
Abstract
Objective:
The primary aim was to comprehensively describe the characteristics of a cohort of older people taking clozapine.
Method:
Participants aged ⩾ 60 had a geriatric assessment including full medical, medication and social history. Standardized screening tools for cognition, function, comorbidity and antipsychotic side effects were administered and descriptive statistics utilized.
Results:
Thirteen patients were eligible to participate and 10 were assessed. The mean age was 69 years. The mean clozapine dose was 309 mg/day and mean duration of use was 10 years. All participants had executive dysfunction, and half had cognitive impairment. The mean number of co-morbid conditions was five. Seven people met the criteria for polypharmacy. Eight people experienced moderate–severe antipsychotic-related side-effects. The majority demonstrated impaired physical functioning.
Conclusions:
This cohort of older people taking clozapine experienced considerable morbidity, functional and cognitive impairment. We suggest routine screening of cognition and function in clozapine patients aged ⩾ 60 years. Those screening positive should be considered for further assessment by Older Person’s Mental Health Services and/or a Geriatric Medicine service.
The physical health of mental health consumers is poor due to a combination of lifestyle risk factors and barriers to accessing appropriate assessment and treatment. 1 These difficulties may be amplified in older people with mental illness who are likely to experience more co-morbid conditions, in addition to functional and cognitive limitations, impacting access to health care. 2 Better integration and coordination of care is needed, aiming for ‘seamless services’ which meet older persons’ social, physical and mental health needs. 2
In our adult mental health service (AMHS) patients prescribed clozapine are monitored in a dedicated Clozapine Clinic, coordinated by a Clinical Nurse Consultant (CNC) with monthly reviews and prescriptions by rotating psychiatry registrars and a psychiatrist 6-monthly. The Older Person’s Mental Health Service (OPMHS) manages people aged ⩾ 65 on clozapine where they have comorbid age-related health conditions (e.g. dementia) or functional disability, first presentation of mental illness in late-life, and/or people who have not been seen by an AMHS in the preceding 5 years. 3
In older people the clinical efficacy of clozapine must be balanced with greater vulnerability to adverse effects.4,5 Previous Australian studies of clozapine use in older people have been retrospective and described the indications, dosage, side-effects and reasons for discontinuing clozapine,6,7 but not medical comorbidity, physical function, or cognition. One study of older patients with ‘refractory primary psychosis’, found a mean comorbidity of 1.4 physical illnesses/individual. 8 The mortality rate for older people on clozapine in one study was equivalent to that of people taking other antipsychotics, and readmission rates were significantly lower on clozapine than for the five-year period prior to clozapine use. 9
The aim of this pilot study was to comprehensively describe a cohort of older people on clozapine in terms of cognition, prevalence of polypharmacy, functional status, medical co-morbidity and side-effect burden.
Methods
This cross-sectional study was conducted in a large metropolitan teaching hospital and associated community mental health service in Sydney, Australia. All patients receiving clozapine prescriptions via the AMHS or OPMHS aged ⩾ 60 years at the time of study commencement were eligible to participate.
Participants were identified from the online clozapine-monitoring database and recruited by their mental health clinician at routine clozapine review. Written consent was sought from participants or, where assenting but unable to give informed consent, from their person responsible. Ethical approval was granted by the local Human Research Ethics Committee.
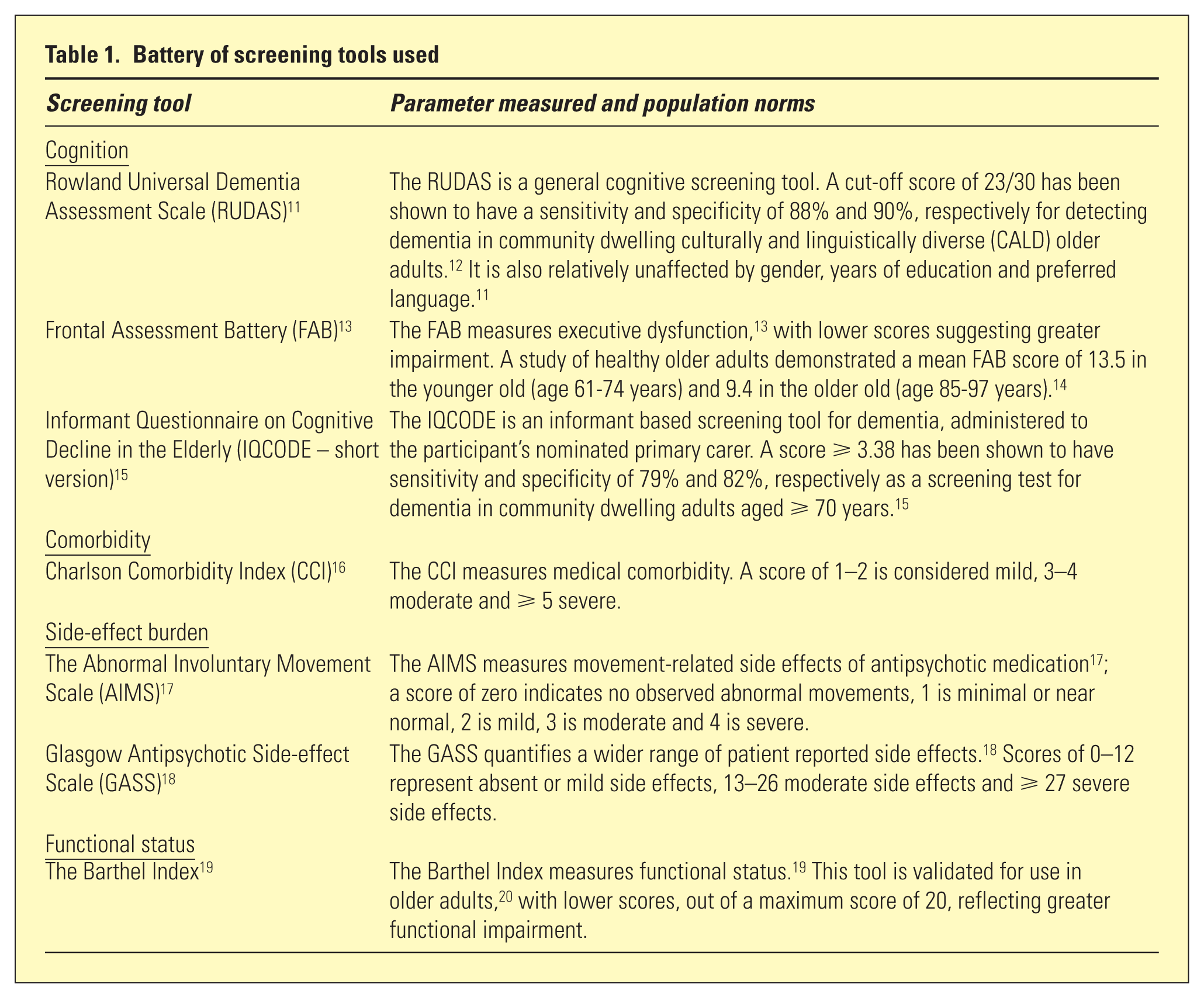
A geriatric assessment was conducted by a geriatric medicine Advanced Trainee (JB), with a Healthcare interpreter when required. Data collected included demographics (age, gender, English-speaking status, accommodation type, general practitioner (GP) contact, duration of clozapine treatment and dose), medical history (including falls in the year prior), and medications (including need for supervision). Polypharmacy was defined as taking ⩾ five medications. 10 Screening tools were administered to measure cognition, comorbidity, side-effect burden, and functional status (see Table 1). Medical records were reviewed and/or the GP contacted to corroborate data gathered. Descriptive statistics summarized the data.
Battery of screening tools used
The demographic characteristics of participants
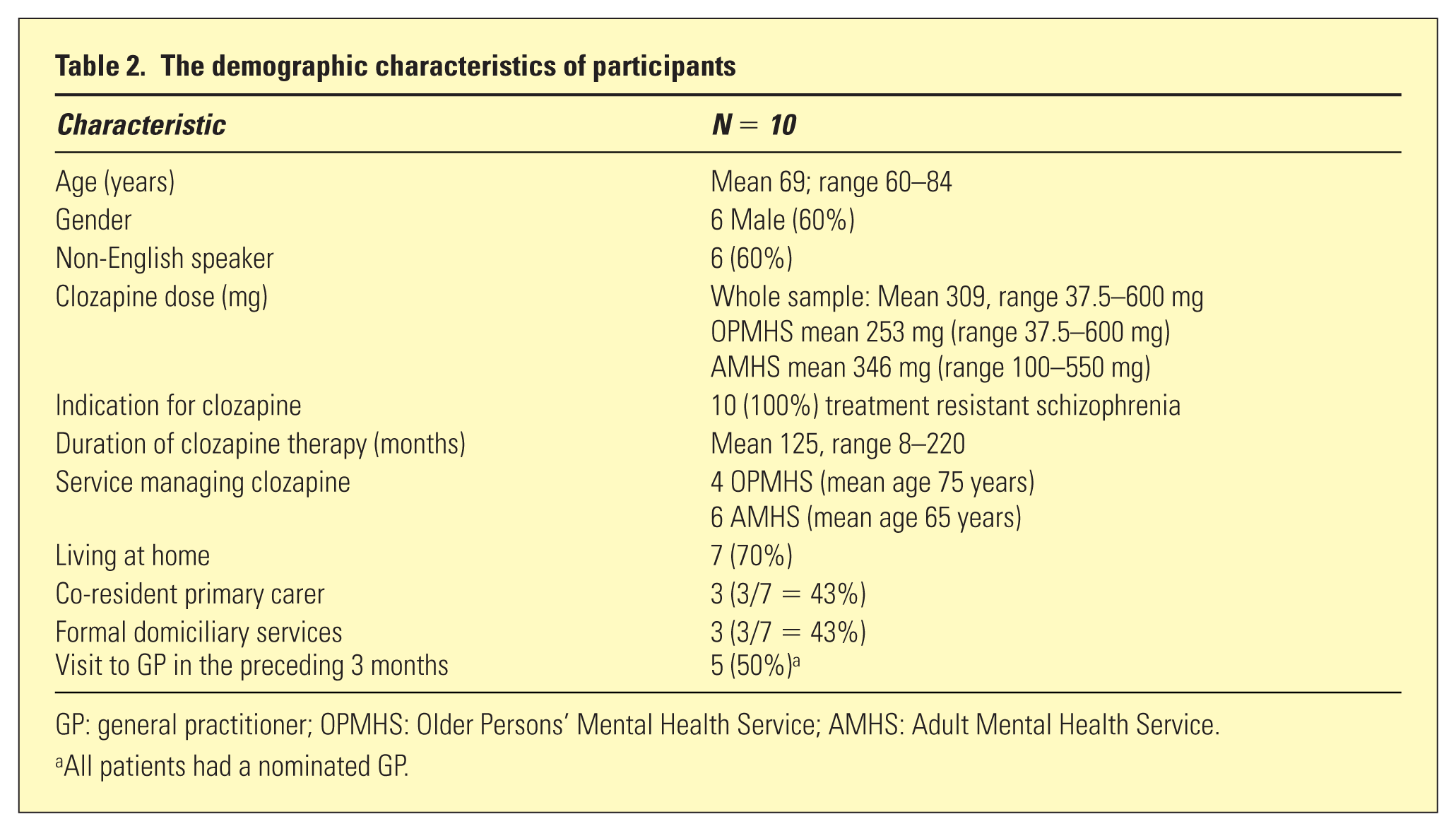
GP: general practitioner; OPMHS: Older Persons’ Mental Health Service; AMHS: Adult Mental Health Service.
All patients had a nominated GP.
The clinical characteristics of participants
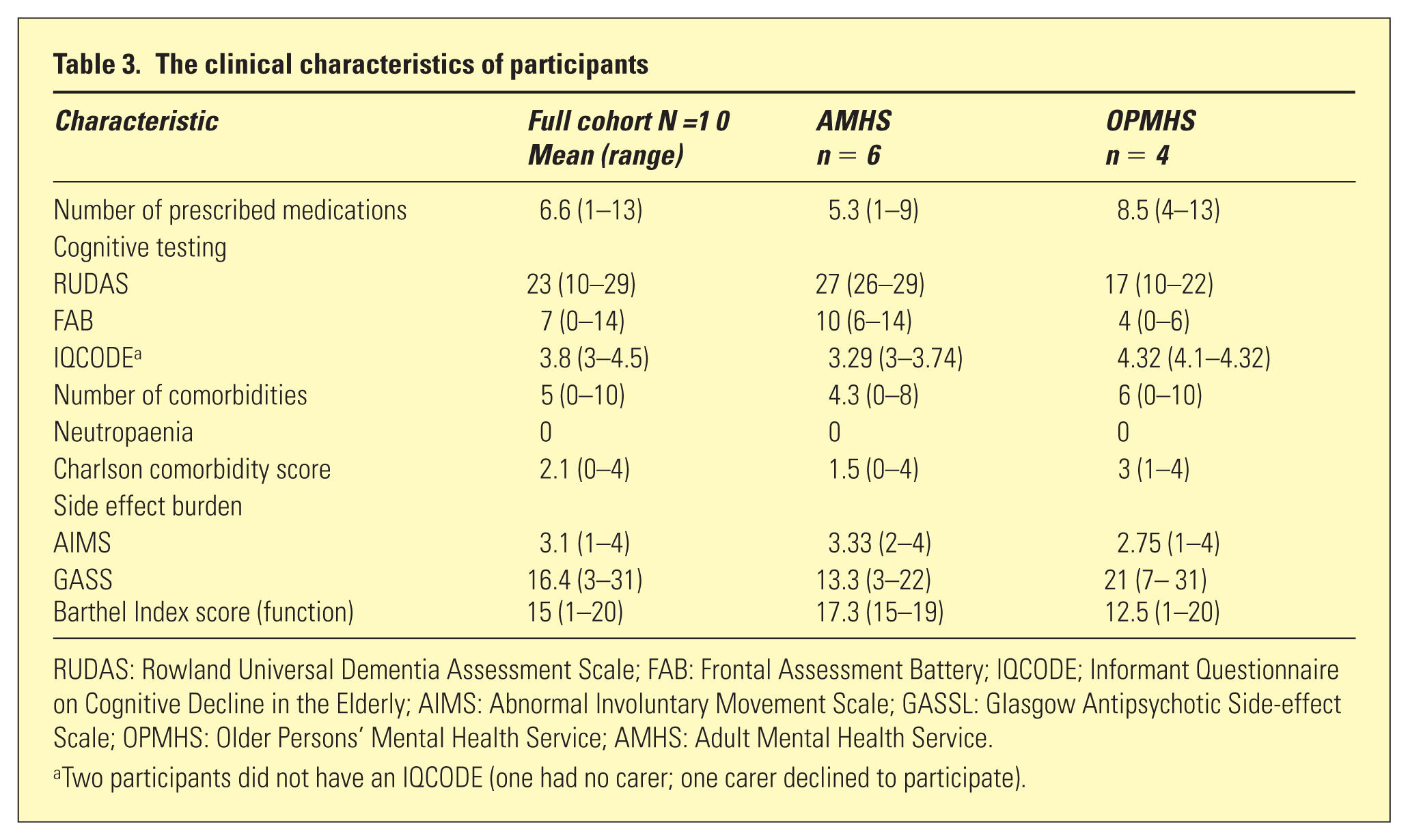
RUDAS: Rowland Universal Dementia Assessment Scale; FAB: Frontal Assessment Battery; IQCODE; Informant Questionnaire on Cognitive Decline in the Elderly; AIMS: Abnormal Involuntary Movement Scale; GASSL: Glasgow Antipsychotic Side-effect Scale; OPMHS: Older Persons’ Mental Health Service; AMHS: Adult Mental Health Service.
Two participants did not have an IQCODE (one had no carer; one carer declined to participate).
Medications
Seven participants had polypharmacy, and three in this group had fallen within the last year. Eight patients self-reported a need for medication supervision; of these, one was unsupervised (living alone without a carer or formal services) and three were residents in aged care facilities.
Cognition
Five individuals screened positive for cognitive impairment on the Rowland Universal Dementia Assessment Scale (RUDAS) or Informant Questionnaire on Cognitive Decline in the Elderly (IQCODE). All participants scored poorly on the Frontal Assessment Battery (FAB); only one participant scored >12. Most (80%) individuals screening positive for cognitive impairment met criteria for polypharmacy.
Comorbidity
The mean number of medical comorbidities was 6.2 in those with cognitive impairment compared with 3.8 in participants without. Four participants had fallen within the last year.
Side effect burden
All participants reported side effects. Eight participants were rated moderate-severe on the Glasgow Antipsychotic Side-effect Scale (GASS) or Abnormal Involuntary Movement Scale (AIMS).
Functional status
The mean Barthel Index score was 13.2 in participants screening positive for cognitive impairment compared with 17.6 in those with normal cognition. The two participants scoring lowest (0–13) were cognitively impaired on all screening tools, were taking 12 and 13 medications respectively, had fallen within the last year, and had moderate severity co-morbidity, but they also had the lowest side effect burden scores.
Discussion
As far as we know this is the first study characterizing the medical, functional and cognitive profile of older people taking clozapine. The clozapine dose range was wide, with the mean dosage above that published for older people of 25–100mg/day 5 (although higher doses have been reported for older people with schizophrenia on long-term clozapine), but similar to other Australian studies.6,7 All participants experienced adverse effects of clozapine. Generally high AIMS scores may have reflected prior antipsychotic treatment or current clozapine dose and plasma levels (not examined), the latter potentially modifiable. Movement-related side effects did not appear to relate to functional impairment according to the Barthel’s Index, as the two participants with lowest side effect burden scores were the most functionally impaired. Comorbidity was greater than in a comparable study. 8 Polypharmacy was common and has been associated with increased risk of falls. 10 The mean duration of clozapine use was > 10 years, significantly longer than a comparable Australian study. 7 All participants had significant executive dysfunction, which may have been attributable to chronic schizophrenia, medication adverse effects, or a neurocognitive disorder. The prevalence of dementia was high, prompting consideration of dose appropriateness and need for specialist review. 5 Relationships between cognitive impairment, falls and polypharmacy previously noted in older people, 21 were also found.
The optimum approach to service delivery for clozapine management in older people has not been well defined. Traditionally, AMHS have managed the majority of patients on clozapine, including those who commenced clozapine in younger adulthood and are now over 65 years of age. However, this cohort of older patients on clozapine had considerable cognitive and functional impairment, polypharmacy, and medical co-morbidity. Thus, they more clearly fit a ‘geriatric’ profile in need of OPMHS, 2 with the necessary specialist training to undertake holistic assessment of all these factors, and advise management which may include clozapine dose adjustment, de-prescribing and consideration of alternatives. To more fully understand these issues a larger study assessing the clinical (including common side-effects and haematological parameters) and functional profile, and outcomes of older people on clozapine is under development (Brian Draper, personal communication).
Limitations
The small sample size limits the generalizability of results and precluded exploration of statistical associations. The cross-sectional design excluded people who ceased clozapine due to side-effects (for example, a 77-year-old male stopped clozapine due to severe neutropaenia months prior to the study period), or difficulties meeting monitoring requirements, potentially underestimating safety and practical limitations of clozapine use in older people. The full medical record of each participant was not reviewed, possibly missing common side effects of clozapine including constipation, sialorrhoea and postural hypotension, extrapyramidal signs due to other antipsychotics or causes, and conclusions regarding the efficacy of clozapine compared with other treatments (crucial in the risk-benefit analysis).
The Barthel Index was not discriminatory in rating functional impairment, as only two individuals scored < 15, whereas most participants lived in a facility, had a carer, or needed medication supervision, suggesting some degree of functional dependence. Additionally, the Barthel Index does not measure instrumental activities of daily living, necessary for independent living.
Conclusions
This pilot study demonstrated that older adults prescribed clozapine have high rates of functional and cognitive impairment, polypharmacy, co-morbidity, and medication side-effects. In addition to the mandatory clinical reviews, we suggest screening for cognitive and physical functioning in adults on clozapine aged ⩾ 60 years. Routine assessment and management of adverse effects (extrapyramidal and medical) is also needed. People screening positive should be considered for specialist Geriatric Medicine or OPMH services, where further assessment for dementia, polypharmacy, co-morbidities and functional impairment may occur; a recommendation echoed by others. 5 This may improve the holistic care of older people on clozapine, who clearly have complex needs.