
Abstract
Objectives:
This clinical update review focuses on the management of cognition and the neuropsychiatric features of Alzheimer’s disease (AD) and highlights current issues regarding pharmacological and non-pharmacological treatment, putative therapeutics and recent relevant research findings in this area.
Conclusions:
AD is a neurodegenerative progressive condition characterised by cognitive impairment and functional decline. Most people with AD will demonstrate neuropsychiatric features, better known as behavioural and psychological symptoms of dementia (BPSD). Early recognition and treatment of BPSD are essential, as these cause considerable distress and carer burden. While there are many disease-modifying therapies for the cognitive symptoms still in the research stage, only symptomatic treatments are currently available for these and the BPSD.
Keywords
‘Memories were waiting at the edges of things, beckoning to me.’
The management of Alzheimer’s disease (AD) is complex and requires a multidisciplinary approach, involving a range of clinicians, including a medical specialist (neurologist, psychiatrist, geriatrician), general practitioner (GP), nursing and allied health professionals (social worker, occupational therapist, psychologist). The major management issues to consider are listed in Table 1. This paper will focus on the management of AD and neuropsychiatric symptoms (or behavioural and psychological symptoms of dementia, BPSD). Family and carers, and the person with AD have essential roles in collaborating on the management of these symptoms.
Major management issues to consider
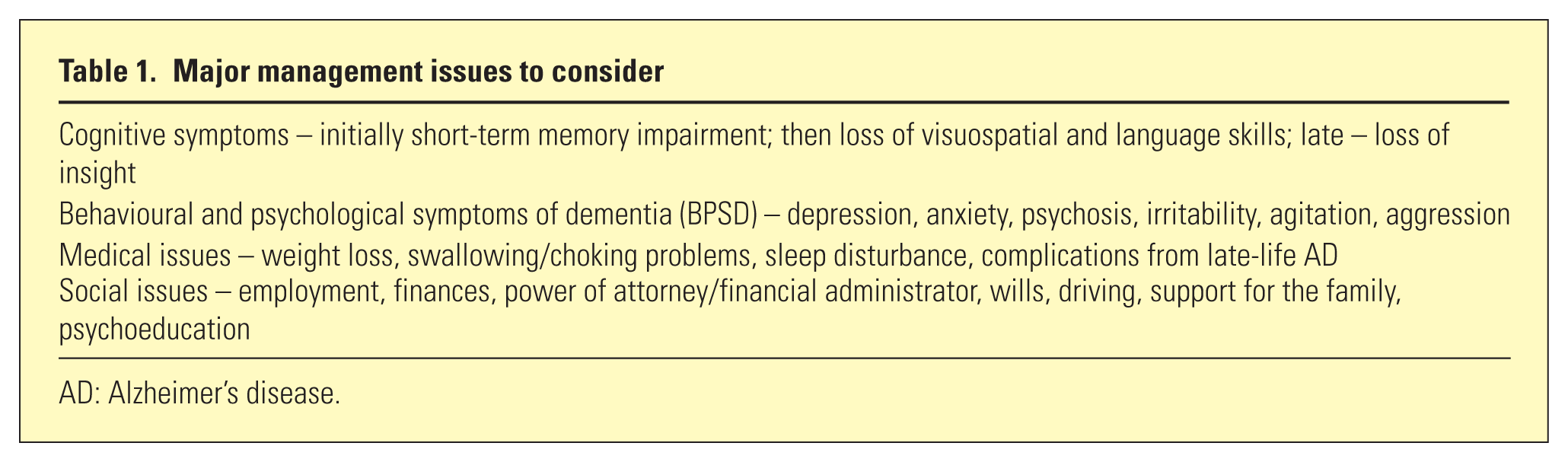
AD: Alzheimer’s disease.
Challenges
The major challenge is the absence of disease-modifying treatments for AD. As Eratne et al. outlined in paper 1, the pathophysiology of AD remains unclear. Deposition of amyloid plaques (composed of amyloid beta, Aβ), neurofibrillary tangles (composed of tau), iron, vascular contribution, etc., may all be involved. The presence of amyloid plaques at least 15–20 years prior to initial clinical manifestations suggests that, when available, combinations of disease-modifying therapies may have to be commenced at the very early stages of the disease to target insidious pathophysiological processes.
Pharmacological treatments for cognitive symptoms of AD
AD is the most common type of dementia and currently the only available treatments target symptoms of AD, such as slowing cognitive decline, and/or treat neuropsychiatric manifestations, while other treatments may be needed for other types of dementia. (see section on BPSD below). The cholinesterase inhibitors (donepezil, galantamine and rivstagimine) and the N-methyl-D-aspartate receptor antagonist, memantine, are licensed for treating AD and produce modest improvements in cognition and neuropsychiatric symptoms for some patients. The putative mechanism of action is through increasing cholinergic signalling and reducing excessive excitatory glutamatergic activity (cholinergic inhibitors and memantine, respectively). In New Zealand, memantine is not currently not subsidised, which may limit its use). In 2008, a transdermal patch for rivastigmine became available and in 2010, a slow-release version of donepezil became available (23 mg). In some parts of Asia, an orally disintegrating formulation of donepezil is also available. In general, cholinesterase inhibitors are introduced once mild AD is diagnosed, while memantine is introduced as an adjunctive treatment as persons with AD develop moderate disease manifesting dysfunction in activities of daily living (ADLs). Unfortunately, both cholinesterase inhibitors and memantine have not been shown to be effective in mild cognitive impairment which may precede AD.
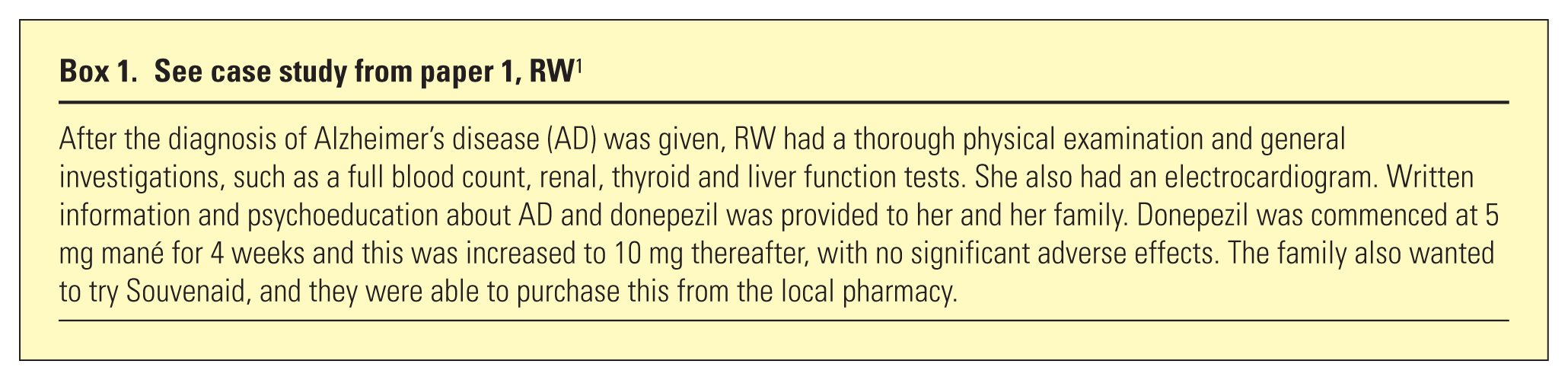
Side-effects are generally mild and tolerable, and include gastrointestinal side effects such as diarrhoea and nausea. Vivid dreams are an occasional complaint. Caution is advised in people who have obstructive respiratory (such as asthma or obstructive pulmonary disease) and cardiovascular conditions (an electrocardiogram is recommended prior to commencement of these medications). Substituting one cholinesterase inhibitor for an alternative may assist, or using the rivastigmine patch may ameliorate these side-effects (Box 1).
See case study from paper 1, RW 1
There are many nutraceuticals for which there is limited evidence of benefit, such as fish oil and gingko biloba. There is limited evidence on the benefits of Souvenaid, a dietary drink containing fatty acids, vitamins and other nutrients.
There have been over 200 other drugs which have reached phase 2 development between 1984 to now, but none have been approved for routine use. Passive vaccines containing monoclonal antibodies in prodromal AD have yielded promising results. Table 2 shows a selection of current trials (please refer to the recommended reading list in the online appendix for further information on this topic).
Selected medications currently being trialled – as of October 2017

Aβ: amyloid beta; APP: amyloid precursor protein; APOE4: apolipoprotein E4; BACE: β-secretase; CSF: cerebrospinal fluid; PET: positron emission tomography.
Behavioural and psychological symptoms of dementia (BPSD)
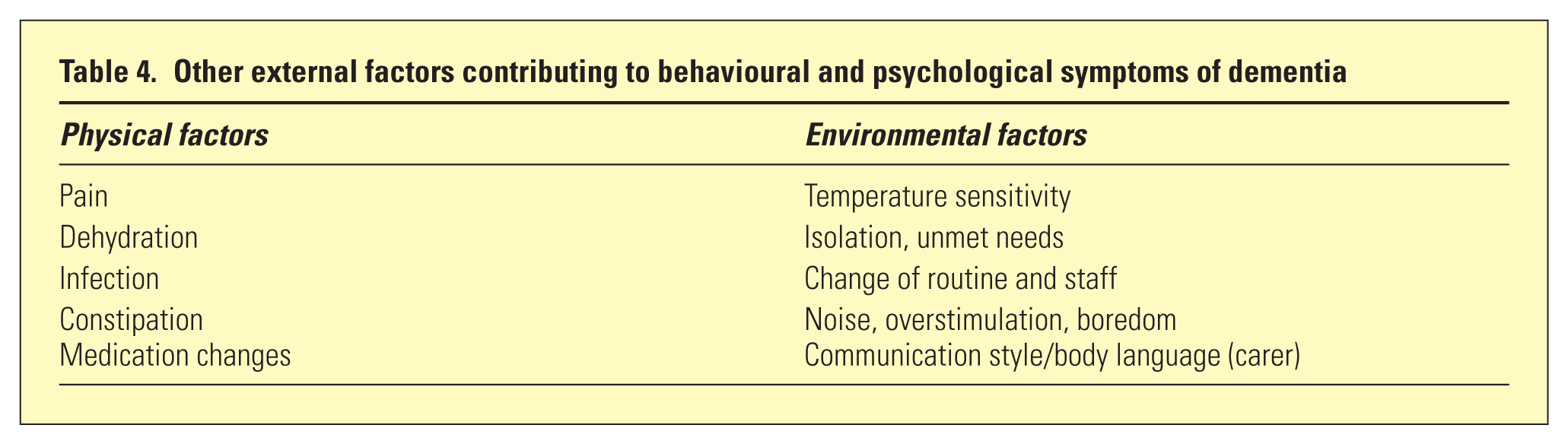
The behavioural and psychological symptoms of dementia occur in most people who have AD and especially in those who are living in residential care (see Table 3). BPSDs are major precipitants of a person entering residential care and can occur at any stage of dementia, though delusions, hallucinations, anxiety, irritability and disinhibition are reported with similar severity at all stages. A general medical assessment to ensure there are no concurrent medical (i.e. delirium), physical or environmental (Table 4) factors is important. The aetiology of BPSD is not well understood but is likely multifactorial.
Types of behavioural and psychological symptoms of dementia
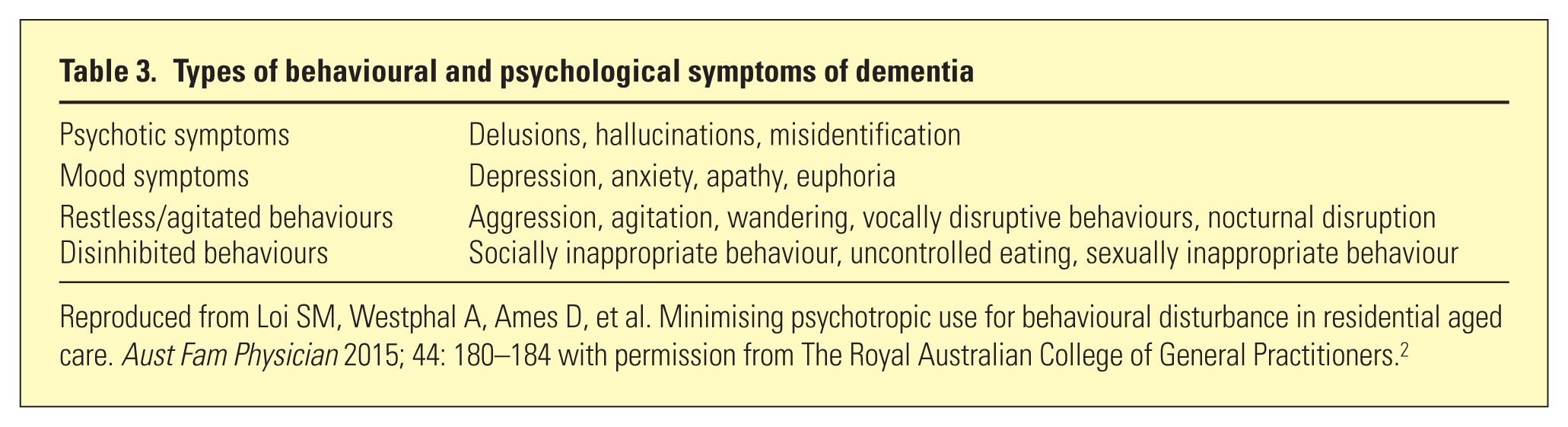
Reproduced from Loi SM, Westphal A, Ames D, et al. Minimising psychotropic use for behavioural disturbance in residential aged care. Aust Fam Physician 2015; 44: 180–184 with permission from The Royal Australian College of General Practitioners. 2
Other external factors contributing to behavioural and psychological symptoms of dementia
Assessment challenges for behavioural and psychological symptoms of dementia
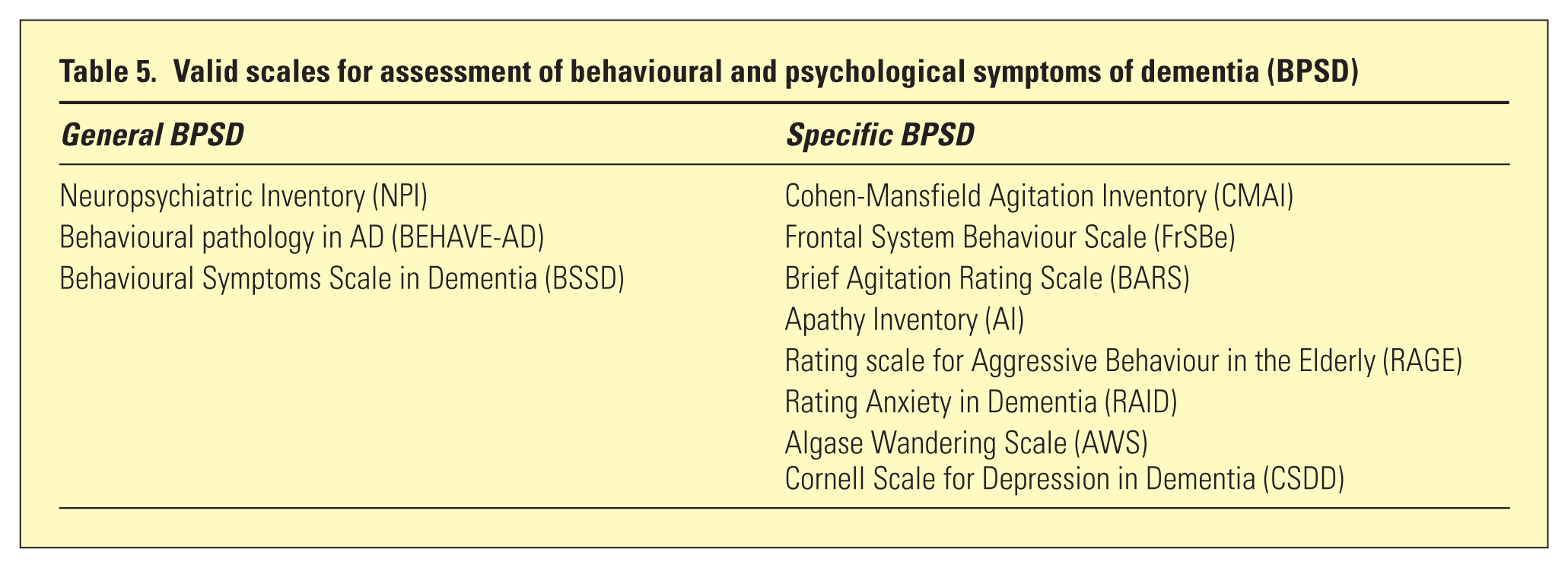
Comprehensive assessment is required, but this can be challenging as the person with AD may have difficulty communicating or co-operating. Table 5 shows a variety of scales available for assessing BPSD, which can be divided into general and specific measures and have a variety of advantages and disadvantages. Important assessment questions are displayed in Table 6.
Valid scales for assessment of behavioural and psychological symptoms of dementia (BPSD)
Assessment questions for behavioural and psychological symptoms of dementia
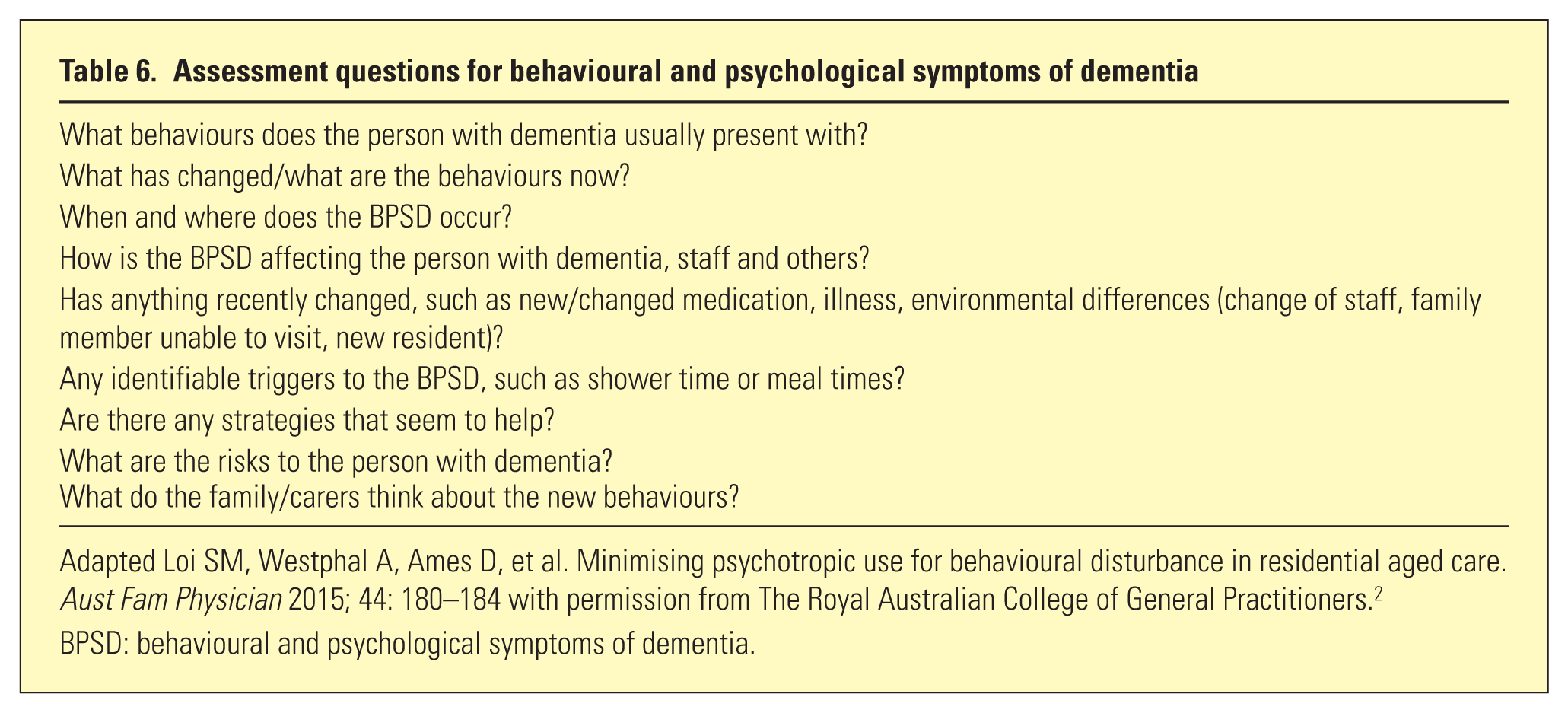
Adapted Loi SM, Westphal A, Ames D, et al. Minimising psychotropic use for behavioural disturbance in residential aged care. Aust Fam Physician 2015; 44: 180–184 with permission from The Royal Australian College of General Practitioners. 2
BPSD: behavioural and psychological symptoms of dementia.
As well as the validated scales, real-time assessment tools may also be useful in capturing this practical information. 3
Non-pharmacological management of behavioural and psychological symptoms of dementia
The limited evidence-base and concern about safety in psychotropic medication have led to recommendations that non-pharmacological strategies are first-line in BPSD, though both are often utilised together. There is a substantial literature on various non-pharmacological strategies, limited by small sample sizes, lack of blinding and randomised design. Five recent review papers informed Table 7 and are listed in the recommended readings (high-level 1, consistent evidence; low-level 5, inconsistent evidence). There is little evidence for specific treatments of certain BPSDs, such as wandering and vocalisation. In general, the best evidence-based approaches are individualised and person-centred. It is important to note that such non-pharmacological strategies may be more resource intensive.
Non-pharmacological strategies in behavioural and psychological symptoms of dementia
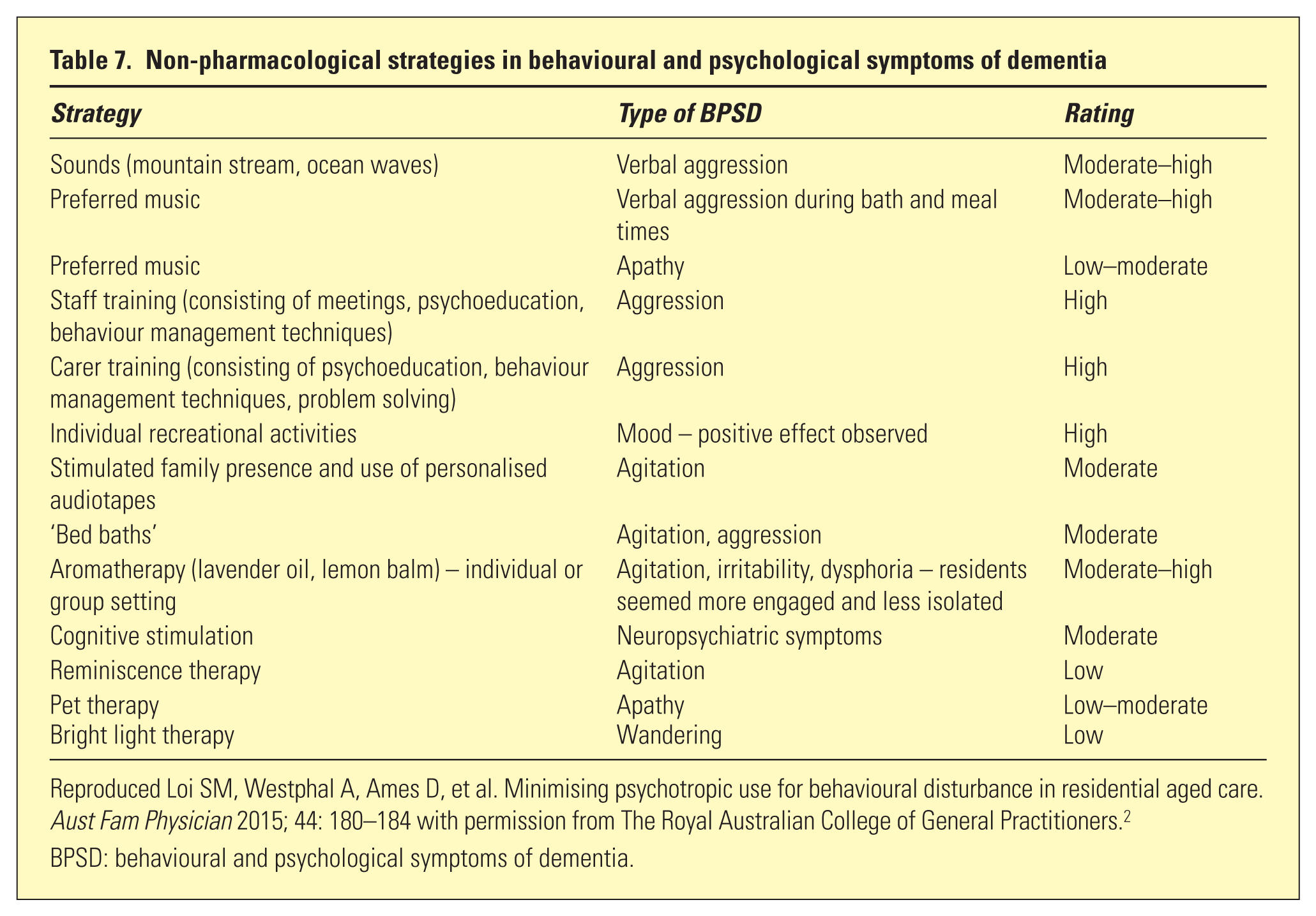
Reproduced Loi SM, Westphal A, Ames D, et al. Minimising psychotropic use for behavioural disturbance in residential aged care. Aust Fam Physician 2015; 44: 180–184 with permission from The Royal Australian College of General Practitioners. 2
BPSD: behavioural and psychological symptoms of dementia.
Carers play an important role in the management of BPSD and are often unaware of their own role in modifying BPSD. Table 8 outlines a variety of factors for carers and staff to consider when implementing a behavioural management plan.
Factors to consider when managing behavioural and psychological symptoms of dementia
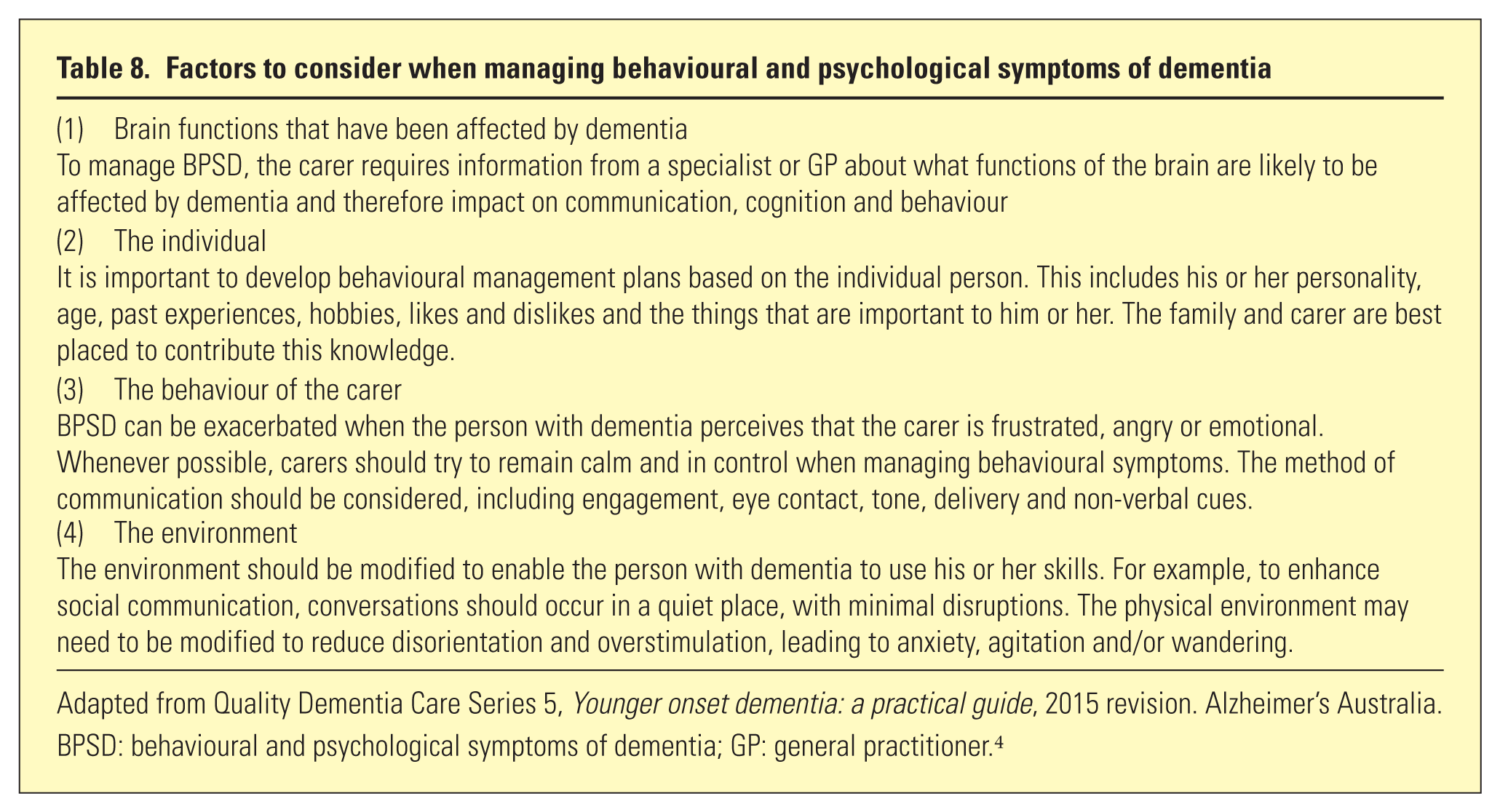
Adapted from Quality Dementia Care Series 5, Younger onset dementia: a practical guide, 2015 revision. Alzheimer’s Australia.
BPSD: behavioural and psychological symptoms of dementia; GP: general practitioner. 4
Pharmacological management of BPSD
Due to the risks of adverse effects and interactions with other medications, pharmacological strategies are second-line. In general, medications should be used to manage specific BPSD clinical syndromes. Antidepressants and antipsychotics may be beneficial in treating depressive and psychotic symptoms, respectively (but see Banerjee et al. 5 ). General treatment principles for older adults are important: start at a low dose with gradual increases, regular reviews, and consideration of other comorbid medical conditions and medications. Discussion with the patient, families and carers about the need for and potential side effects of medication, and how to monitor for side effects is essential (Box 2).
Case study continued…
Risperidone is the only atypical antipsychotic subsidised and approved for use in Australia for BPSD and can improve psychosis, agitation and aggression. Table 9 lists examples of medications, their possible indications for specific symptoms and side-effects. BPSDs such as vocalisation, wandering, reverse sleep–wake cycle, and sexually inappropriate behaviours do not usually respond well to medications. Specialist clinicians such as psychiatrists may feel pressured by aged care facility staff, general practitioners and families, to prescribe ‘something’ for BPSD. Often, by the time a person with dementia is being reviewed by a specialist, the BPSD has not responded to non-pharmacological measures. It is still important that the specialist perform a thorough assessment as described earlier. Both atypical (e.g. risperidone, quetiapine, olanzapine) and typical antipsychotics (e.g. haloperidol) and/or benzodiazepines (e.g. diazepam, oxazepam) have been prescribed individually, and in combination by specialists to manage BPSD. However, there remains limited evidence supporting the use of antipsychotics in dementia with significant adverse effects such as stroke, prolonged QTc interval and exacerbation of existing cognitive impairment. The Royal Australian and New Zealand College of Psychiatrists have published a Professional Practice Guideline and have made recommendations. 6
Examples of pharmacological management
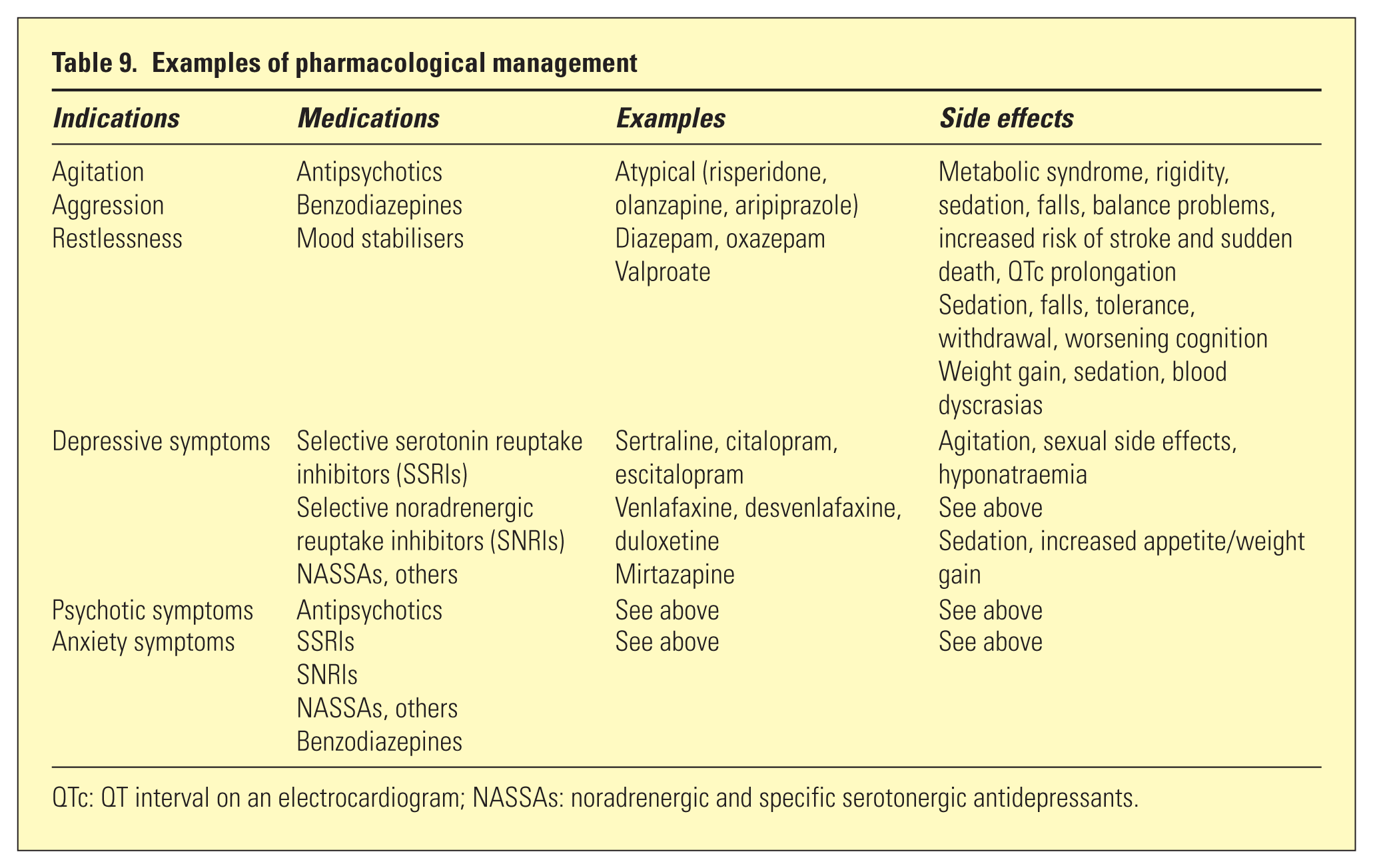
QTc: QT interval on an electrocardiogram; NASSAs: noradrenergic and specific serotonergic antidepressants.
Simple analgesia such as regular paracetamol has been reported to reduce BPSD in residents in nursing homes. 7 Donepezil and memantine may also improve BPSD. 8
Supporting carers
Caring for someone with dementia can be physically and emotionally demanding. Family members and carers need further education and support when undertaking the caring role. High levels of carer burden and ‘burnout’ lead to earlier residential placement for the person with dementia. Carers are at increased risk of anxiety, depression and physical ill health, due to the side effects of the caring role. It is important that GPs and/or the treating specialist engage with the carer and ensure their mental health, physical safety and wellbeing is being closely monitored. Family members and carers often report that they do not have the opportunity to openly discuss their concerns with the treating medical professional. It is vital that the doctor can talk to the carer, without the person with dementia in the consulting room. This ensures that the carer can confidentially disclose any personal safety concerns as a result of the BPSD and discuss their emotional and physical wellbeing. There are a variety of excellent educational and counselling programs and referral services available to support carers. Information regarding behavioural support services, respite and residential care can be accessed through a variety of national agencies (see Table 10 for recommended readings).
Discussion and conclusions
Pharmacological treatment for the cognitive symptoms of AD is based upon use of cholinesterase inhibitors and the N-methyl-D-aspartate antagonist, memantine. The majority of neuropsychiatric manifestations of AD, commonly grouped as BPSDs, are best addressed by personalised non-pharmacological psychological and behavioural approaches. In moderate-to-severe cases, especially where there is significant suffering for the patient and/or carer stress due to risk to others (e.g. aggression, psychosis), judicious pharmacological treatment may be considered. Families and carers play a vital role in supporting the person with dementia and require education, support and respite to assist them in their role.
Supplemental Material
APY766123_Appendix – Supplemental material for Alzheimer Disease: Non-pharmacological and pharmacological management of cognition and neuropsychiatric symptoms
Supplemental material, APY766123_Appendix for Alzheimer Disease: Non-pharmacological and pharmacological management of cognition and neuropsychiatric symptoms by Samantha M Loi, Dhamidhu Eratne, Wendy Kelso, Dennis Velakoulis and Jeffrey CL Looi in Australasian Psychiatry
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.