
Abstract
Objective:
To develop and test a self-reported scale designed to measure the antecedents of depression.
Methods:
Participants of the Sustainable Mastery of Innovative Lifelong Exercise (SMILE) Tai Chi program were invited to complete the scale for antecedents of depressive symptoms. The scale included questions regarding events/factors the participants have experienced over the past three months and preceded their depressive symptoms. The reliability of the questions was assessed using the Cronbach’s alpha. Principal components analysis was used to examine if there were domains of interest across the scale questions.
Results:
A total of 126 participants completed the scale. The scale had a good internal consistency (Cronbach’s α = 0.82). Principal components analysis identified three components (life events, psychosocial problems, and physical/health problems) in the scale and the components detected the root categories of depression in more than 56% of the cases.
Conclusions:
This simple self-administered scale has proven to provide a reliable measure for the antecedent factors of depression in the SMILE Tai Chi cohort; further validation of the scale in different settings is encouraged.
Depression is a common mental disorder, with an estimated 350 million people of all ages affected worldwide. 1 Depression is also an independent risk factor for heart disease, 2 with growing evidence of a bi-directional relationship between depression and a range of physical illnesses such as heart disease, stroke, diabetes, cancer, arthritis, osteoporosis, and obesity.3,4 Findings from the World Health Survey conducted by the World Health Organization indicate that depression is a leading cause of disability. 5 Furthermore, depression is associated with the greatest decrement in health of any chronic disease, and co-morbid depression incrementally worsens other health problems more than many other disease combinations.5,6 In addition, the Longitudinal Investigation of Depression Outcomes study has reported that depression is associated with a 17%–46% increase in healthcare costs. 7
The identification of patients with depression through a scale is the first step towards the start of the therapy, followed by the identification of the antecedent(s) that triggered the depressive episode. The life events and personal risks causing depression were reported previously; 8 however, to our best knowledge there is no reliable scale available that identifies the antecedents of depression. For that reason, researchers from the Sustainable Mastery of Innovative Lifelong Exercise (SMILE) Tai Chi program developed a self-reported scale designed to measure the antecedents of depression.
Methods
The SMILE Tai Chi Program received ethical approval from the Human Research Ethics Committees of both Princess Alexandra Hospital and The University of Queensland. The SMILE Tai Chi program 9 recruited participants using a wide range of methods, such as advertisements and referral from primary care physicians/general practitioners (GPs), from October 2009 to March 2010.
The eligibility criteria included: (1) age between 18 and 80 years; (2) depression (diagnosed by GPs); (3) being on antidepressants for depression or having a short form of the Center for Epidemiological Studies Depression Scale (CES-D10) rating score of 10 or higher; 10 and (4) having central obesity (waist circumference more than 95 cm (men) and 80 cm (women)) and/or body mass index of more than 30 kg/m2). 11 The CES-D10 scale was selected for depression screening among the participants because this scale has proven to be well accepted by the general population, it has been validated in the general population (not just in psychiatric inpatients), and has a high internal consistency. 12 The cut-off point of CES-D10 ≥ 10 was selected as it has a sensitivity and specificity of 96% and 100%, respectively. 10 Only patients with central obesity were enrolled because the one of the SMILE Tai Chi program objectives was to examine the effect of Tai Chi on obesity. Exclusion criteria included contraindications to physical activity, mental illness other than depression (such as bipolar disorder or schizophrenia), any severe or acute general medical problem, type 1 diabetes, current pregnancy, being within three months’ post-partum, or anticipating pregnancy during the course of the study.
Researchers from the SMILE Tai Chi program designed a scale for antecedent depressive symptoms which consisted of 11 questions (see Appendix 1). The SMILE Tai Chi program researchers consisted of a psychiatrist, a complementary and alternative medicine expert, a cardiologist, a mind-body movement therapy expert, and a biostatistician. The SMILE scale was developed based on ‘the life events and personal factors that put a person as risk’ from beyondblue, Australia. 8 Participants of the SMILE Tai Chi program were asked to complete the SMILE scale for antecedent depressive symptoms between August and December 2010; the participants were instructed to use a 4-point scale (ranging from 0 to 3, with 3 indicating higher frequency) to rate the extent to which the events and/or factors experienced over the past three months have interfered with/caused their depressive symptoms.
The internal consistency (reliability) of the 11 questions of the SMILE scale for antecedents of depressive symptoms was determined by the Cronbach’s alpha coefficient. Principal components analysis was used to assess if there were domains of interest across the scale questions. 13 A varimax rotation with Kaiser normalization was used to maximize the sum of the variances of the square loadings. 14
Results
A total of 126 participants completed the SMILE scale for antecedent depressive symptoms. Among the 126 participants, 76% were female and the overall age ranged from 28.89 to 76.78 years (mean 53.88 years, standard deviation (SD) 9.74 years). Seventy percent of the participants were on antidepressant medication and the patients’ CES-D10 score range was 0 to 30 (mean 13.98, SD 6.76). Twenty-six participants had a CES-D10 score of 10–14 (moderate depressive symptoms); whereas, 70 participants had a CES-D10 score >14 (severe depressive symptoms).
The SMILE scale for antecedent depressive symptoms scores ranged from 0 to 33 (mean 12.7, SD 6.6). The scale had a good internal consistency (Cronbach’s α = 0.82) for the 11 questions (see Table 1). Principal components analysis with the varimax rotation identified a three-component solution that accounted for 56.1% of the explained variance. The three components were life events, psychosocial problems, and physical/health problems. The mean values of the 11 questions across these three groups in descending importance were 6.17 (SD 3.84) for the psychosocial problems group, 5.20 (SD 2.92) for the life events group, and 1.37 (SD 1.31) for the physical/health problems group, respectively.
Internal consistency of the components and principal component analysis of the SMILE scale for predictors of depression
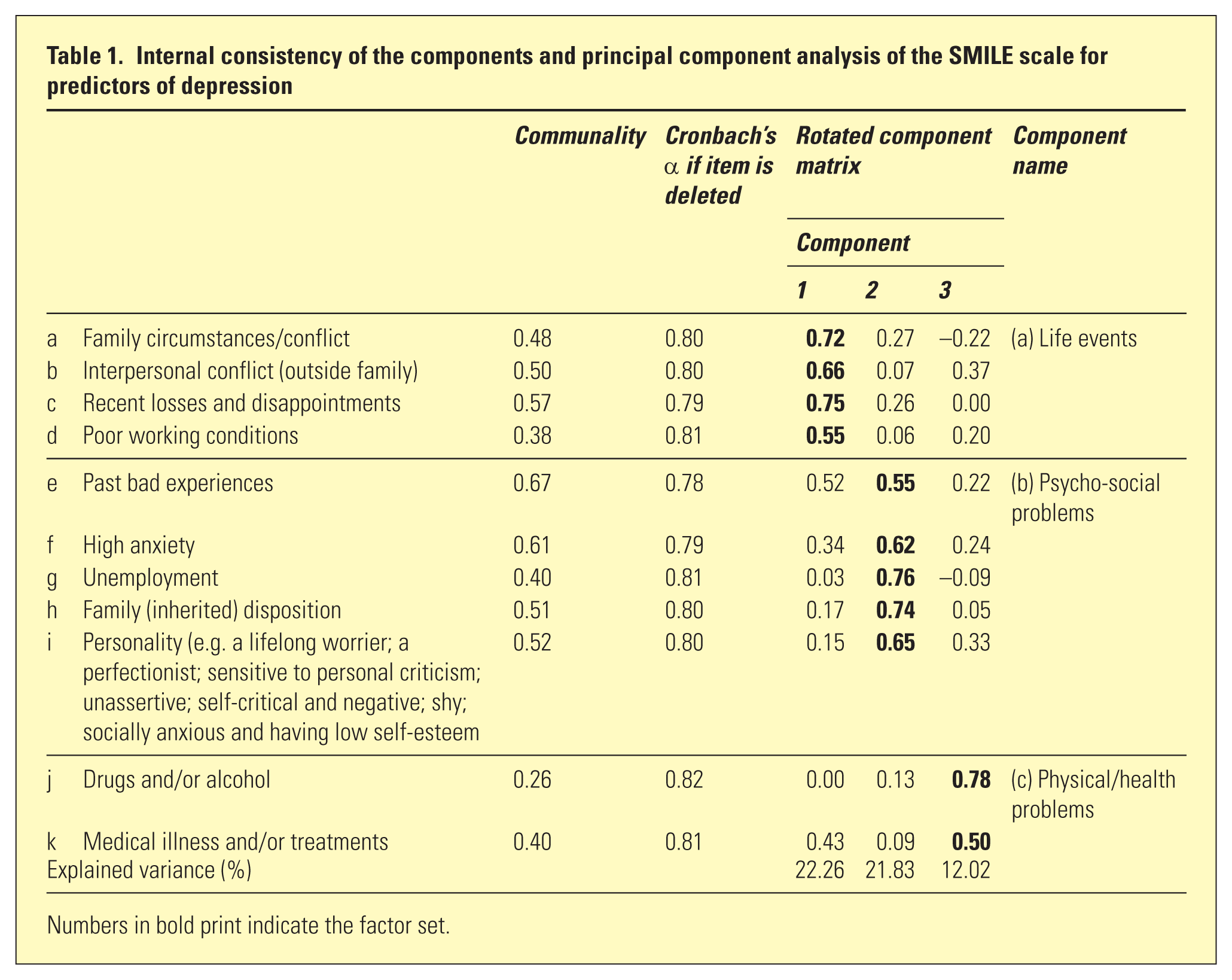
Numbers in bold print indicate the factor set.
Discussion
Several screening scales for affective disorders have been developed throughout the years;10,12,15–17 however, for the first time a self-administered reliable scale that measures the antecedent factors of depression has been developed and successfully tested. The results indicate that the SMILE scale for antecedent depressive symptoms identifies three main antecedents of depressive symptoms: life events; psychosocial problems; and physical/health problems. These three domains identify the root categories of depression in a primary care setting in more than 56% of the cases.
There were several limitations in our study. First, the SMILE scale for antecedents of depressive symptoms was administered once; thus, the test-retest reliability (intra-class correlation coefficient) was not assessed. Second, the SMILE scale for antecedents of depressive symptoms has not yet been validated in a different cohort of patients. Finally, the patients were recruited based on depression identified by GPs (not a psychiatrist) and being on antidepressants for depression and/or depression scores above a pre-determined threshold; therefore, the participants were likely to be experiencing a range of depressive disorders. While this may potentially limit the generalizability of our findings to a specific diagnostic category of depression, such as major depressive disorder, our findings are relevant to the population of depressed patients seen in primary care.
The SMILE scale for antecedents of depressive symptoms is a simple and reliable self-administered scale to detect the antecedent factors of depression. For future studies, we recommend that the scale should be reported in terms of sub-scores for the three sub-groups (life events, psychosocial problems, and physical/health problems).
Footnotes
Appendix
SMILE scale for antecedents of depressive symptoms.
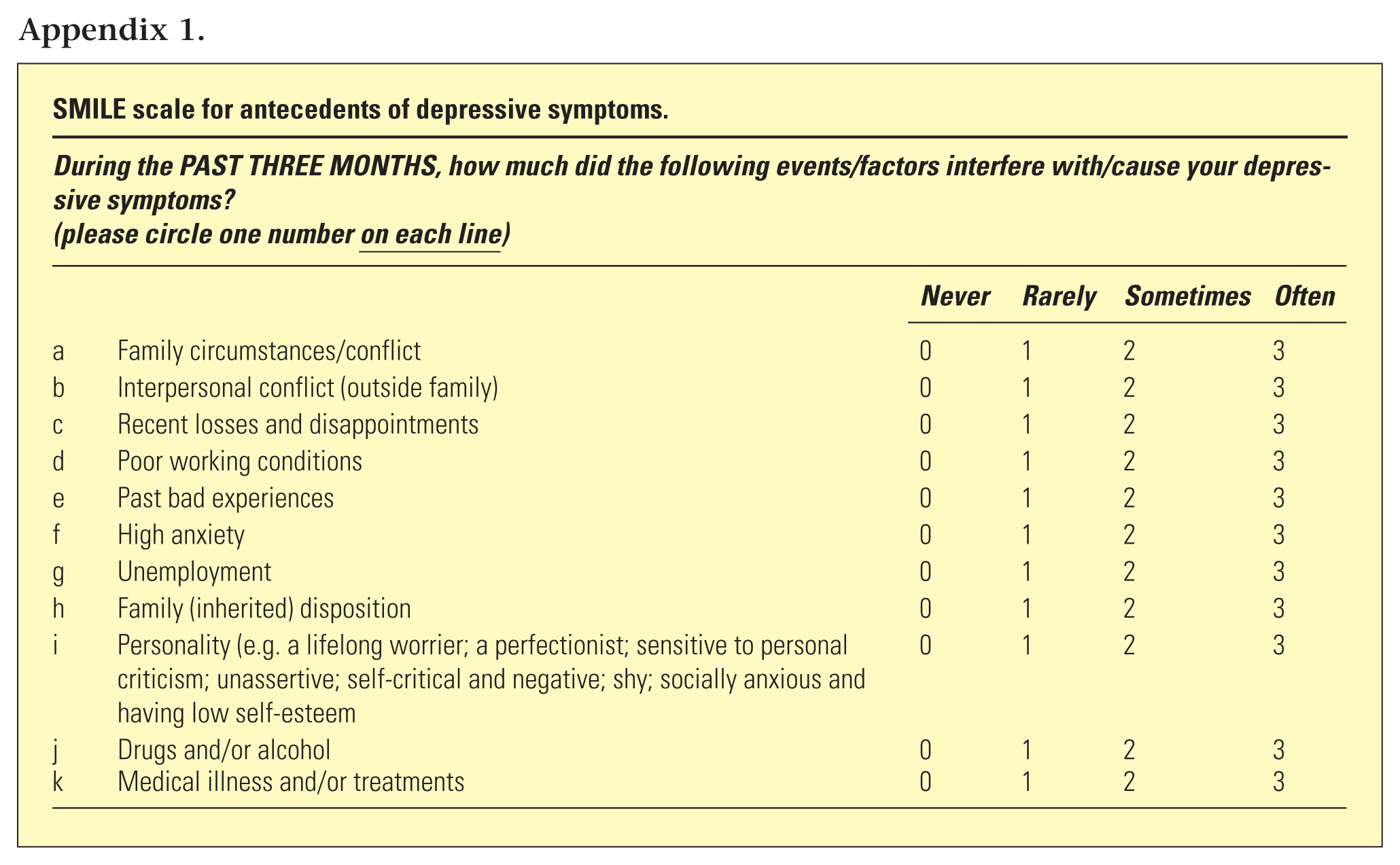
| During the PAST THREE MONTHS, how much did the following events/factors interfere with/cause your depressive symptoms? |
|||||
|---|---|---|---|---|---|
| Never |
Rarely |
Sometimes |
Often |
||
| a | Family circumstances/conflict | 0 | 1 | 2 | 3 |
| b | Interpersonal conflict (outside family) | 0 | 1 | 2 | 3 |
| c | Recent losses and disappointments | 0 | 1 | 2 | 3 |
| d | Poor working conditions | 0 | 1 | 2 | 3 |
| e | Past bad experiences | 0 | 1 | 2 | 3 |
| f | High anxiety | 0 | 1 | 2 | 3 |
| g | Unemployment | 0 | 1 | 2 | 3 |
| h | Family (inherited) disposition | 0 | 1 | 2 | 3 |
| i | Personality (e.g. a lifelong worrier; a perfectionist; sensitive to personal criticism; unassertive; self-critical and negative; shy; socially anxious and having low self-esteem | 0 | 1 | 2 | 3 |
| j | Drugs and/or alcohol | 0 | 1 | 2 | 3 |
| k | Medical illness and/or treatments | 0 | 1 | 2 | 3 |
Acknowledgements
We are grateful to all the participants that took part in this study.
Funding
This work was supported by beyondblue and the National Heart Foundation (G 088 4034). The study sponsor had no further role in the study design and collection, analysis, and interpretation of data, or in the writing of the article and the decision to submit it for publication.
LFK is funded by an Endeavour Postgraduate Scholarship (#3781_2014), an Australia National University Higher Degree Scholarship, and a Fondo para la Innovación, Ciencia y Tecnología Scholarship (#095-FINCyT-BDE-2014).
Disclosure
The authors report no conflict of interest. The authors alone are responsible for the content and writing of the paper.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.