echocardiograms or nuclear gated heart pool scans, and remained asymptomatic.
Overall, our data of one patient developing a possible clozapine-associated cardiomyopathy over 453.84 patient years suggest an incidence of 0.22% in the first year of treatment.
The current Medicare Benefits Schedule scheduled fee for the performance and reporting of a single transthoracic echocardiogram is $AUD 230.65. The cost of routine screening in the first year of treatment (baseline echocardiogram and 6-month study) would therefore be $AUD 461.30. Based on an incidence of 0.22 per 100 person years, the cost of echocardiographic screening in the first year of treatment equates to $AUD 209,356 per case of clozapine-associated cardiomyopathy detected.
Discussion
To our knowledge, this is the first study to examine both the prevalence of baseline cardiac dysfunction in patients being commenced on clozapine, and the utility of routine echocardiographic monitoring for potential cardiac toxicity during clozapine therapy.
Although surprising to discover such a high baseline prevalence of cardiac dysfunction, this finding could be consistent with other reports of increased prevalence of cardiovascular risk factors in patients with schizophrenia compared with the general population. 14
Overall, there was poor adherence with the recommended protocol. The reasons for this were not evaluated, but may be related to logistic difficulties in scheduling echocardiograms in this patient group.
Given that all cases of myocarditis occurred in the first month of treatment, routine echocardiography at 6 months was not helpful. This finding adds weight to recent proposals that the focus should be on active clinical monitoring augmented with laboratory investigations such as CRP and troponin in the first month of treatment. 12 Echocardiography should be used as part of confirmatory testing if a case is suspected.
In relation to clozapine-associated cardiomyopathy, it is clear that further work is needed to establish whether this is a condition independent of other risk factors for cardiomyopathy and whether the true incidence is higher in patients treated with clozapine versus other antipsychotic medications. The cost of identifying one potential case of clozapine-associated cardiomyopathy is high, and given our small sample size, it is possible that the incidence of clozapine-associated cardiomyopathy was overestimated. If the data of Kilian et al. are used, which suggest an annual incidence of 0.05%, 5 the cost of identifying one case would be much higher at $AUD 922,600. One could argue that these resources might be better targeted at the small group of patients with pre-existing cardiomyopathy, or at patients who develop symptoms suggestive of cardiomyopathy during the course of clozapine treatment. We would advocate that while a baseline echocardiogram should remain mandatory, further echocardiograms should only be performed at the discretion of the treating team.
Our study has several limitations, including a relatively small sample and difficulty in accessing medical records for some patients, so that only 76% of the cohort we originally identified were evaluated in detail. While the group evaluated in detail did not differ significantly to the group excluded with respect to age and gender, we cannot exclude the presence of other confounding factors. The retrospective nature of the study also hampers interpretation of data. Echocardiograms were reported by a number of different reporters, and a LVEF was obtained by a variety of methods including visual estimation in many cases. As the majority of patients did not follow a regular pattern of follow-up echocardiograms, an analysis of the stability of these measurements was not possible.
Despite these limitations, our results indicate the limited overall utility and high cost of the current recommendations for routine screening with echocardiography. We support the development of rational guidelines for monitoring of clozapine-associated myocarditis, focusing on the first month after clozapine commencement. Clearly, given the variety of presentations and sometimes abrupt onset of this condition, monitoring of any form presents difficulties. Intuitively, close clinical monitoring as well as frequent cardiac biomarker testing may provide the best solution for early detection of myocarditis and improving patient safety during this period.
Footnotes
Funding
This research was supported in part by an investigator-initiated grant from Hospira.
Disclosure
David Castle has received honoraria for talks and consultancy from Hospira.