
Abstract
Objective:
The objective of this study is to determine if pattern-based formulation (PBF) can accurately contribute to case formulation.
Conclusions:
The application of three PBFs accurately contributed to the development of this patient’s case formulation. The case formulation demonstrated here, and the patterns introduced in this paper, will serve as educational materials for teaching psychiatric case formulation.
Keywords
In an effort to facilitate teaching psychiatric case formulation and clinical reasoning, a methodology known as pattern-based formulation (PBF) has been introduced that works in tandem with a systematic approach to clinical reasoning.1,2 As an expansion of this work, we intend to build a catalogue of patterns that can serve as building blocks in constructing case formulations. A few patterns have already been introduced by demonstrating their use in constructing case formulations.3,4 In this paper we use the clinical case of a patient who developed interpersonal sensitivity as a result of experiencing ongoing mistreatment in their workplace, which finally resulted in major depression and cardiovascular disease. We have introduced four patterns in formulating this case, and have used cognitive schema theory 5 and the current literature on the association between chronic stress, depression and cardiovascular disease 6 in deriving these patterns.
Clinical case
The patient was a 50-year-old man presenting with major depression with comorbid anxiety in the context of workplace bullying and mistreatment. He did not have a previous psychiatric history, and had been functioning well both at work and in the community as an active member of a local sports club.
The patient first suffered a knee injury which required surgical interventions, and resulted in lack of mobility and pain for a period of several months. Consequently, he started experiencing an impairment in work performance, and began to receive harsh treatment from his supervisors at work. As the situation continued the patient increasingly came to believe he was being judged by his work colleagues (e.g. ‘I feel like people think I am a bludger’) and mistreated. He also started losing his self-confidence and feeling inadequate because of his physical impairment and the experience of mistreatment. The patient experienced an increased level of psychological distress at work for a period of 18 months, and the situation became progressively worse. Eventually, he was sent on medical leave because of the decline of his mental as well as physical health. While the patient had recently been diagnosed with hyperlipidaemia, he gained excessive weight after he started neglecting his diet and giving up his routine physical exercise. The patient developed hypertension and ischaemic heart disease during this time period, and also experienced progressively worsening symptoms of depression and anxiety including insomnia, nightmares, depressed mood, loss of concentration and anhedonia.
The patient’s depression improved after commencing antidepressant treatment and engaging in therapy that also focused on treating his interpersonal sensitivity.
Nonetheless, the patient continued to have a fragile mental state with frequent episodes of severe anxiety symptoms including shortness of breath, palpitations, tremors and sweats that were induced by interpersonal disputes. For example, he once became offended and felt he was being ignored while waiting to be served at a counter when there was a minor delay. He was also easily offended. After having a minor disagreement with the manager of his local sports club, he quit his voluntary work. The patient often experienced recurrences of his depressive and anxiety symptoms that usually lasted about 2–3 days following interpersonal disputes.
Psychiatric case formulation
Psychiatric formulation of the above-stated clinical case attempts to answer the question: why did this patient develop major depression and cardiovascular complications in the context of his perceived workplace mistreatment, and end up having interpersonal difficulties and episodes of exacerbated symptoms as a result?
In order to answer this question, we have used PBF and produced four explanatory models (i.e. patterns) that are described in the following sections. We have used the diagram notation given in Figure 1, in which the arrows indicate the hypothesised direction of association or causation.
Diagram notation used in illustrating patterns.
Development of interpersonal sensitivity and fragile mental state with episodes of exacerbations following interpersonal triggers
The patient’s interpersonal sensitivity can be explained from the perspective of cognitive schema theory using the following maladaptive schemas 5 : mistrust/abuse (i.e. feeling of being abused or humiliated by others); and defectiveness/shame (i.e. feeling defective and invalid). It can be hypothesised that these maladaptive schemas were activated by the physical impairment from the knee injury and the resulting criticism and negative evaluation by others because of the patient’s impaired work performance. The persistent over-activation of these schemas can be thought to have caused the interpersonal sensitivity as described in Figure 2. On the other hand, the ongoing interpersonal difficulties can be conceptualised in relation to the cognitive distortions of his perceived mistreatment by others, resulting in the perpetuation of these schemas, 5 as described in Figure 3.
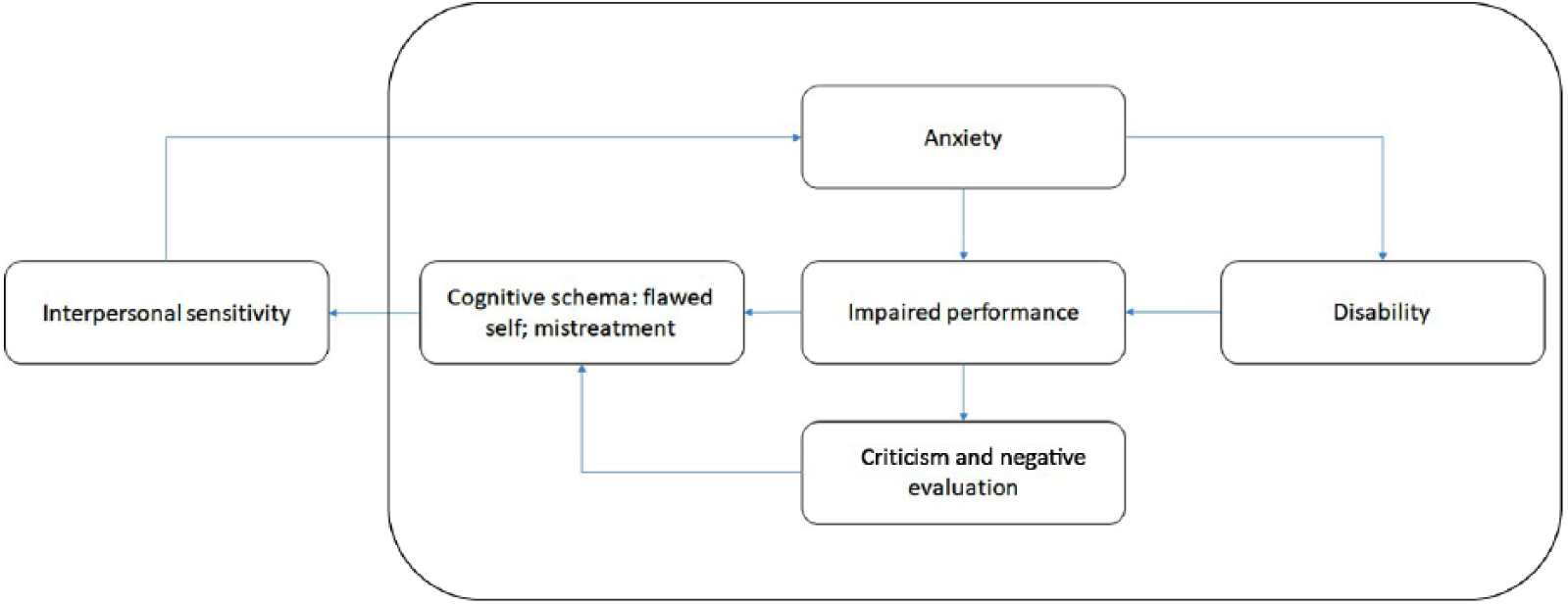
Formulation model for the development of interpersonal sensitivity.
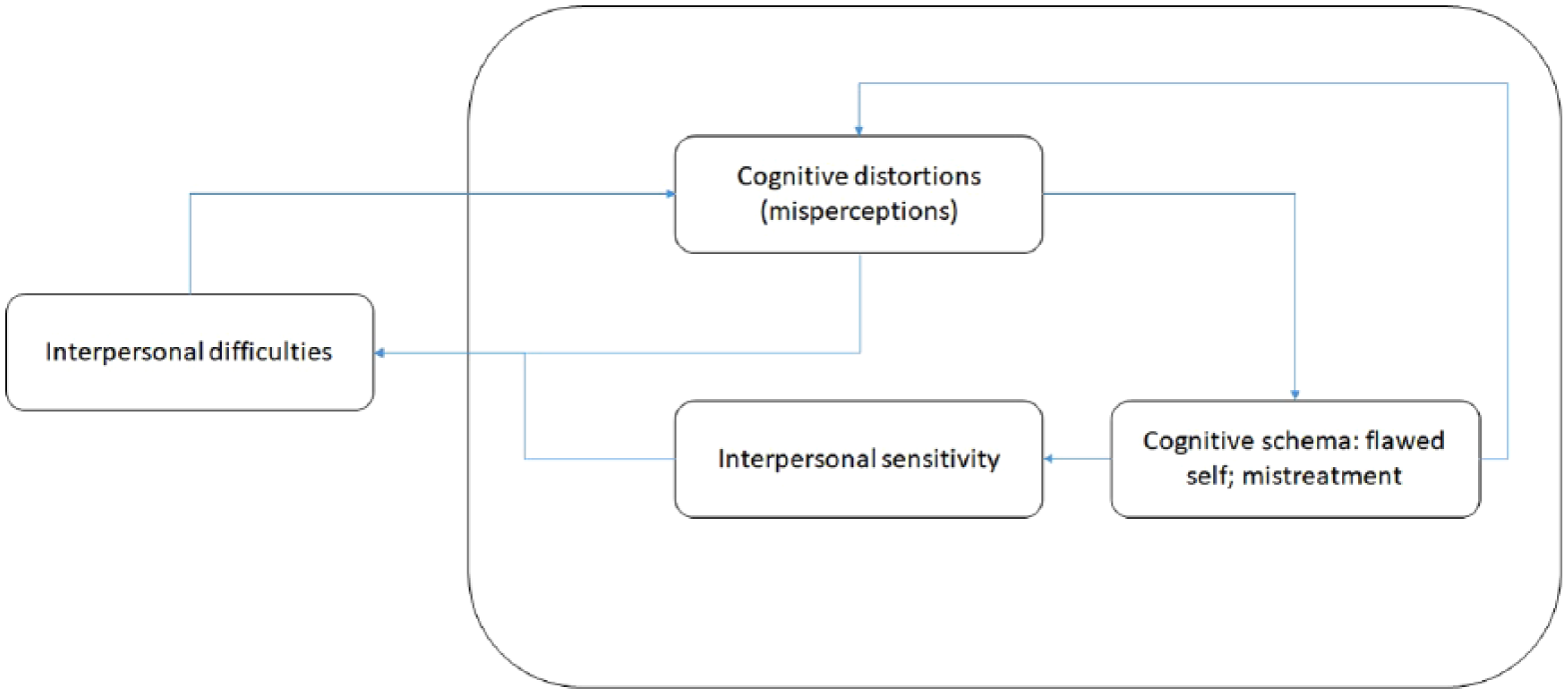
Formulation model for the interpersonal difficulties caused by interpersonal sensitivity, cognitive distortions and perpetuation of cognitive schemas.
Development of major depression and cardiovascular complications in the context of mistreatment in the workplace
As described above, the cognitive schemas of flawed self and mistreatment, and the resulting interpersonal sensitivity, created an ongoing stressful situation at work because of the patients’ almost daily perceptions of being mistreated and judged. Chronic stress is known to cause a common pathway that can result in these two conditions through the following four mechanisms 6 : (a) the hypothalamic–pituitary–adrenal (HPA)-axis dysregulation; (b) autonomic dysregulation; (c) immune inflammatory dysregulation; and (d) metabolic dysregulation via physical inactivity and unhealthy eating. Based on these findings, the simultaneous development of depression and cardiovascular disease can be conceptualised using the two biological models that are described in Figures 4 and 5.
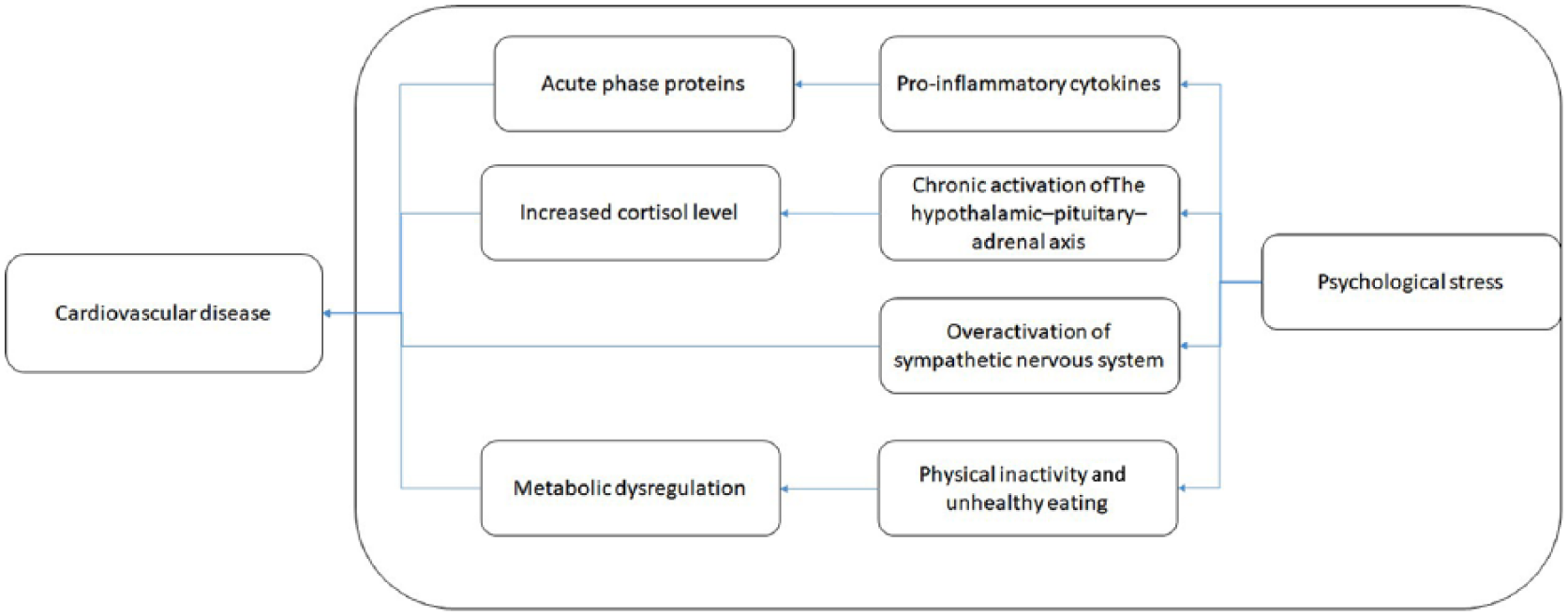
Formulation model for the development of cardiovascular disease in the context of chronic stress.
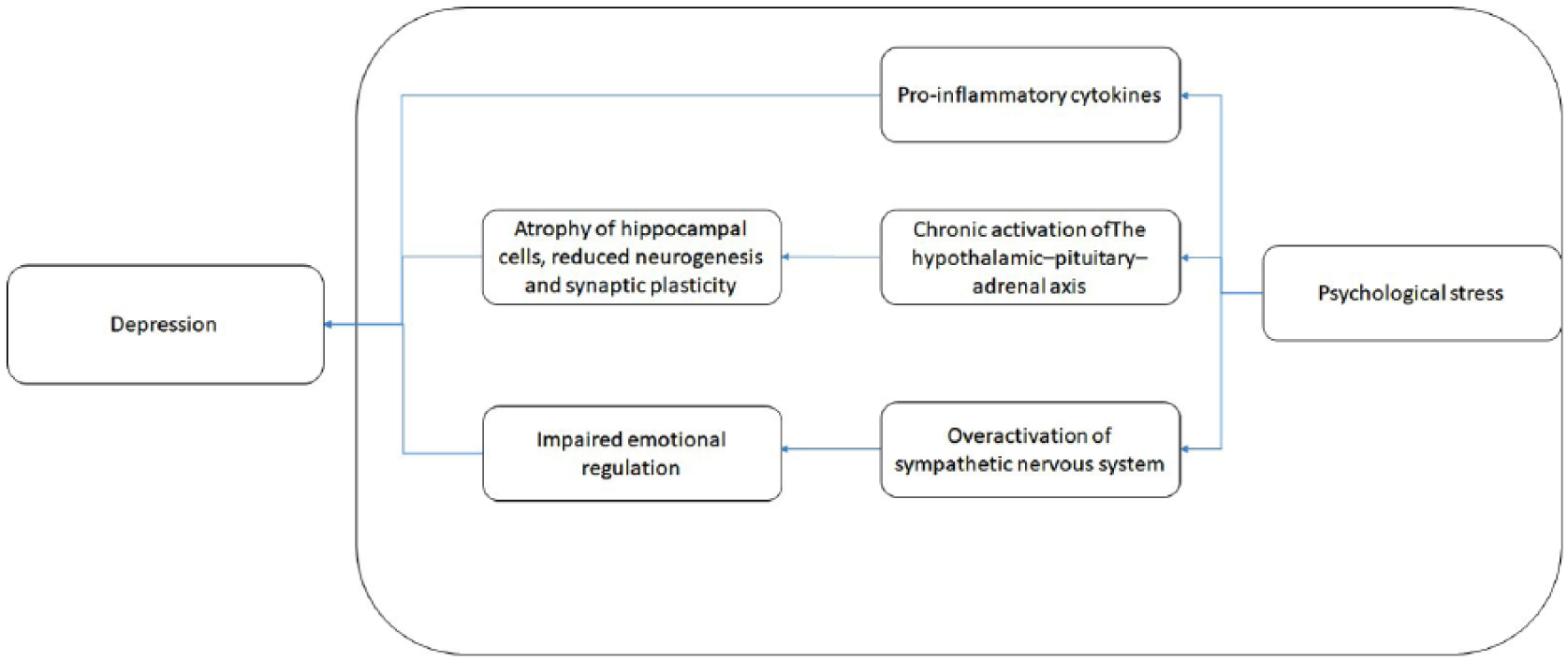
Formulation model for the development of depression in the context of chronic stress.
In relation to the HPA-axis dysregulation, chronic stress is known to cause increased cortisol levels via the corticotropin-releasing hormone, resulting in alterations in the mineral and glucocorticoid receptors, decreased synaptic plasticity and alterations in monoaminergic signalling, which is implicated in depression. 7 Increased cortisol is also known to be associated with increased cardiovascular risk through hypertension and metabolic syndrome. 8
From the perspective of autonomic dysregulation, depression is hypothesised to be a state of the over-activation of a sympathetic nervous system compared to parasympathetic activation, resulting in an increased risk for cardiovascular events. 9 The development of hypertension in the context of chronic psychological stress can be understood in relation to the activation of the renal sympathetic nervous system. 10
In relation to the immune inflammatory dysregulation, the etiological process of depression as a pathway from psychological stress via inflammation has been well described. 11 The activation of the innate immune system via stress is known to induce an array of molecules, including pro-inflammatory cytokines, which in turn induce the synthesis of acute-phase proteins. While this inflammatory process has been linked to the symptoms of depression 12 it has also been implicated in coronary heart disease, particularly in atherosclerosis. 13
Even though the development of depression and of cardiovascular disease in the context of chronic stress have been presented as two separate models for simplicity, it is important to acknowledge the possible bidirectional links between these two conditions. According to a large meta-analysis, 14 depression was found to be associated with future coronary heart disease by a pooled relative risk of 1.81.
Discussion
While a clinical case with obvious causal linkages and associated temporal sequences is chosen and presented in an orderly fashion in this paper for teaching purposes, we acknowledge that clinicians often encounter rather less orderly presentations in their routine clinical practice.
It is not uncommon in clinical practice to encounter patients with depression and cardiovascular disease that they developed in the context of stressful circumstances such as workplace injury and bullying, as demonstrated by the clinical case. Even though it is important to understand each patient as an individual in relation to his/her life circumstances, generalisation using patterns enhances our learning and clinical reasoning. Therefore, the patterns introduced in this paper can serve as a template for conceptualising similar presentations.
We acknowledge that more experienced clinicians may take a different perspective on the case presented in this paper, and construct different psychiatric case formulations (e.g. using attachment theory to explain the interpersonal difficulties). As described in our previous work on clinical reasoning and psychiatric case formulation, it is important for trainees to derive as many potential models as they can, as it enriches their clinical experience and learning. While it is also possible to integrate or merge different models as we have demonstrated previously, 4 their representation as a visual aid using the diagram notation can be flexible. The choice of final model/s needs to be guided by treatment interventions that are informed by the model/s and how they best fit with the clinical case.
The clinical case presented here is characterised by late-onset interpersonal sensitivity and the related affective instability (i.e. rapid changes from euthymic states to mixed states of anxiety, depressed mood and anger) resulting in a fragile mental state. Even though it is not considered as a personality disorder because of its non-pervasiveness, there is a resemblance to the interpersonal difficulties that are experienced by patients with borderline personality disorder (there were no fear of abandonment, which is a common theme underlying interpersonal difficulties in borderline personality disorder). Also, while the cognitive models in therapy often assume the presence of early childhood experiences that cause the formation of early schemas that become activated during later life, the patient did not have such vulnerability. Therefore, this clinical case also serves as a counterexample of someone who has developed the same pathway of psychopathology without a pre-existing early schema.
Conclusion
Using the PBF, this paper has demonstrated the psychiatric case formulation of a patient who developed interpersonal sensitivity, major depression and comorbid cardiovascular disease in the context of stressful circumstances related to their mistreatment in the workplace. It is expected that the four patterns introduced in this paper can be used by psychiatric trainees to construct case formulations for patients presenting with the following issues: (a) depression and cardiovascular disease in the context of increased psychological stress; and (b) interpersonal difficulties related to interpersonal sensitivity that have resulted from the experience of mistreatment. The addition of these four patterns to the repository of existing patterns has expanded the teaching material on case formulation. It is expected that trainees will be able to enhance their learning by familiarising themselves with these patterns and their use.