
Abstract
Objective:
This article provides a brief review of the practical implications of the current diagnostic conceptualisation of generalised anxiety disorder (GAD) and an update on its pharmacotherapy.
Conclusions:
The diagnostic criteria for GAD need to be refined, to better reflect its clinical features and to make GAD more clinically useful. Various pharmacological agents are effective for GAD and to some extent, allow a tailored treatment approach. In addition to effectiveness, the choice of medication is influenced by the speed of therapeutic action, tolerability and habit-forming properties.
Generalised anxiety disorder (GAD) has been considered a prototypical anxiety disorder that is in danger of being marginalised and neglected. 1 In recent years, we have witnessed much discussion about the diagnosis of GAD, along with some changes in its treatment. This article aims to briefly review the practical implications of the current diagnostic conceptualisation of GAD and to provide an update on the pharmacotherapy for this disorder.
Diagnostic conceptualisation of GAD: what does it mean for clinical practice?
The diagnostic criteria for GAD in the Fifth Edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) are the same as those in the Fourth Edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV); however, the pathway from the DSM-IV GAD to the DSM-5 GAD was not straightforward, 2 which reflects the complexity of GAD. Moreover, the same problems that plagued the DSM-IV GAD 3 continue to undermine the clinical utility of the GAD construct. These are listed in Box 1. The most important shortcoming is the lack of any diagnostic feature that is unique to GAD. It comes as no surprise that GAD continues to be neglected in clinical practice, despite its high prevalence rates in the community.
Conceptual problems with the DSM-IV/DSM-5 generalized anxiety disorder (GAD)
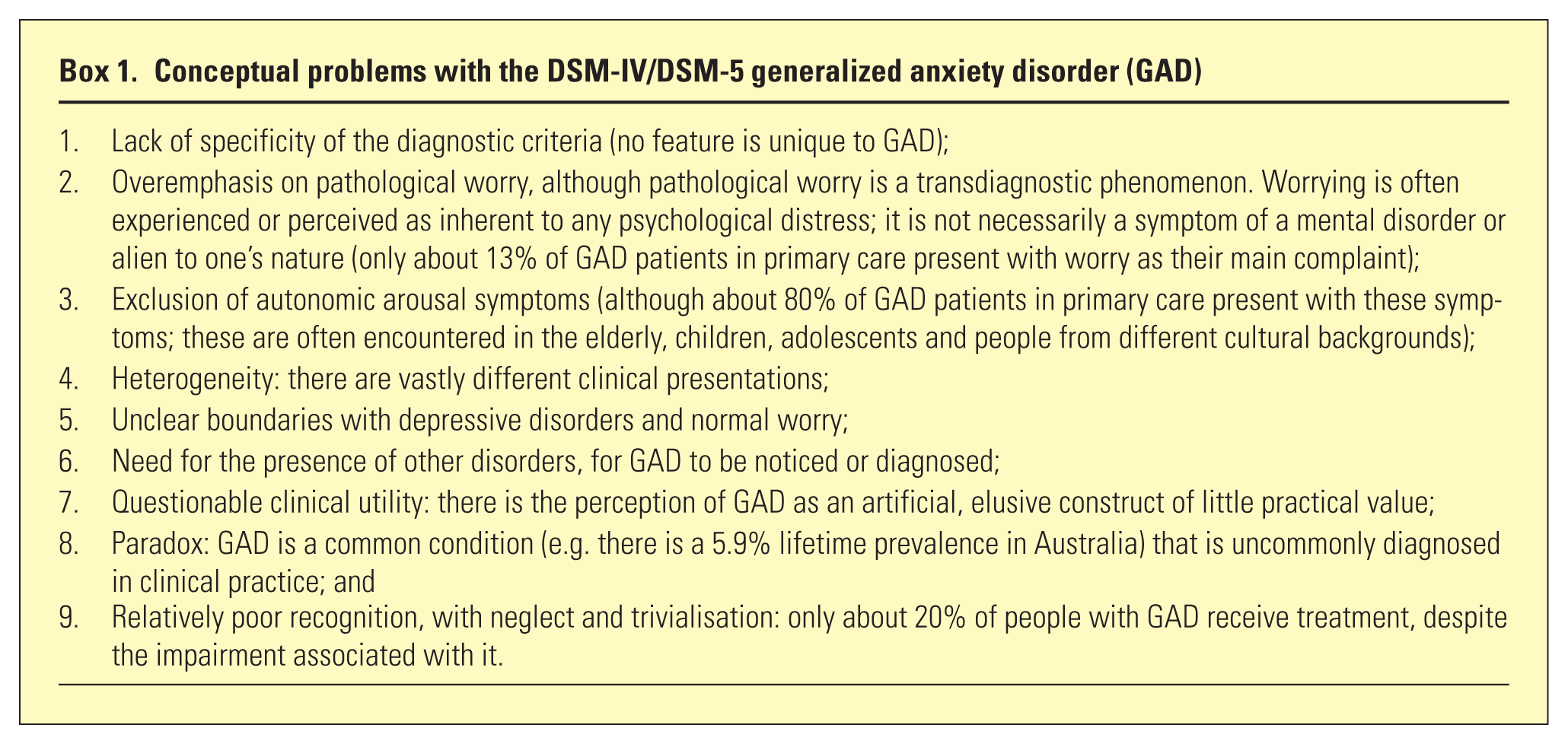
The practicing clinicians would benefit from a clearer delineation of pathological worry from normal worrying, when they ponder whether the former is a characteristic of GAD. Indeed, such worry should be understood as a cascade of uncontrollable and attention-grabbing ‘what if’ thinking scenarios or patterns; moreover, this worry is largely driven by a difficulty in coming to terms with uncertainty, so that worrying could perhaps cease only with complete certainty. Pathological worry is also characterised by ongoing doubt, which prevents formation of a closure; as a consequence, there is a constant anticipation of further complications and problems, with no solution in sight. The individuals with pathological worry do not live in the present. They experience it only as a prelude to a future that is perceived as filled with potential dangers. Thus, pathological worrying is incessant and fruitless overthinking that inhibits problem-solving and decision-making.
In addition to this reconceptualization of pathological worry, the diagnostic role of somatic manifestations of GAD, such as symptoms of autonomic arousal and muscle tension, should not be overlooked. These symptoms (e.g. gastrointestinal distress, trembling, sweating, lightheadedness, palpitations and dizziness) are already a part of the description of GAD in the Tenth Revision of the International Classification of Diseases (ICD-10) and will most likely be included in the upcoming Eleventh Revision of the International Classification of Diseases (ICD-11). While the researchers continue to grapple with the task of finding the right balance between the cognitive symptoms (e.g. pathological worry) and somatic symptoms as diagnostic criteria for GAD, clinicians will need to take both into account whilst assessing patients with chronic anxiety. This has important treatment implications.
Treatment considerations
Results of treatment studies in GAD suggest that there is much room for improvement. For example, the remission rate for GAD patients during the first year of pharmacological and/or psychological treatment was, in one study, only 13.3%. 4 An earlier study reports that 5 years after completion of pharmacological treatment, 18% of GAD patients were in remission, whereas > 50% continued to have symptoms, with significant functional impairment. 5
Efforts to improve treatment outcomes in GAD may entail combining pharmacological and psychological treatments, but there is very little evidence to support this common practice. Regardless of the treatment modality, several factors should be considered here. The first factor is the adoption and implementation of a long-term treatment strategy, because GAD is a chronic condition; this strategy pertains to efforts to maintain treatment gains over prolonged periods of time and to prevent relapses. The second factor is a need to target a broad range of features of GAD, including various cognitive and somatic symptoms. Finally, in view of a close relationship between GAD and depressive disorders, 6 the treatments for GAD also need to be able to reduce symptoms of depression, as these frequently occur concurrently with GAD or complicate its course. Novel treatments for GAD should be evaluated against these benchmarks, i.e. in terms of the extent to which they effectively address the above factors (Table 1).
Considerations in the choice of pharmacotherapy for GAD
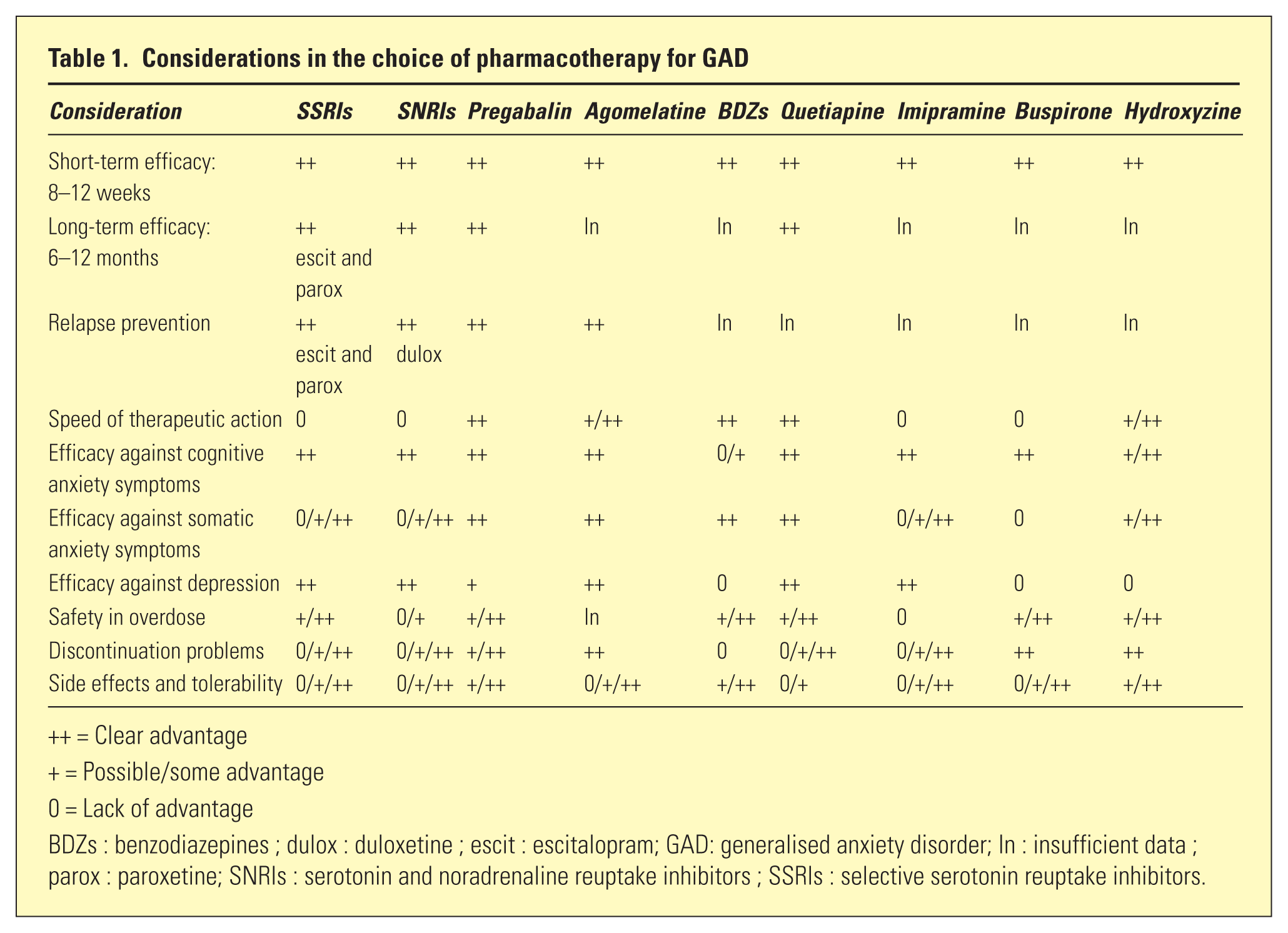
= Clear advantage
= Possible/some advantage
= Lack of advantage
BDZs : benzodiazepines ; dulox : duloxetine ; escit : escitalopram; GAD: generalised anxiety disorder; In : insufficient data ; parox : paroxetine; SNRIs : serotonin and noradrenaline reuptake inhibitors ; SSRIs : selective serotonin reuptake inhibitors.
Pharmacological treatment of GAD
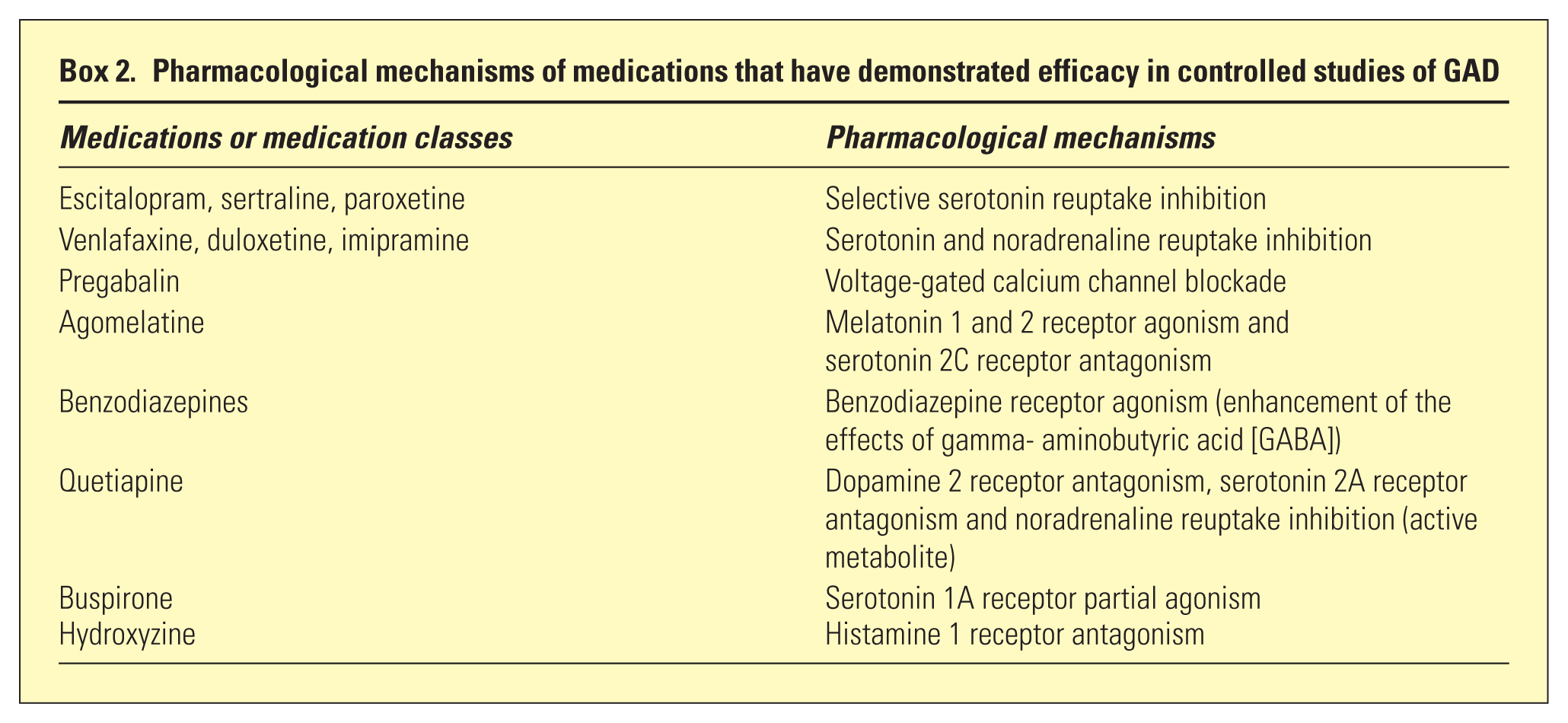
Compared to other anxiety disorders, there have been more pharmacotherapy trials conducted for GAD in recent times. As a result, a variety of medications with different pharmacological mechanisms have been found to be efficacious in double-blind, placebo-controlled trials (Box 2). These different pharmacological mechanisms also attest to the heterogeneity of GAD.
Pharmacological mechanisms of medications that have demonstrated efficacy in controlled studies of GAD
Choice of medication
How should clinicians navigate the often-troublesome waters of pharmacotherapy options for GAD? Several treatment guidelines have been published recently;7,8 despite their reliance on scientific evidence, they were influenced by the context in which they were developed and by the interpretations, if not biases, of their authors. For the Australian setting, all agents that are efficacious in short-term, controlled treatment studies of GAD can be classified into four groups (Box 3). This classification takes into account not only the drug’s efficacy and tolerability, but also the availability and cost of these medications. For example, pregabalin and agomelatine are expensive in Australia and not licensed for GAD; quetiapine is not subsidised for use in GAD, although it is licensed for it; and hydroxyzine is unavailable.
Classification of pharmacological agents for generalized anxiety disorder in Australia
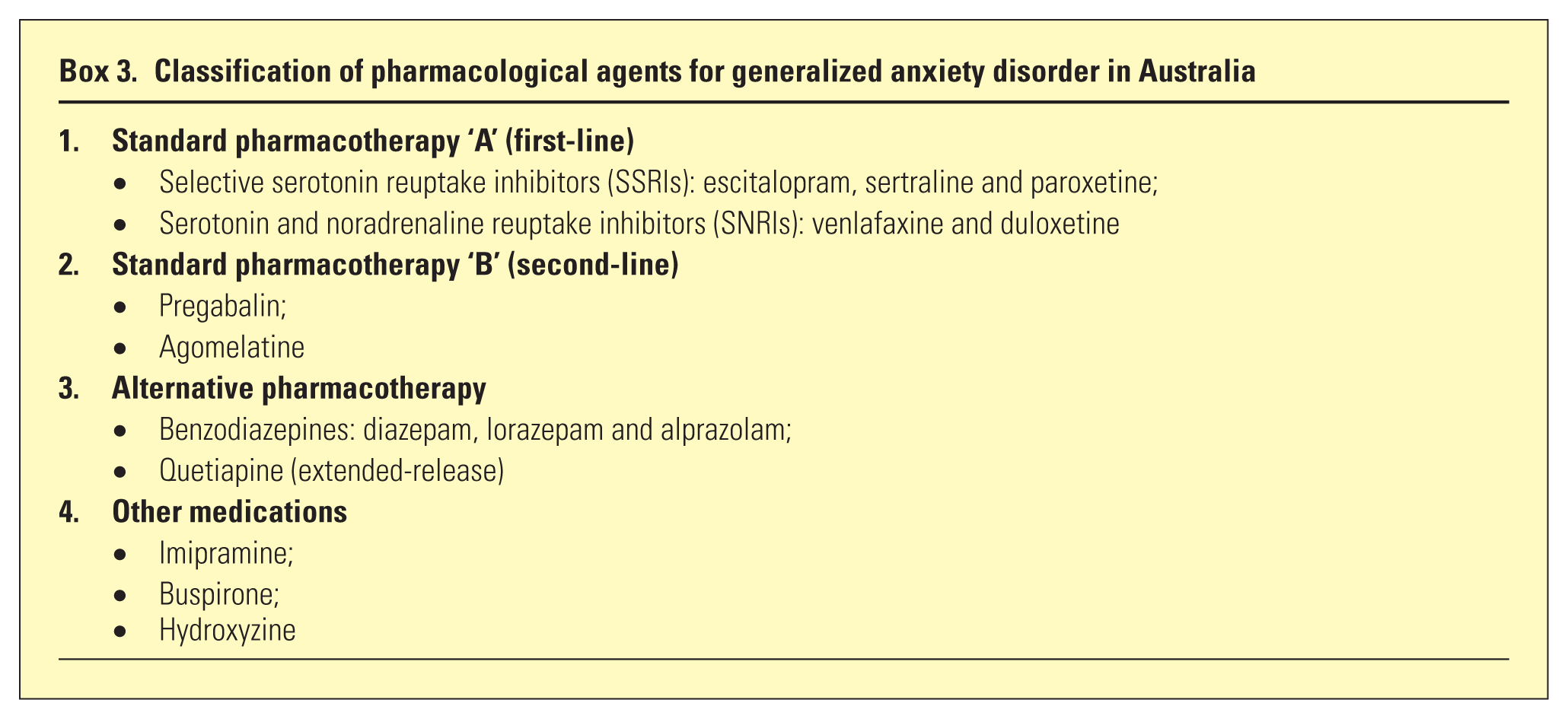
Table 1 lists the advantages and disadvantages of various medications for treatment of GAD. In most cases, the first choice in Australia is one of the selective serotonin reuptake inhibitors (SSRIs) or serotonin and noradrenaline reuptake inhibitors (SNRIs) that have demonstrated efficacy in GAD; however, there are four main problems with their use for GAD. First, they do not work quickly; it may be necessary to wait up to 12 weeks before their effectiveness can be assessed. There is some evidence, however, that patients who do not show an onset of effect within 4 weeks of treatment are unlikely to respond with continued treatment. 9 Second, the effectiveness of SSRIs and SNRIs against somatic anxiety symptoms varies, with many patients reporting little or no symptomatic relief. Third, the drugs’ side effects (e.g. increased anxiety and agitation, gastrointestinal disturbance, dizziness, headache, insomnia and sexual dysfunction) are often unpredictable and can be severe; not infrequently, tolerability problems are a reason for their premature cessation. Finally, the cessation of SSRIs and SNRIs is often associated with discontinuation problems, which can be distressing and in many ways, similar to those that occur with the cessation of benzodiazepines. 10 For these reasons, SSRIs and SNRIs are not always ideal for treating GAD; they can be combined with pregabalin, benzodiazepines or quetiapine, to facilitate a response. Alternatively, other medications may be used as monotherapy, instead of the SSRIs and SNRIs.
Pregabalin does not have most of the disadvantages of the SSRIs and SNRIs, and its efficacy in GAD has been convincingly demonstrated. Higher doses of pregabalin (e.g. 450–600 mg/day) may be more likely to be effective. 11
Pregabalin is not an antidepressant, but it may decrease the intensity of depressive symptoms in GAD patients. 12 While pregabalin is generally well tolerated, the dropout rates in some studies are relatively high, with common side effects including sedation, dizziness, headache and even weight gain. The advantages of agomelatine over the SSRIs and SNRIs are similar to those of pregabalin; however, there are no published data on its long-term efficacy in GAD. Studies suggest that agomelatine may be better tolerated than escitalopram, 13 but it has potential drawbacks: a need to monitor serum transaminases and side effects, such as hepatitis, nausea, dizziness, sedation and fatigue.
The efficacy of benzodiazepines as a long-term pharmacotherapeutic strategy in GAD has not been studied. These medications are relatively ineffective against cognitive anxiety symptoms and are ineffective against depression. Another drawback of benzodiazepines is the dependence associated with their long-term use. The ongoing popularity of benzodiazepines in the treatment of GAD and other anxiety disorders is due to their quick onset of action, the possibility of using them on an ‘as needed’ (prn) basis, their relatively good tolerability and reliable effectiveness against somatic symptoms of anxiety. 14 Although low-dose quetiapine (e.g. 150 mg/day) shows efficacy against GAD and has become an increasingly popular pharmacotherapeutic option, caution is needed, because of its side effects (e.g. sedation, weight gain and metabolic syndrome).
Compared to other medications, imipramine and buspirone have more disadvantages, which limit their use in GAD. They may be considered for patients who fail to respond to the more commonly used agents.
Conclusion
GAD is conceptually a ‘work in progress’. The diagnostic criteria for GAD need to be improved to better reflect its clinical features and turn it into a clinically useful construct. The heterogeneity of GAD calls for a more targeted treatment. A variety of medications are effective for GAD to some extent, and allow for a tailored pharmacotherapeutic approach. This approach also needs to consider the speed of therapeutic action, tolerability and habit-forming properties. Such an approach should improve treatment outcomes for this frequently neglected, but disabling condition.
Footnotes
Disclosure
The author reports no conflict of interest. The author alone is responsible for the content and writing of the paper.
This paper was presented at the International Anxiety Disorders Society Conference which was held in Melbourne in November 2014.