
Abstract
Objectives:
A single case report on cannabinoid treatment for treatment-resistant Tourette syndrome (TS).
Method:
Our subject received 10.8 mg Tetrahydocannabinol and 10 mg cannabidiol daily, in the form of two oro-mucosal sprays of ‘Sativex®’, twice daily. Assessment was pre-treatment and at week one, two, and four during treatment. He completed the Yale Global Tic Severity Scale as a subjective measure, and was videoed at each stage. The videos were objectively rated by two assessors, blind to the stage of treatment, using the Original Rush Videotape Rating Scale.
Results:
Both subjective and objective measures demonstrated marked improvement in the frequency and severity of motor and vocal tics post-treatment. There was good interrater reliability of results.
Conclusions:
Our results support previous research suggesting that cannabinoids are a safe and effective treatment for TS and should be considered in treatment-resistant cases. Further studies are needed to substantiate our findings.
A difficult-to-treat case
Our subject is a 26-year-old single man who lives with his brother in rented accommodation. He has a 14-year history of Tourette syndrome (TS), with multiple complex motor and vocal tics, including coprolalia. He initially presented to Child and Adolescent Mental Health Services (CAMHS) with obsessive–compulsive disorder and tics, for which he was treated with Fluoxetine. This was later augmented with Risperidone, as well as psychological therapies, due to poor response. There was significant anxiety, and later a mood component, to his presentation. He required one admission to a psychiatric hospital with a major depressive episode and suicidal ideation. This improved; however, his tics and obsessive–compulsive behaviour deteriorated, despite adequate doses of antipsychotics (Haloperidol, Risperidone, and Pimozide), antidepressants (Fluoxetine, Sertraline, Clomipramine, Venlafaxine, and Mirtazapine), mood stabilizers (Carbamazepine, Sodium Valproate, and Lithium), and tranquilizers (Clonazepam), which were either ineffective or not tolerated due to side effects.
TS hugely impacts on our subject’s function; he is unable to cook due to the mess he makes, and takes up to two hours to shower and dress. He has repeatedly damaged property, including breaking a washbasin and putting holes in floorboards and walls. He quickly wears out his shoes and regularly sustains minor injuries from collisions. His condition has caused significant disruption in his life; he has never worked nor had an enduring relationship. Our subject is in good physical health and has never used illicit substances.
Tourette syndrome (TS)
In 1885 Gilles de la Tourette first described this condition. As described in the classificatory system Diagnostic and Statistical Manual V (DSM-5 2013), TS is characterised by multiple motor and one or more vocal tics, lasting more than a year, before 18 years of age. It is associated with psychiatric morbidity and often comorbid with attention deficit disorder and obsessive–compulsive symptoms. The prevalence is 1% of the child and adolescent population, with males more commonly affected. Generally, the condition attenuates with age, but some individuals have persistently severe or worsening symptoms in adulthood that disrupt function and impair quality of life. Sequelae of ongoing tics include musculoskeletal pain, social isolation, vocational restrictions, peer victimization, and interpersonal conflict. 1
An abnormality in corticostriatal–thalamocortical pathways, causing tics and psychiatric comorbidities, has been suggested. There is often a familial history of tics, but mode of transmission and genetic defect have yet been determined. The mainstay pharmacological treatments have been antipsychotics, such as Haloperidol and Risperidone.2,3
Using cannabis to treat TS
In 1988 cannabinoid receptors were identified for the first time in the central and peripheral nervous system of humans. These are found in the basal ganglia, cerebellum, hippocampus, and dorsal primary afferent spinal-cord regions. There is experimental evidence that cannabinoids affect the activity of many neurotransmitters. It is speculated that the central CB1 receptor system might be involved in the pathophysiology of TS through the modulation of dopaminergic neurotransmission. The first evidence to suggest that cannabis could be a useful treatment for TS came from case reports published in 1988 that discussed the improvement in tics and urges in three patients, aged 15–39, who were smoking cannabis. 4 Retrospective questionnaire data for Tourettes patients, comparing symptoms in cannabis users with non-cannabis users, found the former experienced less tics. 5 The 1990s–2000s saw the publication of further case reports of Tetrahydrocannabinol (THC), the main psychoactive component of cannabis, in TS treatment.6–9 Two randomised controlled trials were later carried out, which suggested benefit from THC.10,11
Sativex® is the only pharmaceutical-grade cannabis product currently available in New Zealand. It is derived from the plant Cannabis Sativa and contains an equal 1:1 ratio of THC to cannabidiol (CBD), as well as a range of other naturally occurring cannabis-derived terpenoids. 12 It differs from marijuana grown for recreational purposes in which there is often more THC. Sativex® is available as an oro-mucosal spray with each metered dose containing 2.7 mg of THC and 2.5 mg of CBD. Sativex® is approved for clinical use in the treatment of nausea and vomiting associated with cancer chemotherapy, anorexia in HIV/AIDS, and spasticity in multiple sclerosis. Authority to prescribe Sativex® was granted by the Ministry of Health, recognising that it was an off-licence indication. There are currently no published reports regarding the use of Sativex® in TS and it was chosen, rather than synthetic THC, as it is more easily available and has been shown to be safe. 13 Also, there is some evidence that CBD has been beneficial in the treatment of other movement disorders. 14
We prescribed a fixed dose of two oro-mucosal sprays of Sativex® twice daily for our subject, as previous trials have shown benefit from 10 mg THC. 7 He took this for four weeks and was not taking any other substances or medications at the time.
With consent, we assessed our subject on four occasions; initially prior to commencing treatment, then at week one, two, and four during treatment. Assessment involved completing the Yale Global Tic Severity Scale (YGTSS) (see supplement 1); a subjective scale, rating number, frequency, intensity, complexity, interference, and impairment of motor and vocal tics in the preceding week. Assessment also included a 30-minute videotape of our subject, which followed the same format each week. He completed maths then reading tasks, both at a standard suitable for an 11-year-old, each for 10 minutes. He then spent the remaining 10 minutes sitting in silence. The videos were independently assessed, using the Original Rush Videotape Rating Scale (ORVRS) (see supplement 2), by two raters (DT, LE) who were blinded to the phase of treatment. The ORVRS has been shown to correlate well with scores on the comparable items from the YGTSS. 15 Raters were both psychiatry trainees who had watched videos and read appropriate literature to prepare to formally rate tics. Any discrepancy in scores resulted in both raters watching the video together to reach consensus. If this was not possible then it was agreed that the video would be rated by the third rater (RB), who has worked with TS patients and has used formal tools in rating for previous TS research. 16
Using the ORVRS to evaluate tics, we noted a reduction in motor tics of 85%; from 176 pre-treatment to 27 at week four (Figure 1). His vocal tics improved by 90% from a pre-treatment score of 20 to a score of 2 at week four (Figure 2). As expected, motor tics were highest when performing maths exercises and vocal tics were highest when reading aloud. Both motor and vocal tics were less frequent when sitting still (Figures 2 and 3). The number of body areas affected decreased; from 11 areas pre-treatment, to just two areas by week four. The overall severity scores reflected these improvements, reducing from 5/5 (motor) and 4/5 (vocal) pre-treatment, to 1/5 (motor and vocal) post-treatment. Inter-rater reliability was good, with co-efficients of variation calculated for motor tics at 4.2%, 6.2%, and 15.2% for the three exercises, respectively.
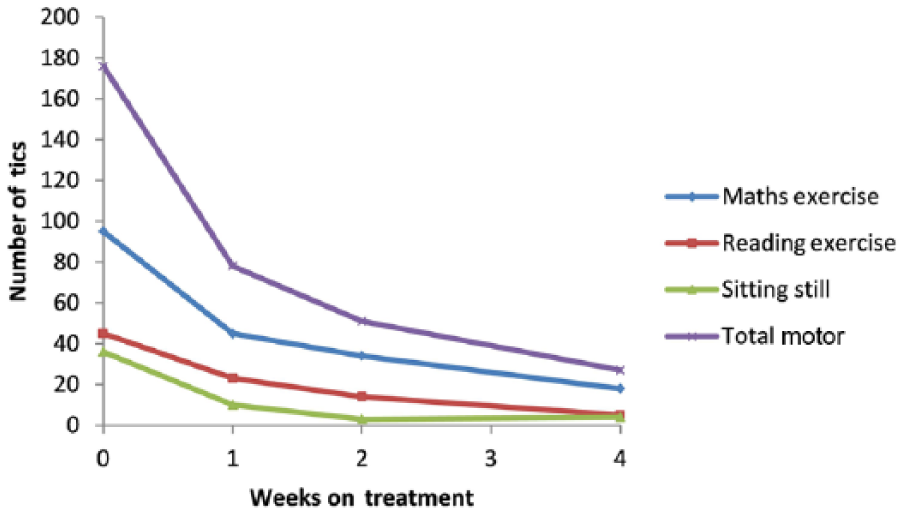
Motor tic count on the Original Rush Videotape Rating Scale (ORVRS).
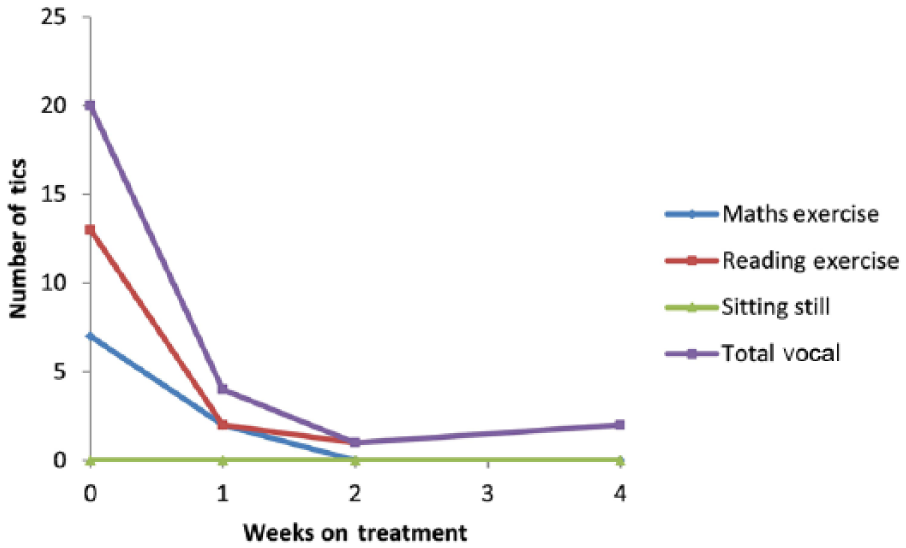
Vocal tic count on the Original Rush Videotape Rating Scale (ORVRS).
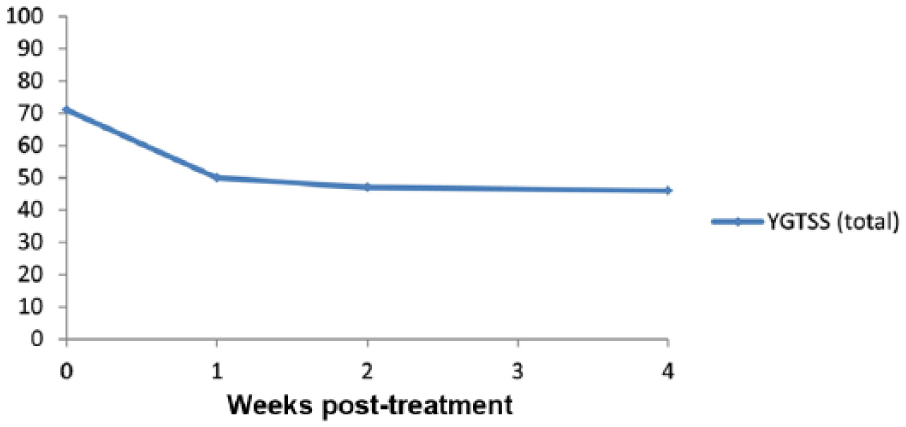
Yale Global Tic Severity Scale (YGTSS).
Our subject’s YGTSS showed a 35% improvement from a pre-treatment score of 71 to a post-treatment score of 46 in week four (Figure 3). Our subject reported that people who knew him in the community, unaware of his new treatment, commented on the improvement in his condition. For the first time he was able to make a cup of tea and cook without making a mess.
Limitations to consider
Tics are often exacerbated by emotional stress. It could be considered that this would be more pronounced pre-treatment, when the process of being filmed was unknown to our subject, compared to week four, when he would be more relaxed. However, this wouldn’t explain the improvement seen in the community, or the subjective rating scores.
Our subject knew he was on active treatment and was aware of the cost and licensing needed to access this novel therapy. This could lead to a larger placebo response compared to previously trialled medications. Furthermore, a Hawthorne effect may have contributed to the results seen.
Caution should also be exercised in extrapolating the findings to other patient groups with tic and other movement disorders.
Comment
TS is a common disorder that can be difficult to treat and may lead to significant psychosocial handicap. Treatment with Sativex® has shown promising early research findings. We documented considerable objective and subjective improvement in tics, which was reflected in our subject’s ability to complete activities of daily living.
The results of the YGTSS are not as marked as the results of the ORVRS. This is largely due to the impairment rating which reflects a ‘moderate impairment’ in functioning on the YGTSS which describes ‘tics associated with clear problems in self-esteem, family life, social acceptance or school or job functioning’ for our subject. Our opinion is that it is unreasonable to expect problems like these to shift in a period of four weeks when the disorder has been severe and longstanding.
As yet, it is unclear whether THC, other active cannabinoids (like CBD), or the ratio between the different cannabinoids, results in the greatest benefit. Furthermore, there remains uncertainty around whether herbal cannabis, or different natural or synthetic cannabinoids, have the best efficacy to adverse effect profile. Sativex® was well tolerated by our patient and led to a rapid and sustained response. Hypothetical concerns about impaired cognitive performance with cannabinoid treatments have been raised by some and refuted by others. 17 In our case there were no adverse effects. It could be argued that the long-term treatment of a vulnerable patient population with cannabis may be unwise; given the increased risk of psychosis with long-term cannabis use. 18 This risk is greater with earlier age of use and higher potency cannabinoids. 19 In the adult population, low-dose Sativex® may minimise this risk, but vigilance is recommended. It should be considered that some sufferers of TS may choose to use cannabis illicitly if there are no alternatives for symptom control, leading to increased risk of adverse health outcomes. 20 To date, clinical trials of Sativex® have not noted any cases of abuse or diversion 13 and tolerance has not been observed.
Key points
TS may manifest as minor, mild, or benign forms through to a severe form of movement disorder with associated functional impairment, self-esteem difficulties, and co-morbid psychiatric conditions.
Current medication treatment is often either ineffective or poorly tolerated due to side effects.
Sativex® is well tolerated and should be considered in patients where first-line treatments have failed.
Treatment options may be limited by the high cost of this proprietary cannabinoid preparation.
There is a need for further research, with a larger cohort of patients, to substantiate our findings and assess longer-term outcomes.
Footnotes
Disclosure
The authors report no conflict of interest. The authors alone are responsible for the content and writing of the paper.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.