
Abstract
Objective:
We report a rare case of bilateral maculopathy that developed with the initiation of sertraline.
Methods:
We conducted a case report and review of the literature.
Results:
A 23-year-old man rapidly developed maculopathy with associated visual blurring after the initiation of sertraline. Treatment was ceased with the patient subsequently reporting mild improvement in visual symptoms.
Conclusions:
Maculopathy associated with sertraline use has yet to be established and recognized as an adverse side effect. With only one previous reported case in the literature, this condition requires further awareness.
Sertraline, a selective serotonin reuptake inhibitor (SSRI), is a widely prescribed psychotropic drug. It is mainly prescribed for the treatment of depressive disorders (83%), anxiety disorders (11%) and occasionally for management of other disorders (6%) such as negative symptoms in bulimia nervosa and anorexia nervosa.1,2 Maculopathy refers to pathological change occurring at the central part of the retina responsible for high visual acuity, the consequence of which may range from reduced vision to possible blindness depending on severity. Changes such as pigmentary mottling and defects in the retinal pigment epithelium of the macular area may be seen on fundus autofluorescence imaging and optical coherence tomography. 3 While maculopathy is recognized in conditions such as diabetes, age-related macular degeneration, Stargardt’s disease and drug-related cases such as chloroquine toxicity, maculopathy occurring due to SSRIs is yet to be established. We present a rare case of a patient with acute onset bilateral maculopathy associated with sertraline use. To our knowledge, there has only been one previous published report of this clinical occurrence. 4
Case report
A 23-year-old man presented complaining of 2 weeks of worsening bilateral blurred vision and metamorphopsia. The onset of symptoms coincided with the initiation of 50 mg daily of sertraline, an SSRI. He had a medical history of asthma but no significant ocular history or family history.
On examination, uncorrected visual acuity was 6/6 in both eyes with normal pupillary responses. Colour vision testing scored 1/13 on the Ishihara pseudo-isochromatic testing (test plate only). Intraocular pressure was normal and anterior segment examination was unremarkable. Dilated fundal examination showed perifoveal retinal pigment epithelium atrophic changes with the appearance typical of Bull’s eye-type maculopathy. Fundus autofluorescence revealed patchy perifoveal areas of hyper- and hypo-autofluoresence (Figure 1(a)). Optical coherence tomography demonstrated intermittent outer segment defects and thickening of the retinal pigment epithelium (Figure 1(b)). These findings suggest retinal damage possibly from sertraline-induced toxicity. Sertraline was immediately ceased and the patient was reviewed 1 month later. At follow-up, the patient reported some mild visual improvement. In comparison, there was no improvement in vision even after several months in the case report by Sener and Kirath. 4 Visual acuity remained stable but fundus autofluorescence imaging demonstrated persistent retinal pigment epithelium changes. Central 10-degree perimetric visual field testing revealed perifoveal depression in sensitivity consistent with a Bull’s eye-type maculopathy (Figure 1(c)). The patient unfortunately did not return for further follow-up.
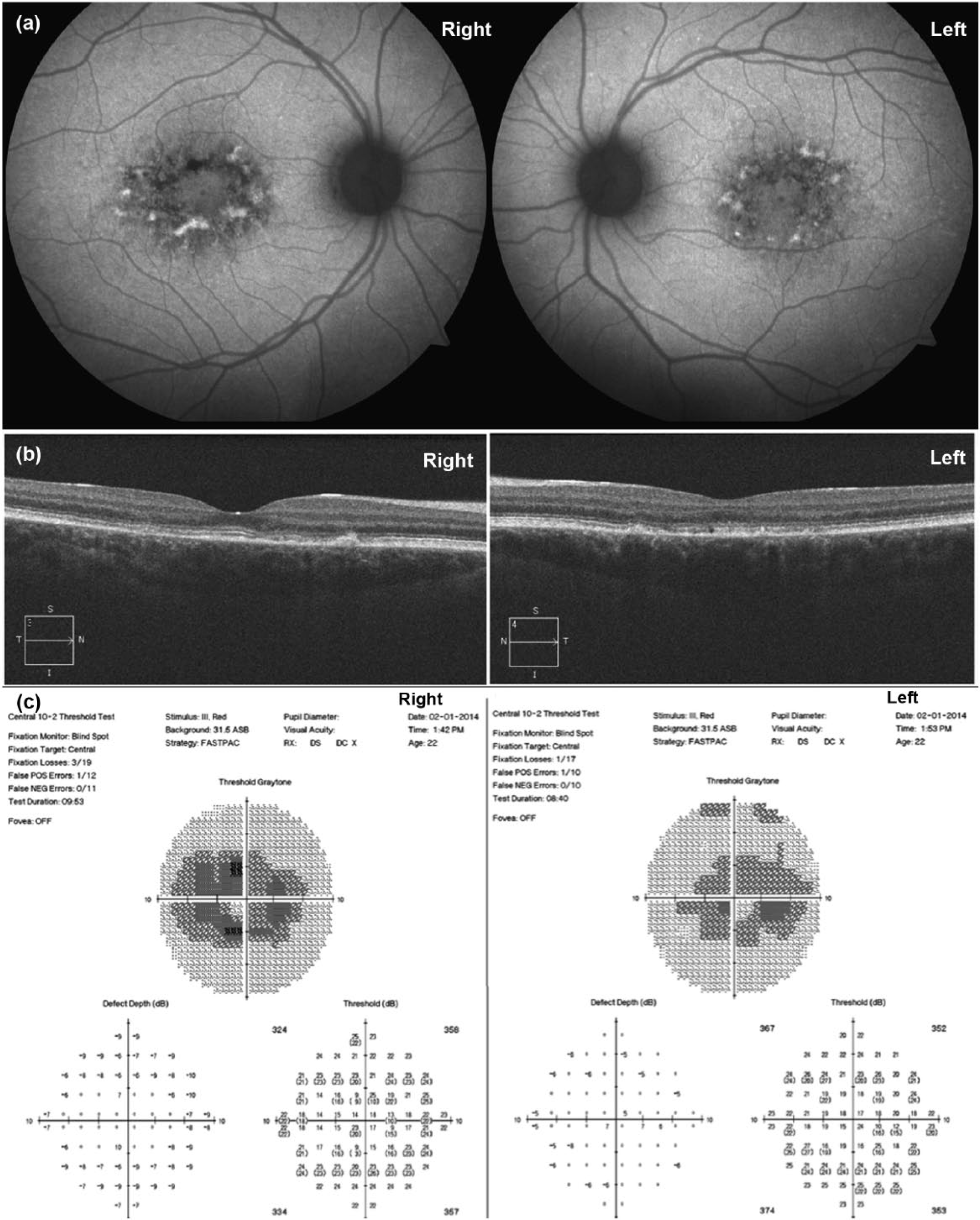
Fundus autofluorescence at initial presentation (a) shows patchy perifoveal areas of hyper- and hypo-autofluorescence. Optical coherence tomography (b) at initial presentation demonstrates retinal outer segment defects and thickening of the retinal pigment epithelium. Perimetric visual field testing at the 1 month follow-up (c) shows perifoveal depression in sensitivity.
Discussion
Antidepressants are among the most commonly prescribed medication in younger people. 5 Antidepressant use in Australia alone has doubled over the last decade, 6 with SSRIs being the most common group of antidepressant prescribed. 7 While the general and systemic side effects of SSRIs are well documented, the incidence of ocular side effects is unknown and reports remain anecdotal and infrequent. There are reports of mydriasis, raised intraocular pressure, oculogyric crises and glaucoma associated with SSRI use. 8 Although sertraline was introduced in 1991, more than two decades ago, there has only been one case of presumed sertraline maculopathy reported in 2001 by Sener and Kirath. 4 This case was of a 58-year-old female who developed deteriorating visual acuity, absent colour vision and central scotoma after 4 months of sertraline therapy (50 mg daily). Our case developed very rapidly (2 weeks) in an otherwise fit and healthy young adult. This presentation is consistent with the prior report, 4 and supports this rare but possible direct causal relationship between sertraline (or SSRI) use and development of bull’s eye-type maculopathy similar in appearance to that occurring in chloroquine toxicity and Stargardt’s disease. The limitations of our report lie in our ability to ascertain if the adverse changes due to sertraline were reversible, as the patient did not present for further follow-up.
A possible mechanism of SSRI-induced maculopathy is via its impact on phospholipase C. SSRIs may increase the functionality of 5-HT2AR by increasing the available level of synaptic serotonin. 9 Increased activation of the 5-HT2AR can lead to activation of phospholipase C, which can then result in all-trans-retinal (atRAL)-induced NADPH oxidase-mediated overproduction of intracellular reactive oxygen species. 9 This could then contribute to the pathogenesis of retinal degeneration via oxidative stress and pathological cell death within the retina.
Further evidence and investigation is required to expand our understanding of sertraline maculopathy. Given the increasing use of SSRIs in the community, more awareness and education is required to ensure that ocular side effects are detected early in order to prevent visual compromise.
Footnotes
Disclosures
The authors report no conflict of interest. The authors alone are responsible for the content and writing of the paper.