
Abstract
Objectives:
Self-harm is common in New Zealand (NZ) young people and can have short-term and long-term consequences, including suicide. This study was undertaken to examine the extent to which evidence-based approaches for addressing self-harm are offered by Infant, Child and Adolescent Mental Health Services (ICAMHS).
Methods:
A national survey of ICAMHS practitioners working with young people who self-harm was undertaken between May and July 2016.
Results:
Responses from 23 out of 30 ICAMHS confirmed self-harm was a familiar presentation and most commonly associated with diagnoses of depression, anxiety and borderline personality disorder. Cognitive behavioural therapy (47.1%, n = 8), dialectical behaviour therapy (47.1%, n = 8) and acceptance and commitment therapy (5.9%, n = 1) were the treatments of choice, but variably delivered. There were significant training gaps for all types of therapy.
Conclusions:
Although it is reassuring that many ICAMHS are using evidence-based approaches to address self-harm in young people, there is concerning variability in the way these therapies are delivered. Improvement in training in key modalities, further research into therapist performance and continuous evaluation of workforce development are needed to maximise the effectiveness of proven interventions and provide NZ young people with the state-of-the-art service they deserve.
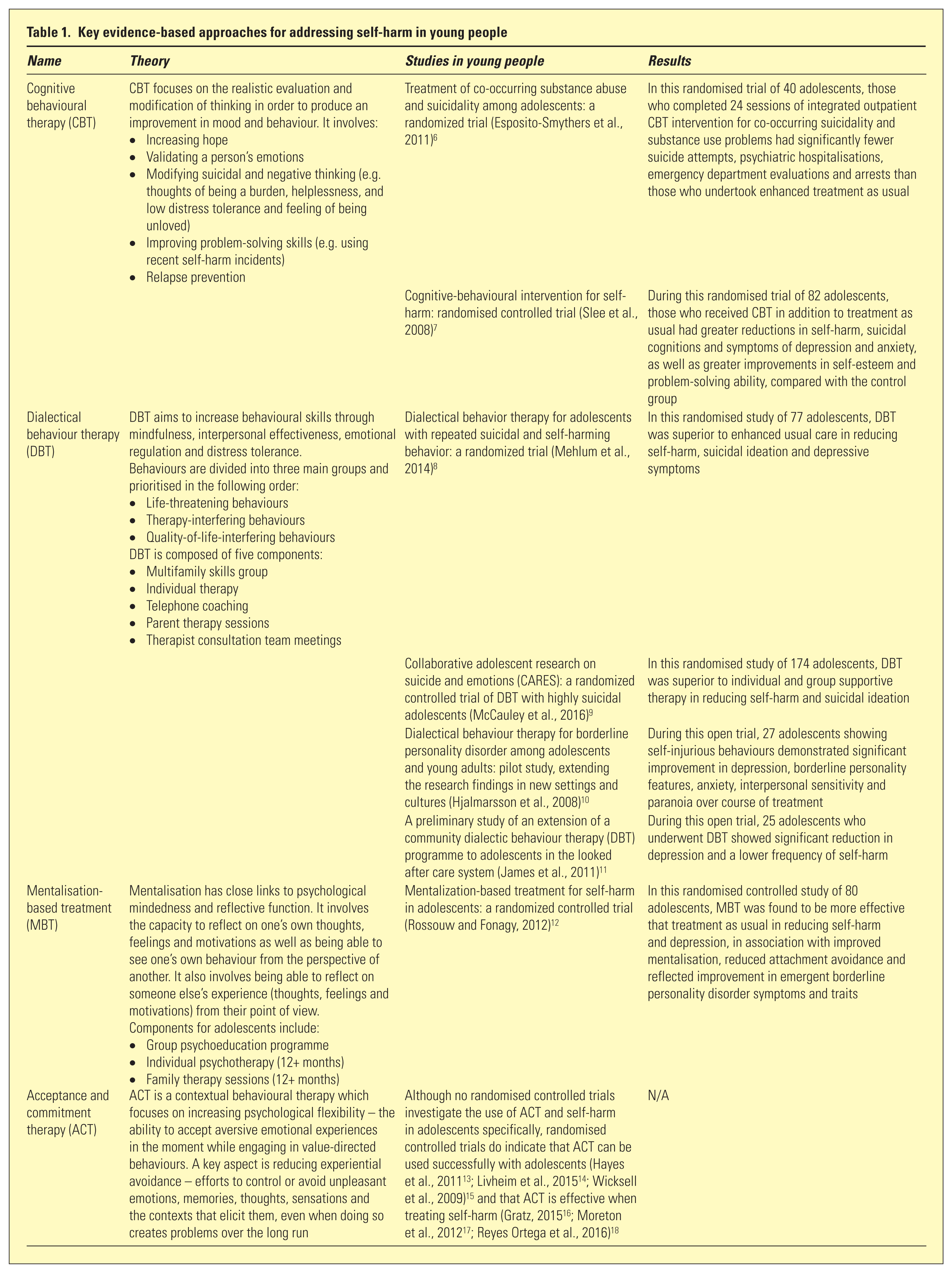
Self-harm, the intentional self-injury or self-poisoning, irrespective of the extent of suicidal intent, 1 is an increasingly significant health issue for New Zealand (NZ) young people, affecting around 24% of high school students (17.9% of males, 29.1% of females aged 13–19 years). 2 Its consequences include hospitalisation (80.8 per 100,000 males, 212.0 per 100,000 females aged 15–19 years), 3 depression and suicide. The NZ youth suicide rate remains one of the highest among OECD (Organisation for Economic Co-operation and Development) countries (19.3 per 100,000 young people and 36.4 per 100,000 Maori young people). 4 A number of evidence-based interventions, including cognitive behavioural therapy (CBT), dialectical behaviour therapy (DBT), mentalisation-based therapy (MBT), exist for addressing self-harm within specialist mental health settings (Table 1). 5 However, most research on these approaches has been conducted with adult populations in other countries. Training in these interventions is usually accessed via overseas providers in keeping with longstanding deficits of local opportunity. 19 Given the extent of self-harm in NZ young people and the significance of its relationship with youth suicide, it is important for specialist mental health services to offer high-quality evidence-based interventions to those who present for treatment. This study was undertaken to identify i) which, if any, evidence-based interventions for self-harm are currently being offered by NZ Infant, Child and Adolescent Mental Health Services (ICAMHS); ii) how closely delivery of these interventions is related to recommended practice by the developers of these interventions; and iii) what gaps exist for future training and workforce development.
Key evidence-based approaches for addressing self-harm in young people
Materials and methods
Practitioners from all 30 NZ community and inpatient ICAMHS working with young people who self-harm were invited to participate in an electronic survey between May and July 2016. As the study was considered ‘low-risk’ by NZ Health and Disability Ethics Committee standards, formal ethics approval was not required. To preserve confidentiality, demographic information was limited to participants’ role and District Health Board. Quantitative responses were analysed using statistical software in Microsoft Excel. Qualitative responses were categorised using content analysis. 20 Questions regarding approaches to the management of self-harm were based around a clinical scenario involving a 15-year-old high school student who presents to the emergency department for the third time in a year following an episode of self-harm (cutting) in the context of an argument with her boyfriend. Possible options for treatment included CBT, DBT, MBT, acceptance and commitment therapy (ACT), transference-focused therapy (TFT), the Conversational Model for Borderline Personality Disorder (CMBPD), the Common Factors Model (CFM), general psychiatric management (GPM) and others. Full details of the questionnaire are available by contacting the lead author.
Results
Participants
Responses were received from 20 out of 30 ICAMHS, two adolescent inpatient services and one youth alcohol and drug service from the Northern (n = 5), Midland (n = 5), Central (n = 7) and Southern (n = 7) regions. Participants included service managers (n = 4), team leaders (n = 5), clinical nurse specialists (n = 4), psychiatrists (n = 3) or did not specify their profession or role (n = 6). Services provided for young people who self-harm are outlined in Table 2. Most participants said their services would offer CBT (47.1%, n = 8), DBT (47.1%, n = 8) or ACT (5.9%, n = 1), or a range of secondary approaches to the young person in the described clinical scenario (Table 2). None said they would primarily employ MBT, TFT, CMBPD, CFM, GPM or pharmacotherapy to address self-harm or associated diagnoses. Most CBT strategies apart from homework using thought records and recommended activities were variably employed, as outlined in Table 3. A similar phenomenon was apparent with the practice of DBT. Although individual and family sessions were usually offered, out-of-hours support was usually delegated to crisis teams. Reasons provided for amendments to the full DBT programme included not having sufficient staff numbers and not having proper training to correctly implement treatment.
Services for young people who self-harm
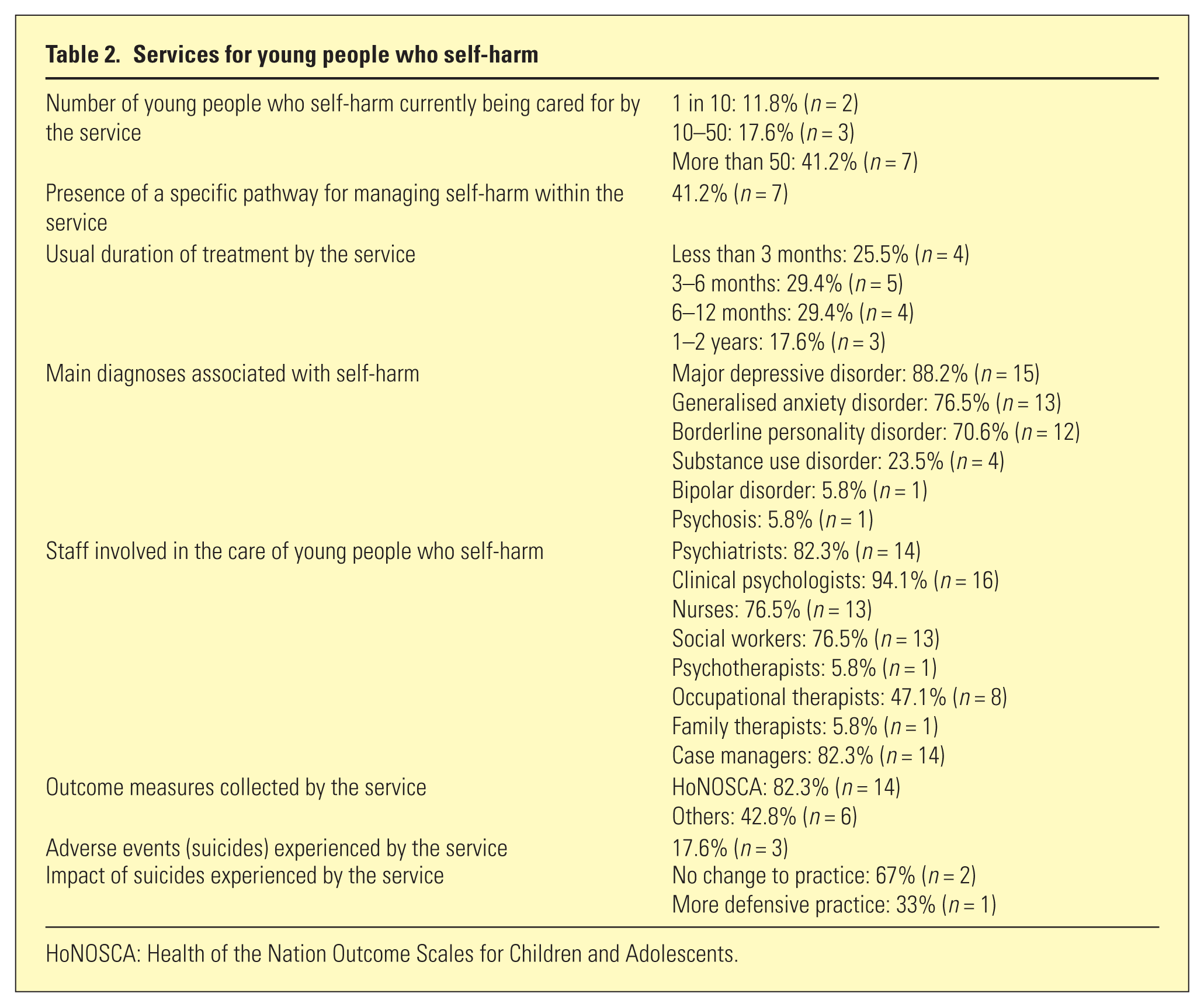
HoNOSCA: Health of the Nation Outcome Scales for Children and Adolescents.
Reported frequency of use of evidence-based interventions and their components
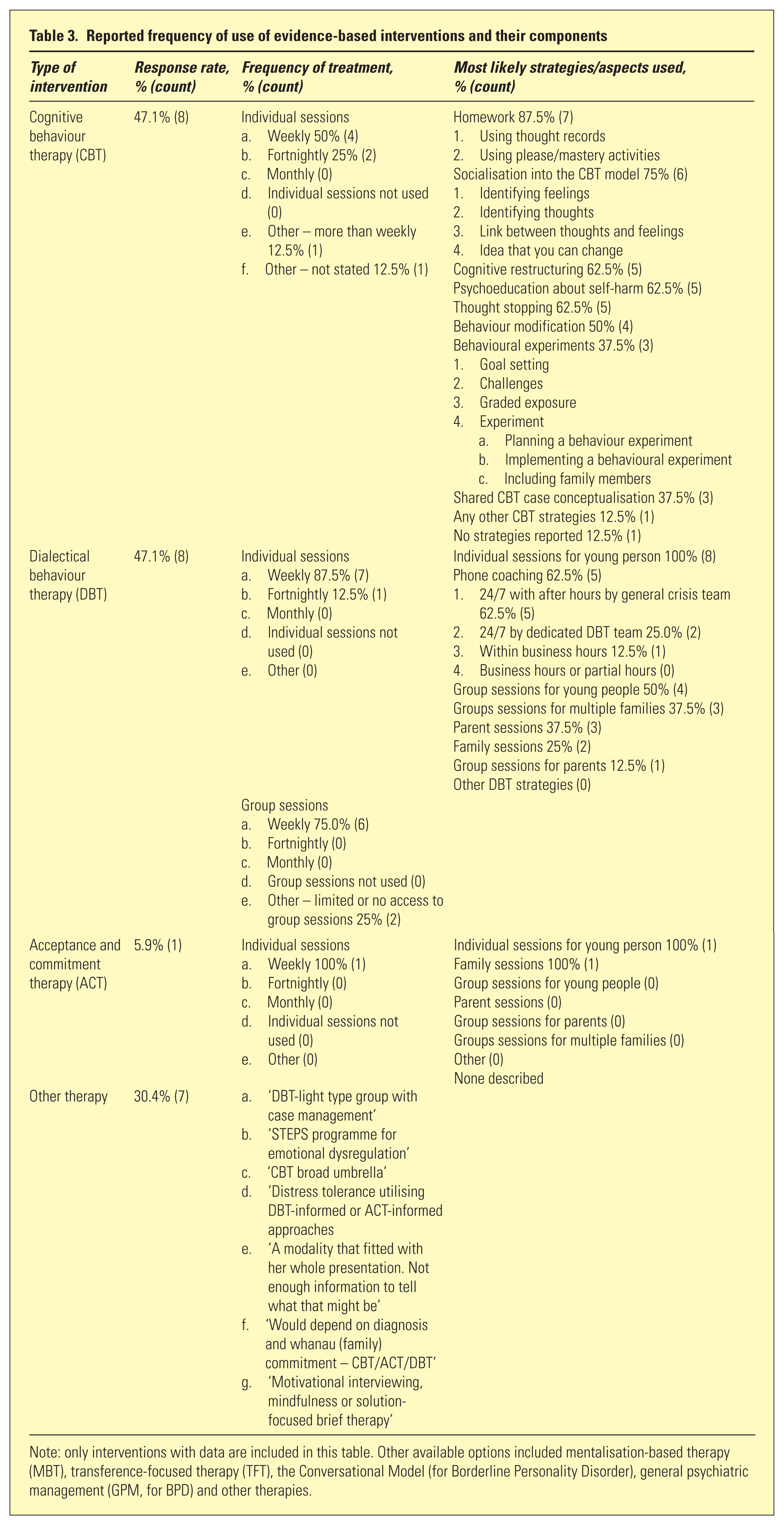
Note: only interventions with data are included in this table. Other available options included mentalisation-based therapy (MBT), transference-focused therapy (TFT), the Conversational Model (for Borderline Personality Disorder), general psychiatric management (GPM, for BPD) and other therapies.
Training and supervision for health professionals
Of respondents who said their service would offer CBT, adequate training and supervision was reportedly available to all staff in 12.5% (n = 1) services, to 25–50% of staff in 12.5% (n = 1) services and to less than 25% of staff in 75% (n = 6) services. The single respondent who said their service would offer ACT reported that less than 25% of their staff were well trained in the modality. None of the respondents who said their service would offer DBT or other interventions commented on the ease of access to training or supervision. However, individual open responses to the issue of training included requests for ‘more DBT training’, ‘skill development for inpatient staff to support community approaches’, eye movement desensitization and reprocessing to address issues underlying or associated with self-harm’ and the blanket statement that ‘any or all (training) would be welcome’.
Discussion
To our knowledge, this is the first study investigating the management of self-harm in young people by NZ specialist mental health services and it provides guidance for improving services toward this group. Concordant with community-based reports of its incidence, 2 self-harm is a familiar presentation to ICAMHS, most often associated with diagnoses of major depressive disorder, generalised anxiety disorder and borderline personality disorder. CBT, DBT and, to a lesser extent, ACT are the most commonly offered modalities for addressing self-harm within these services. Although MBT is yet to be offered as a therapeutic option, current clinical practice is broadly in line with the available body of research. Four systematic reviews21–24 and one narrative review 25 of interventions for children and young people with self-harm have only identified three interventions, namely self-harm-focused CBT, DBT and MBT, as capable of significantly reducing recurrent suicidality or self-harm. Although it is reassuring that young people have access to multi-disciplinary care, the fidelity with which ‘real-world’ treatment aligns with research-tested models shows concerning variation. One could argue that therapeutic interventions should be tailored to fit the needs of individuals, rather than delivered using a ‘cookie-cutter’ approach. However, when given the same clinical scenario, survey respondents reported disparate methods of providing nominally identical interventions, primarily for reasons of practicality and training, rather than conscious clinical preference. The most commonly reported duration of treatment of less than a year is in keeping with national trends toward briefer interventions within specialist mental health services. However, the effectiveness of currently used interventions remains unknown as the only consistently undertaken outcome measure in ICAMHS is the HoNOSCA (Health of the Nation Outcome Scales for Children and Adolescents), a global rating that neither measures self-harm nor associated psychopathology. The RANZCP (Royal Australian and New Zealand College of Psychiatrists) guideline on deliberate self-harm describes five factors that should be included when designing interventions to prevent the repetition of self-harm – motivation to change, maintenance of sobriety, familial or non-familial support, promotion of positive affect and healthy sleep – and recommends timeliness of intervention as people are most likely to repeat self-harm within four weeks of an index event. 5 Although these recommendations have yet to be formally evaluated, they should also be borne in mind when treating young people who self-harm.
Admittedly, there is more to providing high-quality evidence-based interventions than offering all components of proven therapies. International studies have shown that clinicians lack adequate training and supervision in managing self-harm,26,27 that outcome variability is strongly linked to therapist qualities or performance rather than to treatment itself, and that therapists are often inaccurate in estimating their own performance and clinical outcomes. 28 Fortunately, it has also been shown that with adequate training and support, therapist performance can be improved and maintained at a good standard, and a subset of therapists can achieve superior performance. 15 The findings of our study support the need for further workforce development for practitioners working with young people who self-harm. Improved access to local training and supervision, particularly for those who do not receive Continuous Medical Education funding, is also necessary to increase skills and confidence. Finally, national or regional ‘hub and spoke’ networks should be used to increase fidelity of practice for key interventions toward desired standards.
Strengths of this study include the geographic spread of respondents and the depth of questioning regarding available interventions. Limitations include not all ICAMHS participating and incomplete responses, particularly regarding training issues. Evaluation of formal outcome measures is needed to demonstrate interventions are associated with reduction or prevention of further self-harm. Randomised controlled trials of existing interventions within a local context are also necessary to demonstrate their value and acceptability, particularly to Māori and Pacific Island young people. Locally developed interventions also need to be examined for comparative efficacy. Finally, research into therapist performance and continuous evaluation of workforce development activities are needed to maximise the effectiveness of proven interventions. For now, there is room for improving the quality of existing evidence-based interventions and implementing newer interventions such as MBT for services to stop cutting corners and provide young people who self-harm with the state-of-the art service they deserve.