
Abstract
Objective:
To describe the clinical population of women admitted to a Mother–Baby Unit in Adelaide, South Australia and to evaluate changes during admission in both Axes I and II diagnoses of maternal mental health, and in mother–infant relationships.
Method:
Both clinical and self-report assessments of maternal mental health were made at admission and discharge, and self-report comparisons of the mother–infant relationship.
Results:
Depressive illnesses (46.2%) were found to be the most prevalent conditions leading to admission, with rates of psychosis (10.3%) and bipolar disorder (3.4%) being lower. A high incidence of borderline personality disorder (23.1%) was found clinically, with almost half the admitted women showing features of borderline personality disorder on a self-report measure at admission. Significant improvements in maternal mental health and the mother–infant relationship were found at the time of discharge.
Conclusions:
Admission to this Mother–Baby Unit on mothers’ self-report scales showed improvement in mothers’ mental health and the relationship that they have with their infant. Given the high prevalence of borderline personality disorder and emotional dysregulation identified within the population, treatment implications and possible consequences for the infant are discussed for this client group.
Keywords
Women are particularly vulnerable to the development or exacerbation of mental health disorders following the birth of a child. Joint admission of unwell mother and child to a mother–baby unit (MBU)1-3 has benefits including addressing mother–infant attachment or care issues that may be contributing to her disorder.1,3-6
Diagnostic groupings in MBUs show a high incidence of affective and psychotic illness. Of 1081 women admitted to eight MBUs in the United Kingdom, Salmon et al. 2 report that 38% had a diagnosis of a non-psychotic depression, 21% of schizophrenia, 14% of bipolar disorder, 4% of an anxiety disorder, 3% of a personality disorder and 1% of alcohol or substance abuse. A large scale study of French MBUs reported similar rates of mood disorders and schizophrenia, and 23% adult personality, behaviour, cognitive or mental organic disorders. 1 A New Zealand MBU study of 93 women showed high rates of affective disorder with less schizophrenia. 7 They also found that 59% of inpatients had more than one Axis I diagnosis, with 30% having an Axis II personality disorder.
A study of four MBUs 6 in Victoria, Australia, found 59% of women had major depression, 14% schizophrenia or a related illness, 8% puerperal psychosis, 5% bipolar disorder, 17% adjustment disorder, 7% anxiety disorder, 8% personality disorder, 2% substance abuse and 1% an eating disorder. A later Victorian MBU study 8 had similar results.
Fewer studies have evaluated the effectiveness of admissions to MBUs. Glangeaud-Freudenthal et al. 1 used the French version of the Marcé checklist (originally developed in the UK to measure clinical change in MBUs) and found that two-thirds of patients had improved significantly by the time of discharge. A large UK study using the Marcé checklist reported good clinical outcome for 78% of cases.
Despite clear evidence of the potential for poor outcomes for infants of mentally ill mothers,9-11 only two studies4,5 in an MBU have evaluated the infants themselves or the mother–infant relationship. Salmon et al. report good outcomes as assessed by staff in terms of baby care and emotional responsiveness in 80% of mothers and Bilszta et al. focus on improvements with either video or verbal discussion in direct mother–infant therapy. Others have focused only on whether infants have been removed from their mother’s care or whether child protection services have become involved in monitoring.
Helen Mayo House (HMH) is a six-bed publicly funded inpatient MBU located in Adelaide, South Australia, which admits women experiencing severe mental health issues with their infants up to the age of three years. Admitted women receive mental health treatment including individual, group and mother–infant psychotherapy, medication and ECT, and support from psychiatric, nursing and allied health staff.
The aims of this study are three-fold:
Describing the clinical characteristics of women admitted to the unit using both clinical and self-report data;
Evaluating improvements in mental health during admission to a MBU;
Evaluating improvements in outcomes for infants.
Design
Information about mental health diagnoses, mothers’ and infants’ ages and length of admission were collected for all consecutive admissions to the MBU unit during an 18-month period (N=117). All mothers who were able to provide informed consent were invited to complete measures assessing their mental health and the mother–infant attachment relationship at admission and discharge (ethics committee approval was obtained).
The following measures were used to evaluate maternal mental illness and the mother–infant relationship.
Clinical interview
All women admitted to the unit were interviewed by a consultant psychiatrist and a psychiatric trainee. DSM-IV diagnoses were made based on the admission interview and observations made of the patient during admission. Following discharge, the discharge summary was reviewed to determine principal diagnoses as well as the presence of Axis II disorders or traits.
Self-report scales
All consenting women were asked to complete the following measures at admission and again at discharge:
Edinburgh Postnatal Depression Scale (EPDS), 12 a scale well validated with postnatal populations;
Beck Anxiety Scale (BAS); 13
McLean Screening Instrument for Borderline Personality Disorder (MSI-BPD); 14 (the latter two instruments were chosen for their validity and widespread acceptance with general populations as no specific well validated perinatal measures were found);
Maternal Postnatal Attachment Scale (MPAS), 15 designed to assess the strength of the mother’s emotional response to her infant (under 12 months) across a number of dimensions relating to parent-to-infant attachment and widely used with postnatal populations.
Data analyses
Comparisons for significance of difference between admission and discharge questionnaires were made using repeated measure two-tailed t-tests. SPSS was used for data analysis.
Results
Self-report scales were completed at admission by 89 women admitted to the unit (76%). Not all women completed any or all of the questionnaires at the time of discharge.
The average age of women admitted to the MBU was 29.95 years (± 6.45), with the average age of the infant being 7.82 months (± 5.65). The average length of stay was 22.34 days (± 16.73). Twenty-four of the 117 infants were more than 12 months of age.
Diagnoses
Table 1 shows the principal diagnoses made by clinical interview of women. Major depressive disorder was the most frequent diagnosis (43.6%), and 8.5% an anxiety disorder. Bipolar disorder was the principal diagnosis for 3.4% of women, with 7.7% having a diagnosis of schizophrenia or psychosis not otherwise specified (NOS) and 2.6% puerperal psychosis.
Principal diagnoses of women admitted to the Mother–Baby Unit (N=117)
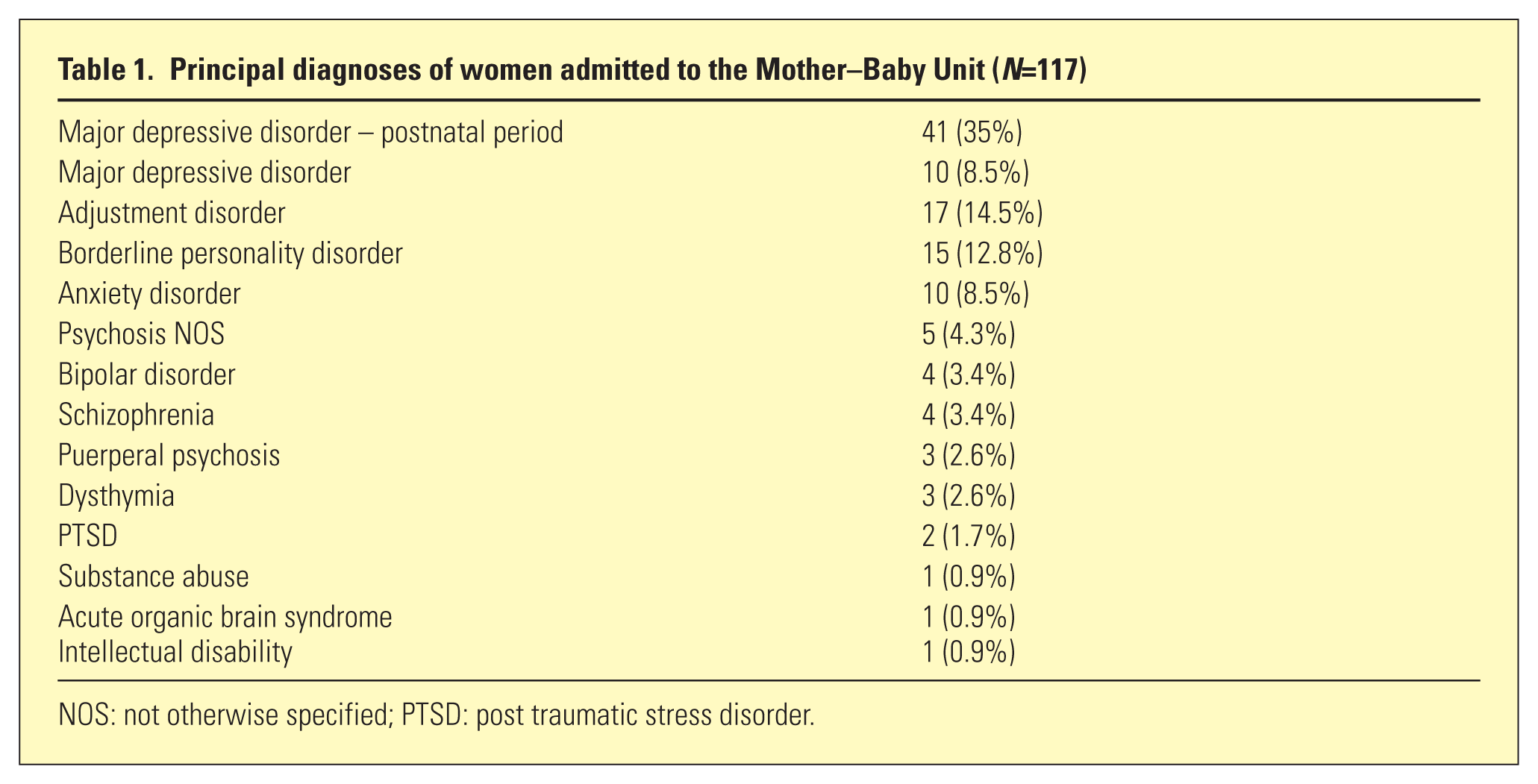
NOS: not otherwise specified; PTSD: post traumatic stress disorder.
Fifteen women (12.8%) were found to have a principal diagnosis of borderline personality disorder (BPD). Twelve other women had BPD co-morbid with an Axis I diagnosis. Overall 23.1% of admitted women had a clinical diagnosis of BPD, with a further 13 (11.1%) being described as having substantial BPD ‘traits’ although not fully satisfying a DSM-IV diagnosis.
This was further supported by the self-reported MSI-BPD, with 34 of 73 women (46.6%) who completed this scale at admission reaching or exceeding the cut-off score for a potential diagnosis of this condition. Fourteen of 36 women (38.9%) still reached the cut-off score for a potential diagnosis of BPD at discharge.
Changes in maternal mental health
Thirty-six patients completed the MSI-BPD at both admission and discharge, 35 the EPDS and 37 the BAS. Significant improvement from admission to discharge was found for all measures including depression (EPDS: t(34) = 5.92, p < .001), anxiety (BAS: t(36) = 5.06, p < .001) and BPD symptomatology (MSI-BPD: t(34) = 2.88, p = .007).
Changes in the mother–infant relationship
Results for mothers with infants younger than 12 months showed significant improvement in the mother–infant attachment relationship from admission to discharge (MPAS: t(27) = 2.95, p = .006).
Discussion
Like previous reports, the results of this study suggest that depressive illnesses (46.2%) are the most prevalent conditions leading to admission to this MBU. Improvements in symptoms of depression and anxiety occurred between admission and discharge, and in the self-reported mother–infant relationship.
Rates of psychotic (10.3%) and bipolar disorders (3.4%) were generally lower than for other MBUs studied despite this MBU admitting most known cases of severe psychotic illness in postnatal women in South Australia. Reasons for this disparity are unclear although it is clear that women with schizophrenia treated by community mental health teams are proactively provided contraception wherever acceptable and many women with bipolar mood disorder frequently have active prophylaxis to prevent postnatal relapse. In addition, this MBU admits infants up to the age of three years whereas most MBUs admit only infants who are not yet perambulatory or they have a cut-off age of one year. Other differences may be related to socio-economic variance as private psychiatric admissions are almost unavailable in South Australia.
A relatively high proportion of admitted women had a primary or co-morbid diagnosis of BPD, similar to that found by Wilson et al., 7 and the most prominent finding was that rates of BPD (23.1%) were generally much higher than in other studies. This may be for a number of reasons including:
As this MBU admits infants up to the age of three years, a different diagnostic profile may be seen.
Not all previous studies may have published all co-morbid diagnoses.
Some MBUs may specifically exclude women with BPD, 6 due to prevailing perceptions that Axis II diagnoses are untreatable, with mental health staff holding stigmatised attitudes towards patients with BPD. 16
Increasing knowledge on three separate fronts may make it more urgent to actively identify BPD in mothers, and offer treatment.
First, neurobiological effects such as disturbance of frontolimbic regulatory systems in infants whose mothers have compromised parenting styles such as in BPD have more recently been identified and summarised, 17 suggesting a need to intervene in order to prevent potentially permanent physiological difficulties in the infant’s ability to regulate its emotions. Early intervention to potentially prevent such intergenerational transmission has been suggested by others. 18
Second, many new treatments have been developed over the last two decades to treat BPD, with some showing promising results.19,20
Last, changes as outlined above have led to the development of protocols at a national level in Australia to promote better management of BPD including early identification and appropriate active management plans. 21
In this MBU, therefore, noting the high proportion of women with BPD, specialised protocols have been developed (available by contacting the corresponding author), which promote identification of BPD early in a mother’s admission, followed by the provision of psychoeducational material, family meetings when the patient is agreeable, a further focus on mother–infant interaction, and management plans beyond discharge which focus on ongoing treatment of BPD as well as the parent–infant relationship. When mothers have postnatal depression it is suggested that treating the mother’s depression is not sufficient to ensure an overall positive outcome 22 and that attention to the mother–infant relationship is also appropriate. 23 Treating both the maternal BPD and the mother–infant relationship is the assumed model.
Another interesting finding from this study was that even more women (46.6% at admission and 38.9% at discharge) reached criteria for a possible diagnosis of BPD on the self-report MSI-BPD than were identified clinically. Anecdotally, staff in this unit have noticed that many women, particularly those with diagnosed BPD, struggle with managing their infants when the infant is unsettled, and quickly become emotionally dysregulated themselves. It may be that having to manage a distressed infant somehow ‘activates’ a similar emotional dysregulation as is experienced by individuals with BPD. This may be even more likely for women experiencing an Axis I disorder. Once the Axis I disorder is treated and the mother has learned to manage and deal with her infant’s emotional distress more effectively, however, this activated ‘emotional dysregulation’ may ‘settle down’ again, which may account for the finding that BPD symptomatology reduced significantly from admission to discharge.
Study limitations include small sample size, particularly the number of participants who completed the measures at both admission and discharge, and basing improvements on single self-report measures. Future studies using a structured clinical interview as well as the Marcé checklist and observer ratings of the mother–infant relationship will add reliability to the findings.
Despite these limitations, this study as well as others1,7 identifies a significant proportion of women presenting to MBUs with BPD, a condition which causes the woman herself great distress and potential highly damaging consequences for her infant and family. Recent positive developments in the treatment of BPD along with the knowledge of the intergenerational transmission of problems provide an impetus to promote identification of BPD traits or diagnoses early in a mother’s hospitalisation with a view to more appropriate and ongoing management. Further research in this MBU therefore is focusing on the development of skills for staff in therapies such as dialectical behaviour therapy, 24 which has been shown via controlled clinical trials to have promising results for managing this disorder.19,20
Footnotes
Disclosure
The authors report no conflict of interest. The authors alone are responsible for the content and writing of the paper.
Funding
This research was supported in part by the “Lane Bequest for the benefits of patients at Parkside Mental Hospital – now Glenside Hospital