
Abstract
Objectives:
The objective of this study was to offer some personal observations as to how melancholia can be diagnosed and differentiated from the non-melancholic depressive conditions.
Methods:
Personal clinical and research-based observations are presented following a critique of common current strategies.
Results:
The paper offers views on the most differentiating clinical features, argues for adding illness course variables to symptoms and provides details of the Sydney Melancholic Prototypic Index, a measure with a high overall classification rate in differentiating melancholic and non-melancholic depression.
Conclusions:
Greater precision in differentiating melancholic from non-melancholic depression is advanced by weighting signs and symptoms of psychomotor disturbance, as well as including illness correlates and family history in the diagnostic process.
Keywords
Melancholia is variably accepted or disregarded by mental health professionals as a condition. Its ‘believers’ variably position it dimensionally (i.e. as a more ‘severe’ type of clinical depression) or categorically, with the latter reflecting the long-standing binary model that views melancholic/endogenous depressive and reactive/neurotic as two distinct and contrasting depressive ‘types’. My personal view is that melancholia is a categorical type of depression that may manifest as a psychotic or a non-psychotic state and that it is particularly prevalent in those experiencing bipolar depressive episodes. Its initial description is commonly attributed to Hippocrates in the 5th century BC and, for more than 2000 years, it was seen more as a movement disorder than a mood disorder, in light of its distinctive overt signs of psychomotor disturbance (PMD). 1 In the 20th century melancholia accrued a number of ascriptions, 2 including that, and in comparison to non-melancholic depression, it (i) principally had genetic and biological rather than psychosocial determinants, (ii) had a relatively distinct pattern of clinical symptoms, (iii) showed a minimal response to placebo (in the order of 10%) and (iv) had a superior response to physical treatments such as antidepressant medication and electro-convulsive therapy rather than to psychotherapy.
Formal strategies for diagnosing melancholia
In recent years, melancholia has been increasingly viewed as a disorder of neuro-circuitry, reflecting perturbed neurotransmitter functioning impacting on mood, cognition and psychomotor parameters 3 and disrupted connectivity of cortical systems. 4 Attempts at its definition and precise diagnosis have been problematic. Multivariate analyses conducted over several decades generated a large set of so-called ‘endogeneity’ symptoms that were viewed as defining the condition. As quantified in an early study, 5 while many such symptoms (e.g. weight change, insomnia, impaired libido) are common in melancholic depression, they are also common in non-melancholic depression and in other states (e.g. anxiety). Thus, if such items are included in melancholia diagnostic indices (as commonly occurs), their non-specificity swamps the capacity of truly differentiating items to accurately assign patients to a diagnosis of melancholic or non-melancholic depression.
DSM-5 criteria also have limitations. In DSM-5, 6 melancholia is accorded ‘specifier’ as against ‘sub-type’ status, which automatically compromises its clear differentiation from major depression itself. In addition, a number of DSM-5 depressive symptoms (e.g. PMD, weight loss, anhedonia, early morning awakening, excessive or inappropriate guilt) are criteria for both melancholia and for major depression. As major depression is the broad generic diagnosis, it would have been logical to require patients with melancholia to first meet criteria for major depression symptoms and then to meet a differing set of symptom criteria that have specificity to melancholia itself. The consequence of the current DSM-5 model is that there is minimal differentiation between those who are assigned a diagnosis of major depression with melancholia and those assigned a diagnosis of major depression without melancholia. This muddies the diagnosis of ‘true’ melancholia while also leading to an increased risk of ‘over-diagnosing’ melancholia. Thus, studies that seek to pursue the causes and optimal treatments of melancholia are clearly compromised if DSM-5 criteria are used.
I have spent several decades seeking to develop a refined set of diagnostic features for circumscribing and diagnosing melancholia. Pursuing the long-standing observation that melancholic patients are highly likely to show signs of PMD led us to develop the CORE measure, and which requires raters to judge the presence and severity of 18 signs of cognitive disturbance and of motoric change (i.e. retardation and agitation). In comparison with traditional endogeneity symptoms, CORE signs proved a distinctly superior differentiation and, in one key study, 7 met criteria for ‘necessary and sufficient’ status. In essence, those we studied who had clinically defined melancholia universally showed signs of PMD – the ‘necessary’ component – while adding endogeneity symptoms to CORE signs did not improve differentiation of those with melancholic from those with non-melancholic depression, indicating that CORE signs were sufficient in and of themselves.
There were, however, two key limitations to the application of the CORE measure. Firstly, not all patients are at the nadir of their episode when they present for clinical assessment (and might even be in remission), risking invalid rating of signs at such times. Secondly, the majority of the patients we studied were over the age of 40. In patients with melancholia under the age of 40 (and particularly adolescents), overt PMD is less distinctive and less severe. We therefore judged that we needed to move beyond measuring PMD signs, and returned to pursuing a set of symptoms with distinctive specificity. A representative study 8 generated overall classification rates (in distinguishing those with melancholic and non-melancholic depression) in the order of 67%. As such, differentiation was sub-optimal. Thus, we elected to add illness correlates to the refined set of symptoms, a strategy akin to that of the old Newcastle Index, 9 and so developed a self-report measure termed the SERDEX, 10 and with the latter – with self-report and clinician-rated versions – then named the Sydney Melancholia Prototype Index (SMPI). 11
The clinician-rated SMPI (see Figure 1) requires clinicians to rate 24 descriptors. These comprise two equal sets of 12 symptoms and illness correlates that show specificity to melancholic and non-melancholic depression, respectively. Such ratings collate material already garnered in standard clinical interviews and, therefore, SMPI completion generally takes only a minute or two for the clinician to complete. At the bottom of the form the clinician or researcher is able to estimate an overall prototypic rating. In the development study 11 we established that for the clinician-rated form, affirming four or more descriptors in the left-hand column than the total affirmed in the right-hand column had a high classification rate (i.e. sensitivity of 0.84, specificity of 0.92 and respective positive and negative predictive values of 0.90 and 0.88). Such a level of classificatory accuracy is impressive but not perfect. Further, there is no laboratory test or gold standard against which SMPI-allocated diagnoses can be referenced. While disappointing, this scenario is not dissimilar to many medical conditions, with Parkinson’s disease being an exemplar. 12 Parkinson’s disease also requires clinician judgement as there is no definitive laboratory test and, while it possesses some common features, it has several differing phenotypic presentations. Neurologists recognise such limitations and so they not only assess the presence or absence of certain symptoms with differing prototypic pictures but also build in illness course variables. Therefore, we view the differentiation of melancholic and non-melancholic depression as requiring a similar approach and suggest that the SMPI assists such a process by operationalising clinical diagnostic judgment.
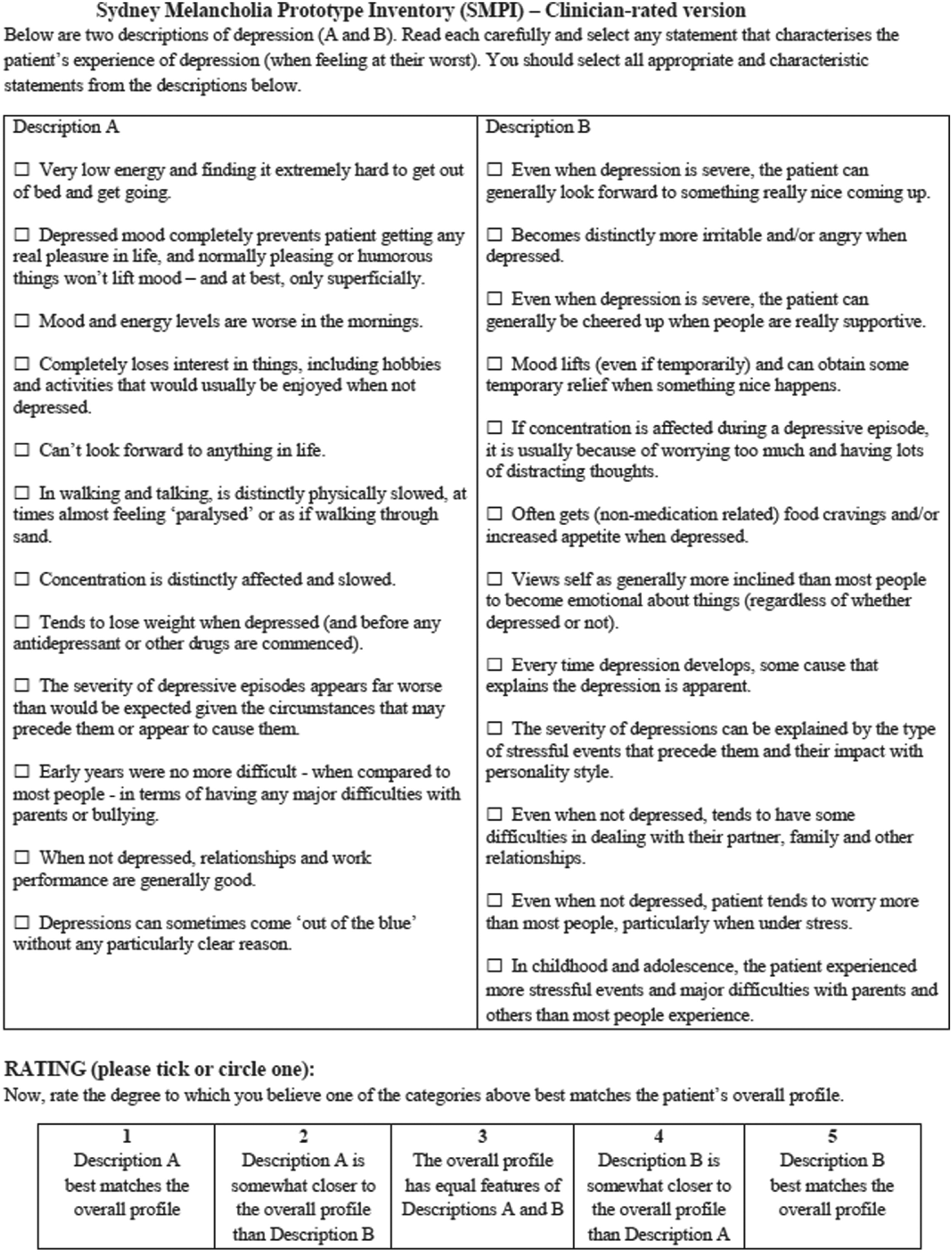
The clinician-rated SMPI.
Personal strategies for diagnosing melancholia
While the SMPI captures most of the symptoms that I personally find useful to identify melancholia, there are some nuances to their identification in a clinical interview. I usually start by asking the patient whether, when depressed, they have a non-reactive and anhedonic mood – although both can be difficult to rate. For example, some patients with clear-cut melancholia will observe that such symptoms, when present, are not absolute and that they can be cheered up to some extent by some events (e.g. playing with a grandchild). I then pursue anergia, asking if they ‘find it difficult to get out of bed and get going’. While that weights PMD, it is possible that patients with a non-melancholic depression may simply lack motivation and thus acknowledge difficulty getting out of bed. Thus, there is a need to pursue how the anergia actually impacts on the patient. Those with melancholia will report that it is not explainable by a simple lack of motivation and that it is physically difficult to get out of bed. Pursued, they will generally report features such as going from their bed to a sofa or, as a consequence of the anergia, failing to wash or bathe for several days. I then ask if there is any diurnal variation, and expect that the great majority of those with melancholia will report their mood and energy levels as worse in the mornings. In response to questioning, the majority of depressed patients will report impaired concentration. In non-melancholic depression it is most often experienced as poor attention and distractibility, and underpinned more by anxiety than by depression. In melancholia, there is a differing quality to it, in that the person acknowledges the direct question about their thinking being ‘foggy’, making it hard for them to take in and remember things, with one patient reporting that ‘while I normally cook the evening meal, when I’m depressed I can’t remember the recipe for an omelette’. Psychomotor slowing also weights a melancholic depression as evidenced by the person feeling as if they are ‘walking through sand or molasses’, and tending to be monosyllabic or with a diminished voice tone range. I am particularly struck by melancholic patients losing the ‘light’ in their eyes during depressive episodes. The last feature is clearly best determined by interviewing a relative but, at times, can be detected at clinical interview, particularly if the clinician moves attention away from the patient to talk to a family member. Finally, a family history of depression, bipolar disorder or of suicide advances the probability of a melancholic depression.
In essence, there appears to be a relatively short list of symptoms that have high specificity to melancholia. As noted, the SMPI lists a number of illness correlates for melancholic and non-melancholic depression. Those with melancholia are more likely to have episodes that come ‘out of the blue’, to have their episodes last longer than would be predicted from any antecedent or potentially relevant stressor, and for its severity to be worse than would be expected from the impact of any preceding or concurrent stressful circumstances. Finally, if asked whether they judge their depression as likely to have psychological, social or biological causes, many will effectively judge it as ‘biological’ in that they perceive it more as being a ‘disease’ imposed on them rather than simply a reaction to psychosocial factors.
I suggest that the diagnosis of melancholia is important in and of itself. As Montgomery observed13:252 about the provision of a diagnosis:
Patients want to know what is wrong, if it’s serious, how long it will last, whether it will alter their life plans…. To know the cause of disease is to have control…[and] just having a diagnosis means that the rest of your life can start.
Equally importantly, the strategies for managing melancholia differ from the modalities weighted for managing non-melancholic depression and thus argue for diagnostic sub-typing. Such management nuances are considered in the accompanying article. 14
Footnotes
Acknowledgements
Editorial assistance was provided by Stacey McCraw and Kerrie Eyers.
Disclosure
The author reports no conflicts of interest. The author alone is responsible for the content and writing of the paper.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research components were supported by a National Health and Medical Research Council (NHMRC) program grant (grant number 1037196).