
Abstract
Objective:
Age correlated changes in mental and physical capacity have contributed to increasing concerns about older physicians’ clinical competence. This paper explores the relationship between age and health in a clinical population referred for fitness for duty evaluations.
Methods:
Fifty cases from an evaluation center performing fitness for duty evaluations were randomly selected. Cases were reviewed for referral reason, demographic information, diagnosis, and recommendations.
Results:
Age ranged from 28–70 (median age of 51, mode of 45).
Eighty-eight percent of cases had a diagnosed medical condition with potential cognitive sequellae.
Conclusion:
While the literature supports performance concerns in aging practitioners, health independent of age, appears to be an important contributing factor. A screening process considering biopsychosocial reserve and professional load while applicable to older clinicians would optimally be implemented for physicians across their careerspan.
The aging of the medical workforce has contributed to concerns about practitioner competency and patient safety. Studies have demonstrated that age is a risk factor for litigation, discipline, poorer clinical outcomes in primary care physicians and surgeons,1–4 poorer prescribing practices in older physicians, 5 and decreased knowledge base and performance on Board certification exams.6,7 Age is also associated with referral for peer assessment, competency evaluations, and lack of benefit in remediation.8–10 These concerns contributed to suggestions for a mandatory retirement age and/or screening of aging physicians to ascertain fitness for duty.
While age does appear to be a risk factor for underperformance, the cause of this correlation is not completely understood. One possible contributory factor to the observed difficulties is normal aging-related change. Age has a greater impact on fluid intelligence, abilities such as novel or abstract problem-solving capability, versus crystallized intelligence, ability associated with learned or acculturated knowledge (Figure 1).11,12 Significant findings in older adults also include heterogeneity of performance and decreases in processing speed.13,14 However, optimism, empathy, resilience, compassion and wisdom remain stable or increase with age. 4 Educational and occupational attainment, physical and social activity, and overall medical and mental health status all are associated with increased resiliency to brain changes. 15
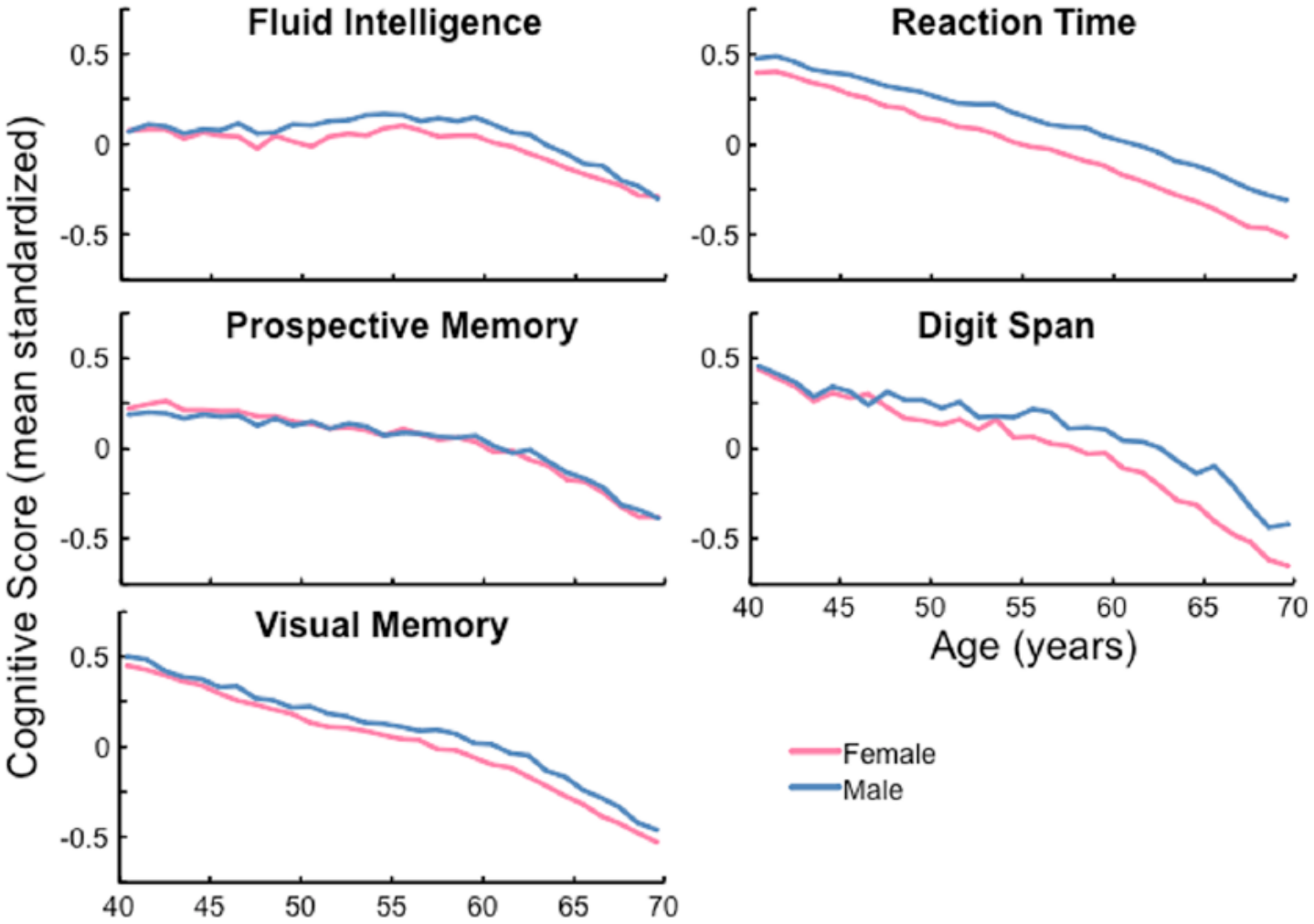
From Moore et al. 12 Relationship between several types of cognitive function and age.
Eva11,16 and others described how age-related changes in cognitive processes might impact diagnostic approach and ability to benefit from professional development opportunities.17,18 Physicians referred for competency evaluations perform less well on neuropsychological tasks especially those associated with executive functioning.18–22 Deficits can manifest as problems with concept formation, organizational skills, set shifting, inhibiting over-learned information, and using feedback.
It is our hypothesis that health challenges are common among physicians who have work-based performance difficulties. We believe that maintenance of wellbeing is central to professionalism for the physician population and that the link between health and performance is better conceptualized as a life-span rather than age issue.
Methods
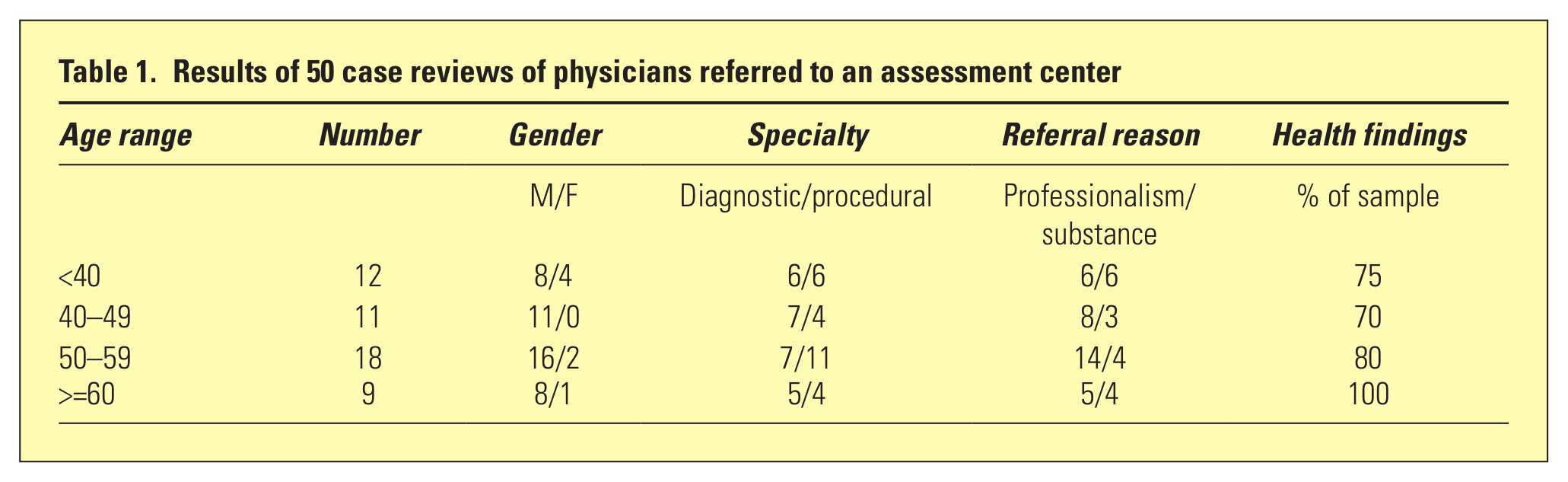
The authors randomly selected 50 cases referred for evaluation and/or treatment for performance problems to a center specializing in fitness for duty evaluations of physicians in training and in practice (see Table 1). Practitioners in this study were not selected based on age. Primary referral reasons were not associated with clinical competency, aging or a medical health concern.
Results of 50 case reviews of physicians referred to an assessment center
Results
Eighty-eight percent of the cases were diagnosed with a medical condition that could have neurocognitive sequellae. All were referred for issues surrounding professionalism, with the vast majority referred for behavior that disrupted the functioning of their system (see Table 1). The age ranged from 28–70 (median age 51, mode 45). Over 80% were males.
The cases represent the entire continuum of physicians, from undergraduate to late career. Representative synthesized case examples are presented.
Expanded case examples
Dr. A is a 51-year-old physician referred for fitness for duty (FFD) evaluation for disruptive workplace behavior. He demonstrated poor interpersonal and communication skills, tardiness in seeing patients, and chart incompletion. Results of neuropsychological evaluation (age and education corrected) were significant for impaired processing speed and difficulties on tests of executive functioning with other areas of performance Average or above. Previously unidentified risk factors for cognitive dysfunction included sleep apnea, Vitamin D deficiency, and chronic work stress. Medical conditions were addressed and repeat neuropsychological testing post stabilization showed no areas of impaired performance. One-year post intervention the workplace reports no issues.
Dr. B is a 69-year-old married primary care physician referred for more than ten years of disruptive workplace behavior. Events include demeaning communications with nursing staff, delayed responses to telephone requests, and throwing objects. Results of the FFD evaluation were negative for medical or psychiatric conditions. Neuropsychological testing (age and education corrected) was Average or better. However, he did poorly on a knowledge test assessing importance of communication, interprofessional teams, and recent changes about behavioral comportment. He completed a remedial education course designed to increase insight into causes/costs of disruptive behavior, develop stress-management and communication skills, and promote translation of knowledge and skills into practice. Sixteen months post intervention he continues to do well.
Discussion
Findings support that a large number of referred practitioners have health challenges that could contribute to performance difficulties. Reportedly only one third of physicians have a primary care physician 23 and physicians generally do not follow preventive health guidelines. 24
Several Codes of Ethics assert that it is the physician’s responsibility to engage in self-assessment of health, wellbeing, and practice. The American and Canadian Medical Association Codes of Ethics charge physicians to recognize and intervene when a colleague appears to have health or practice difficulties. However, physicians are poor at self-assessing and poor at seeking assistance for colleagues.25–30 This has contributed to concerns in the United States about physicians’ ability to self-regulate. 31
In the United States, certifying and credentialing agencies have recently begun implementing programs to assure competence of Board-certified and hospital credentialed practitioners throughout the careerspan.32,33 There is interest in conducting mandatory age-related health and competency screening but disagreement about the necessity and age this process should begin remains.4,34 A more appropriate and acceptable approach is to include health and wellbeing screens throughout the careerspan in currently established approaches used for hospital credentialing. This process allows for more focused reviews if indicated. 33
Such reviews could be achieved through multidisciplinary FFD examinations provided as part of the existing credentialing framework.
Conclusion
Our FFD evaluation approach includes determining areas of strength and weakness, factors contributing to each, and providing recommendations for remediation and support. Current results support the importance of assessment for medical conditions and psychiatric/psychological issues including, but not limited to, substance use disorders, mood disorders, anxiety disorder, personality styles, burnout, and compassion fatigue. Comprehensive neuropsychological testing, clinical observations, evaluation of developmental factors, external stressors and supports, and work and family system factors are also important. Practice specialty and style (hours, patient load and mix, complexity and demand, call schedule, etc.), methods of maintaining currency, work life balance, and physical and mental health should also be assessed. Collateral data collection can clarify system factors and ecological validity of data collected within the evaluation center.
Providing feedback and allowing the practitioner to participate in groups with other practitioners in difficulty helps the clinical team clarify the referred physician’s level of insight into referral reasons, contributing factors and acceptance of next steps. When retirement is recommended, assistance with closing a practice is often required.
Our work suggests that health is an under-identified threat to physician performance across the life/careerspan. Pesiah’s approach described in this volume provides an excellent classification system organizing these issues. We extended her approach to include Practice Performance and Health Problems (see Figure 2). One would expect an increasing proportion of late career physicians with health deficit based underperformance.
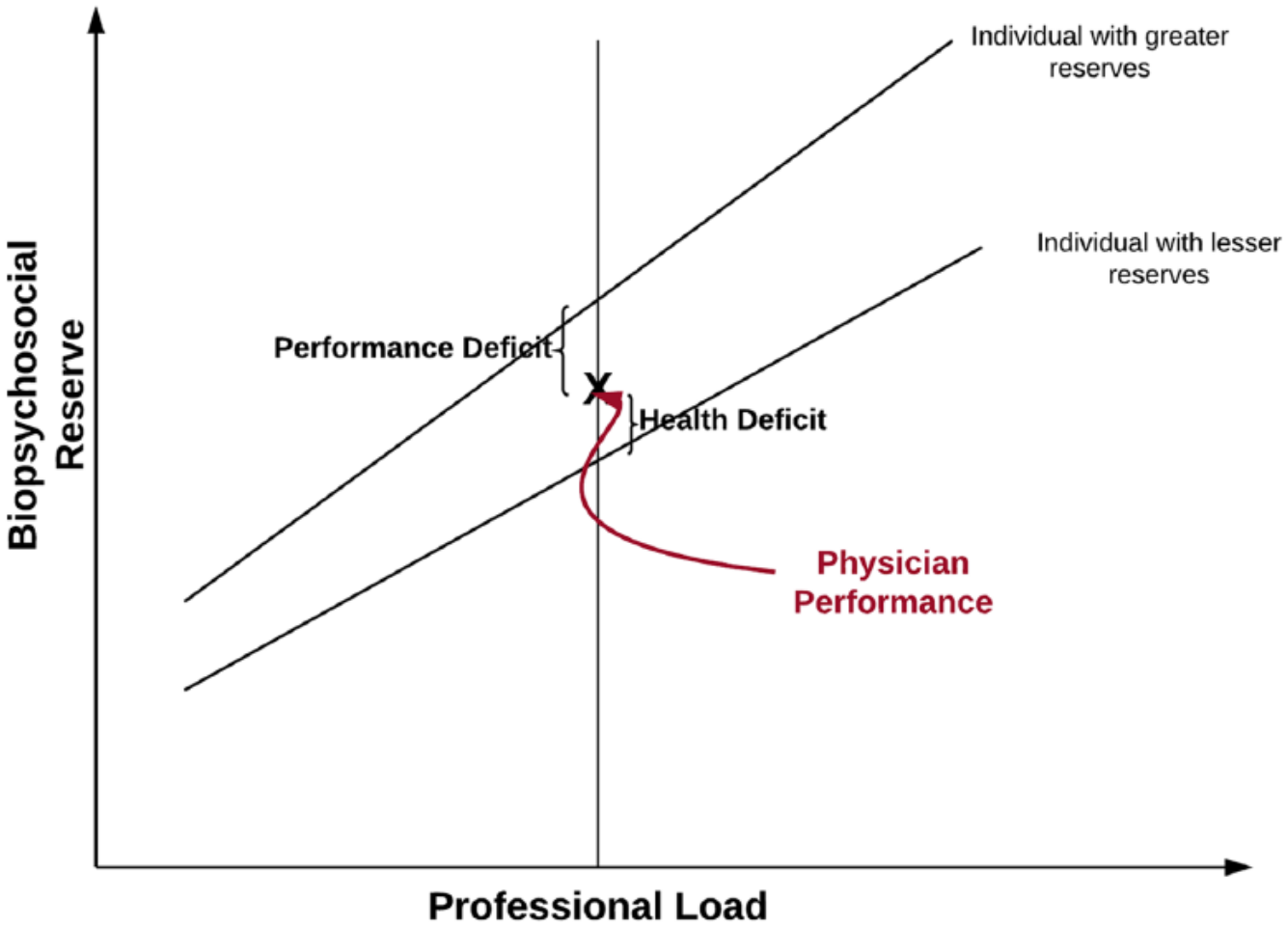
After Pesiah, underperformance related to Biopsychosocial Reserve and Professional Load.
Durning and collegues 35 note: “Taken together the impact of aging on cognitive performance can not be assumed to affect all physicians equally and frameworks that can account for complex interactions between factors contributing to cognitive performance are needed.” Mandatory age related screening does not account for the heterogeneity associated with age or the many factors contributing to underperformance across the lifespan. While we understand concerns related to aging practitioners, challenges to patient safety and outcome must be vigorously addressed whenever in the careerspan they occur. Increased emphasis on health and wellness as direct challenges to performance quality in the medical workforce should be addressed across the lifespan.
Footnotes
Disclosure
The authors report no conflict of interest. The authors alone are responsible for the content and writing of the paper.