
Abstract
Objectives:
This study examined (i) the demographic and illness profiles of mothers admitted to Werribee Mercy MBU in Victoria, Australia and (ii) the severity of maternal depressive symptoms over the course of admission.
Method:
A retrospective audit was conducted on consecutively admitted mother–baby dyads between January 2011 and June 2015. Routinely collected maternal Beck Depression Inventory, second edition (BDI-II) scores were analysed for severity and change.
Results:
A total of 307 mother–baby dyads were admitted during the study period. The majority of mothers was partnered and educated young adults. The average length of stay was 4.4 weeks. The mean age of babies was 3.3 months. One-third of mothers met International Classification of Diseases, 10th edition criteria for two or more psychiatric diagnoses. Unipolar major depression was the commonest diagnosis. Of the 307 mothers, 125 mothers completed BDI-II on admission and on discharge, which showed a mean reduction of 16 points (p < 0.001) on discharge.
Conclusions:
This study notes the similarities between the clinical profiles of the study population with mother–baby admissions to MBUs worldwide. Maternal depressive symptoms improved by 16 points on the BDI-II over the course of MBU admission, which shows the utility of MBU admission on maternal depressive symptoms.
Postnatal depression and mother–baby attachment
In developed countries, around 15% of women experience a relapse, onset or exacerbation of clinically diagnosed postnatal depression (PND) and PND is the commonest psychiatric diagnosis in the postpartum period. 1 Maternal depression is associated with lower self-esteem and greater parenting stress. 2
Babies of mothers suffering from PND demonstrate less positive affect and involvement with their mothers, while these mothers are observed to be less sensitive and less responsive to their babies. Early attachment impacts on how the baby will interact, communicate and form relationships in later life.
Mother and baby units (MBUs) use a holistic approach by simultaneously assisting mother–baby attachment and treating maternal mental illness. For this reason, MBUs are regarded as the highest standard of care for women experiencing psychiatric issues in the first year postpartum.3–5
Study aims
Australia has the highest number of individual MBUs publishing outcome data. This study aimed to focus on (a) the demographic and illness profiles of mother–baby dyads admitted to our MBU and (b) the severity of maternal depression over the course of admission to our MBU as measured using the Beck Depression Inventory, second edition (BDI-II).
Research methods
A retrospective audit using a quantitative approach.
Participants
Participants were 307 mother–baby dyads who were consecutively admitted between 1 January 2011 and 30 June 2015 to our MBU.
Diagnoses
The treating psychiatrists made all the diagnoses prior to the mother–baby dyads’ discharge from the MBU. Diagnoses were coded using the International Classification of Diseases, 10th edition (ICD-10).
BDI-II for measuring PND
All mothers were offered the BDI-II on admission (entry) with instructions to complete it within 1 week. The BDI-II was again offered to all mothers on discharge (exit). The total BDI-II scores were calculated by nursing staff according to the scoring instructions and recorded into MBU database using de-identified hospital numbers. The researchers made no ratings.
The 21-item BDI-II measures depressive symptoms over the proceeding 2 weeks, which demonstrates good internal consistency with postpartum samples and good concurrent validity with other measures of PND. Depression severity is as follows: minimal depression (0–13); mild depression (14–19); moderate depression (20–28); and severe depression (29–63).
Data collection
The authors accessed de-identified and routinely collected data on the demographic and illness profiles from a statewide mental health database. All data were securely stored in the MBU database.
Statistical analysis
All data (standard deviation, p-values, tables and graphics) were developed and analysed using Microsoft Excel version 14.0.0 (Microsoft Corporation, 2010).
Ethics approval
Ethics approval was obtained to undertake the analysis and publish these findings.
Research findings
Demographic profile of mother–baby dyads admitted to MBU
Table 1 shows the demographic characteristics of the 307 participants.
MBU admissions: 1 Jan 2011 to 30 Jun 2015 (N = 307)
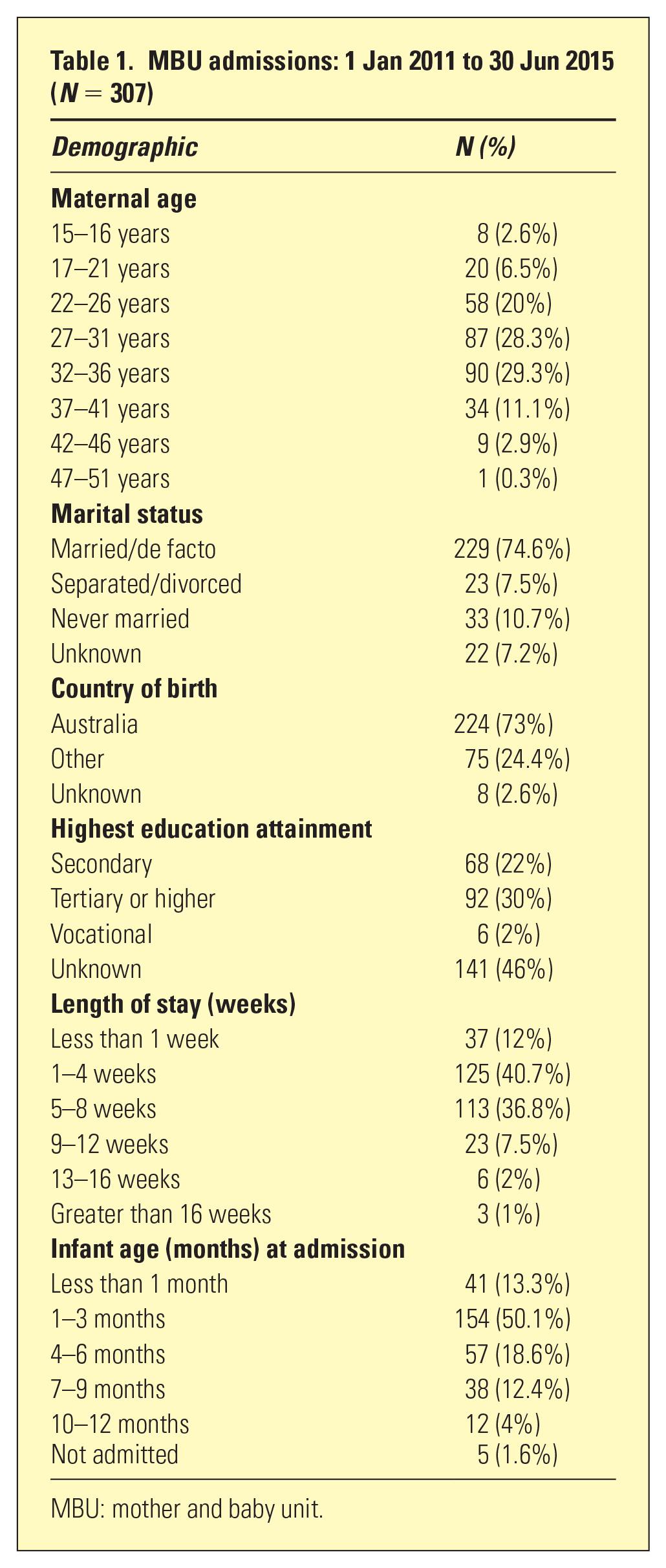
MBU: mother and baby unit.
Mean maternal age was 30 years (±6 years). Mean infant age on admission was 3.3 months (±2.8 months). The average length of stay (LOS) was 31 days (±23 days).
The majority (75%) of mothers were partnered. Most mothers (52%) had attained secondary (22%) or tertiary (30%) education. A majority (73%) of mothers were born in Australia. The remainder were born in a variety of countries.
Illness profile of mother–baby dyads admitted to our MBU
Table 2 shows that around a third of mothers met ICD-10 criteria for two or more psychiatric diagnoses; 24% (N = 73) of mothers met ICD-10 criteria for two psychiatric diagnoses and 7% (N = 21) met ICD-10 criteria for three psychiatric diagnoses.
MBU Jan 2011–Jun 2015: diagnostic profile of 307 mothers
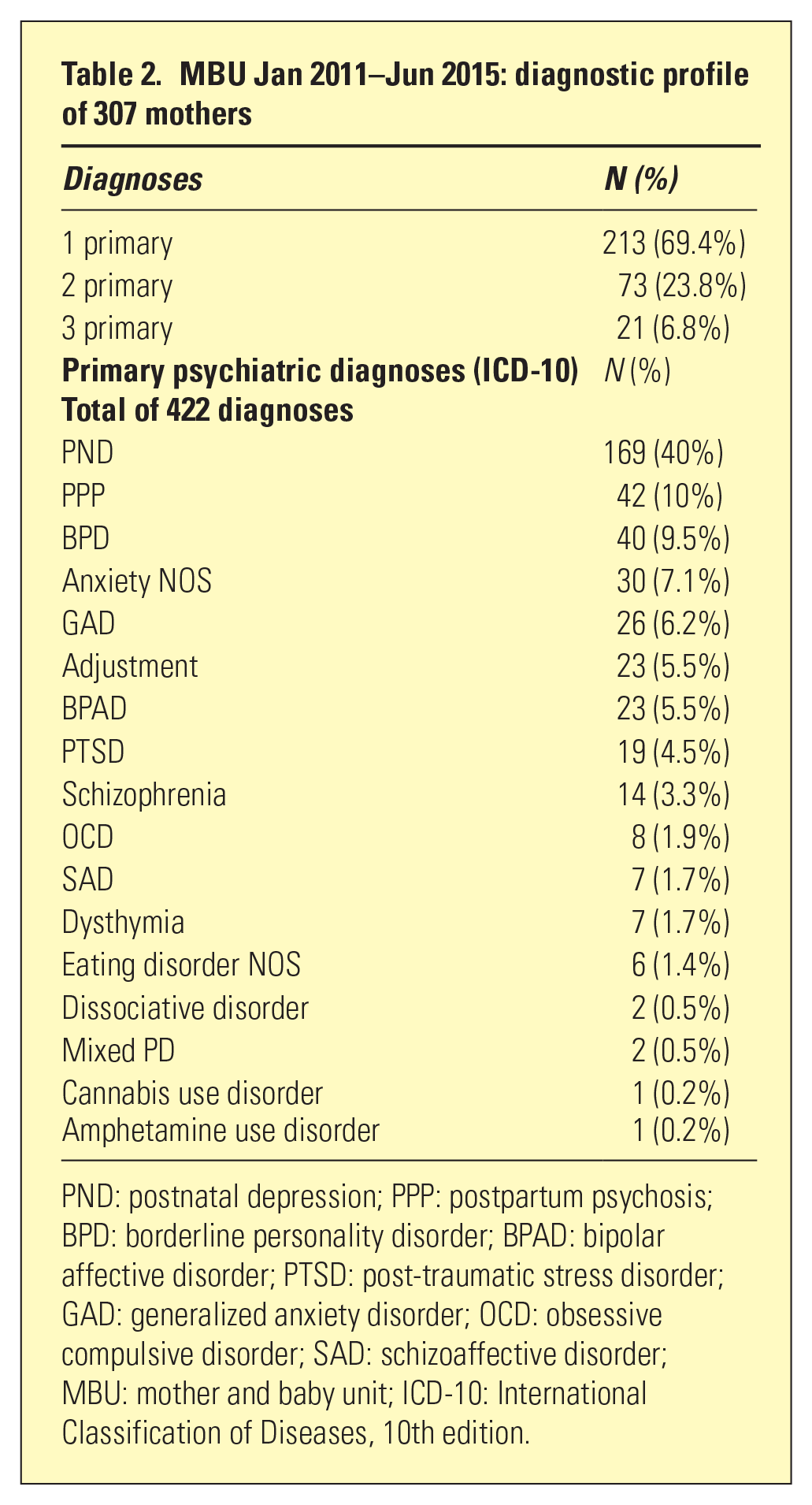
PND: postnatal depression; PPP: postpartum psychosis; BPD: borderline personality disorder; BPAD: bipolar affective disorder; PTSD: post-traumatic stress disorder; GAD: generalized anxiety disorder; OCD: obsessive compulsive disorder; SAD: schizoaffective disorder; MBU: mother and baby unit; ICD-10: International Classification of Diseases, 10th edition.
The most common primary diagnosis was unipolar depression (40%, N = 169), followed by generalized anxiety disorder or anxiety disorder NOS (13.3%, N = 56), postpartum psychosis (10%, N = 42) and borderline personality disorder (9.5%, N = 40).
Figure 1 shows the psychiatric comorbidities associated with unipolar depression. Of the 169 mothers diagnosed with PND, 53 had one or more psychiatric comorbidities. The most common comorbidities associated with unipolar depression were anxiety disorders (75%, N = 40) and borderline personality disorder (23%, N = 12).
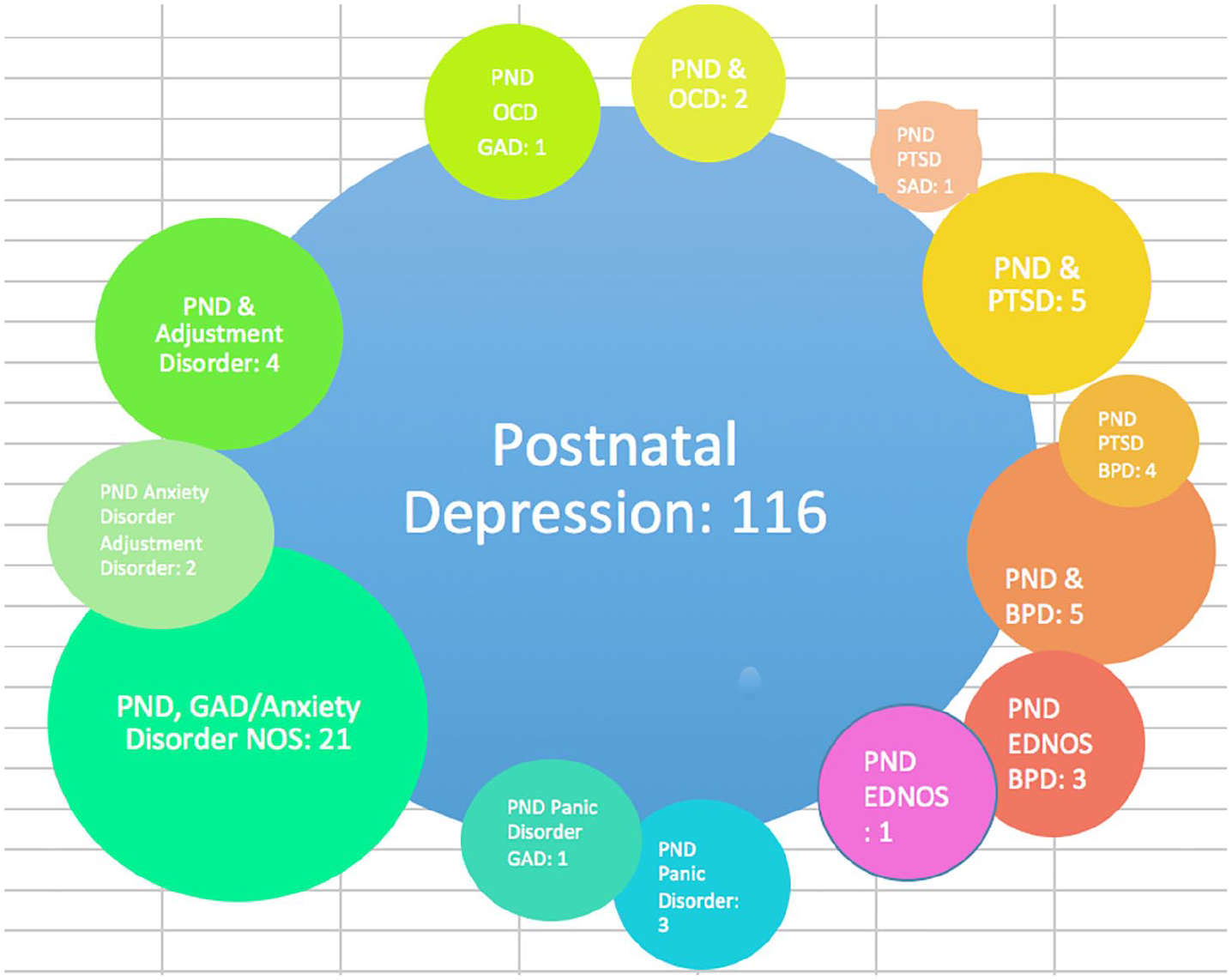
MBU Jan 2011–Jun 2015: postnatal depression and comorbidities.
Maternal BDI-II ratings
Table 3 shows that 125 of 307 (40.7%) participants completed BDI-II on admission and discharge. The average BDI-II scores of this sample were 28 on admission and 12 on discharge.
BDI-II scores: MBU Jan 2011–Jun 2015 (N = 125)
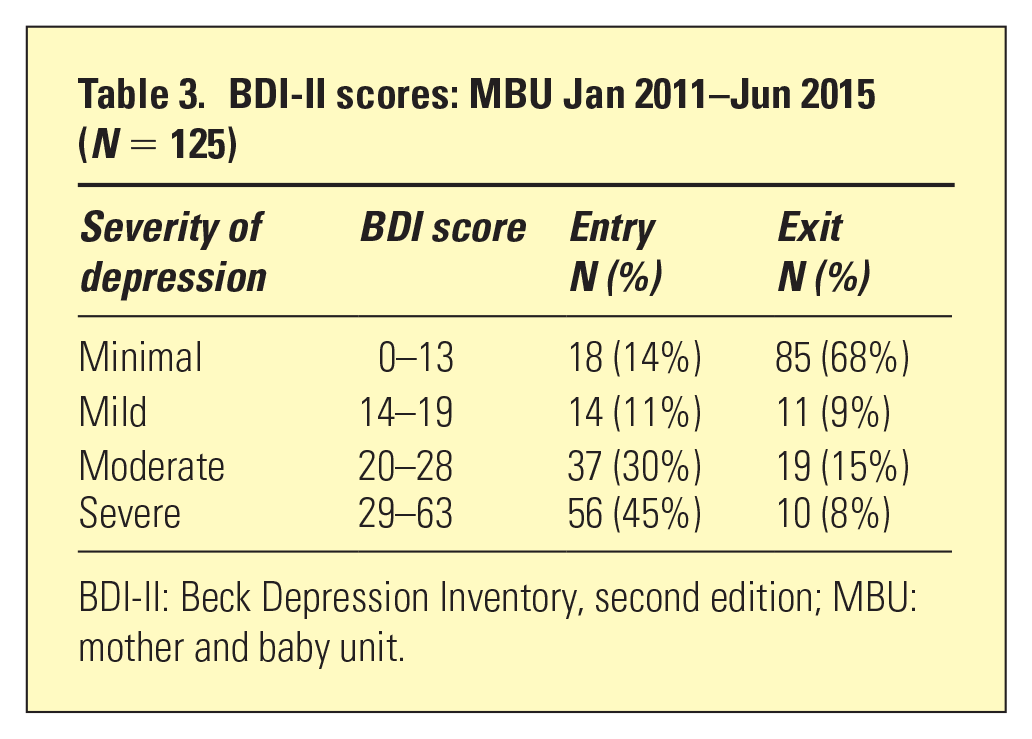
BDI-II: Beck Depression Inventory, second edition; MBU: mother and baby unit.
One hundred and eighty-two mothers had incomplete BDI-II data, so they were excluded from the final depression analysis. The average BDI-II scores of the excluded data were 27 on entry and 12 on exit. No statistically significant difference between included and excluded data was found with respect to the average BDI-II score on entry and exit.
BDI-II scores were not matched with the underlying psychiatric diagnoses, as the aim of this study was not to examine the ability of BDI-II to identify PND.
Maternal BDI-II ratings over the course of admission
Figure 2(a) shows the change in BDI-II scores in participants who completed the BDI-II on admission and discharge. There was a statistically significant reduction in BDI-II score from a mean of 28 on admission to a mean of 12 on discharge (p < 0.001).
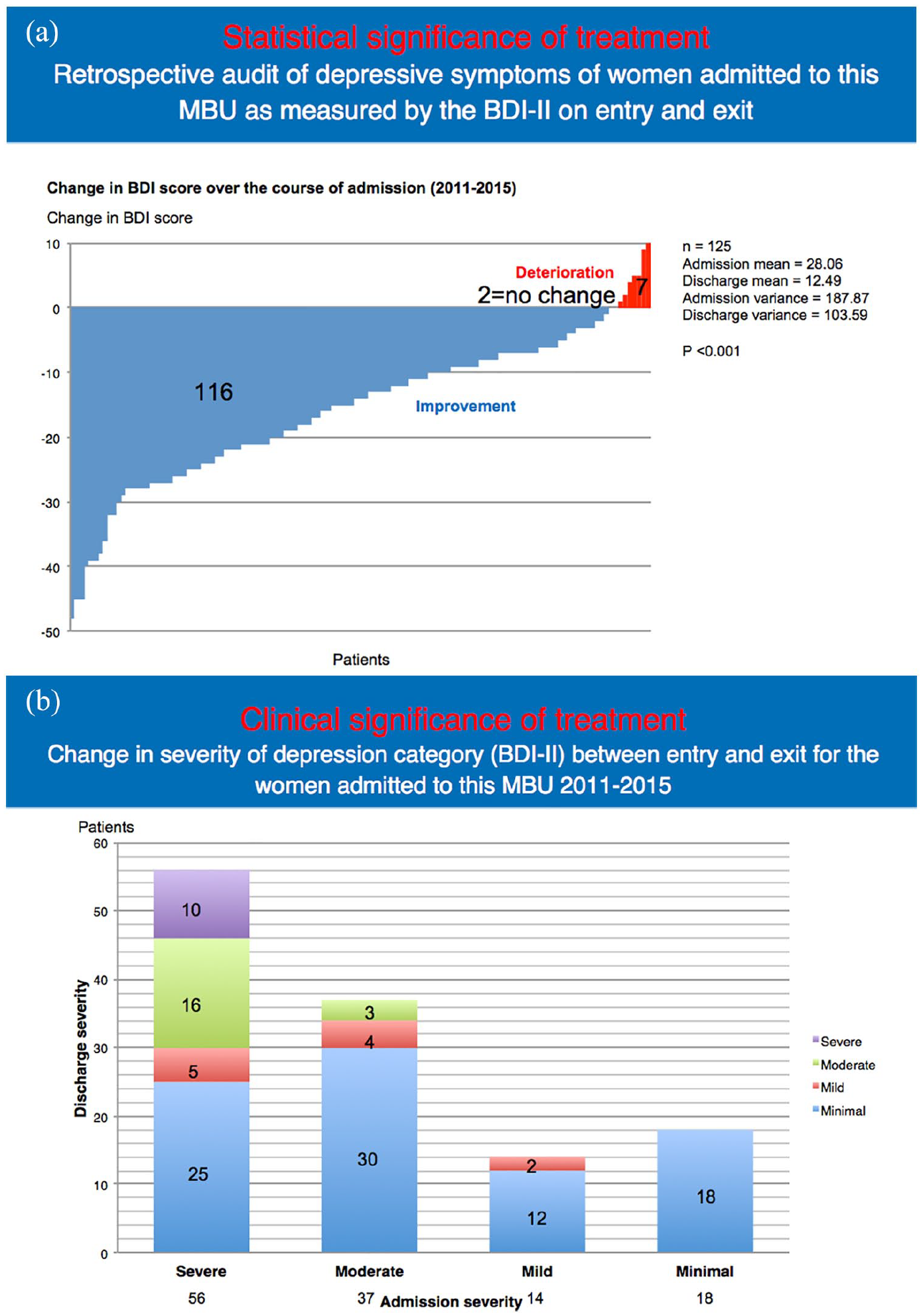
Of 125 participants, 116 (92.8%) reported an improvement in depressive symptoms, which is demonstrated by a reduction in BDI-II score of between 1 and 50 points (shown in blue); 7 of 125 (5.6%) participants reported a worsening of depressive symptoms, which is demonstrated by an increase in BDI-II score of between 1 and 10 points (shown in red).
Figure 2(b) shows the BDI-II severity category for the participants who completed the BDI-II on admission and discharge, where a shift from a higher severity category to a lower severity category (red to orange or orange to green) represents a clinically significant improvement in maternal depressive symptoms.
Research discussion
Demographic profile of mother–baby dyads admitted to our MBU
This is the first quantitative analysis of data from our MBU. Similar to published data from worldwide,6–13 the mean maternal age was 30 years (24.3–33.5 years worldwide); mean infant age was 3.3 months (2.4–7.8 months worldwide); and average LOS was 4.4 weeks (1–11.6 weeks worldwide).
Three-quarters of the mothers in our study were partnered. Partners have been a primary focus of only two previous studies. One German study with 31 partners found that only a third of partners could be described as ‘supportive partner or competent father’ and that women with supportive partners had a shorter stay in the MBU. 14 The German study also highlighted the high rate of partners with psychiatric disorders. A qualitative interview of six fathers in the United Kingdom found that fathers were facing their own difficulties adjusting to parenthood and lacking the necessary skills to help the partners, children and themselves. 15
At least one-half of the mothers in our study had completed secondary or higher education. It is difficult to draw conclusions as a significant proportion (46%) of women did not respond to the education screening question. Previous studies suggest that low education attainment may be a risk factor for maternal depression.
Illness profile of mother–baby dyads admitted to MBU
Our study confirms earlier findings that unipolar depression is the most common diagnosis made during admission to MBU. One exception in the literature was an Indian sample, which found that bipolar illness (36.2%) and acute and transient psychosis (34.5%) were more common than unipolar depression (14%).
Approximately one-third of our sample had two or three psychiatric diagnoses, which is important to identify to enable a holistic management plan. The average LOS of 4.4 weeks, which is approximately 1 week longer than the average LOS in Australian MBUs, could be reflective of the complexity of some patients admitted to our MBU. Anxiety disorders and borderline personality disorder were most commonly comorbid with PND, which has implications for specific treatment modalities including CBT and DBT in addition to depression treatment.
BDI-II rating scale
The use of BDI-II for measuring postpartum depression symptoms in our MBU is unique because the Marcé Clinical Checklist and the EPDS were used in eight out of the nine studies in the literature. The Marcé Clinical Checklist may be popular because it is a comprehensive summary of maternal socio-demographic and diagnostic information as well as maternal clinical and parenting outcomes. Compared with the BDI-II, the EPDS focuses more on the psychic aspects of depression in the postpartum and has a defined clinical improvement score of 4 points or more. 16 Some items on the BDI-II, such as sleep loss and tiredness, are generally accepted as ‘normal’ in motherhood. However, it is important not to trivialize the ‘normal’ demands placed on the new mother.
BDI-II ratings over the course of MBU admission
In the BDI-II respondent sample, admission to our MBU had a clinically beneficial effect on maternal depression symptoms. According to the National Institute for Health and Clinical Excellence mental health guidelines, a clinically significant treatment effect for normal depression is a reduction of ⩾ 3 BDI-II points and for treatment-resistant depression a reduction of > 2 BDI-II points. Meanwhile, a Japanese study of 85 adults with major depression according to DSM-IV criteria proposes that a 5-point difference on BDI-II corresponds to a minimally important clinical difference, 6–9 point difference to a slight change, 10–19 points to a moderate change and 20 or more points to a large change. 17 A 16-point BDI-II difference represents a clinically significant change.
Of the respondents 23% (N = 29) continued to report depressive symptoms in the ‘moderate to severe’ category on BDI-II at discharge. Previous studies have found that up to 14% of women either did not improve or became worse from MBU admission. This subgroup of mothers needs close monitoring and coordinated follow-up in the community.
Research limitations
There is insufficient evidence to suggest that it was the admission itself that led to the reduction in BDI-II. Other factors include medication, ECT and psychotherapy. The proportion of participants with incomplete data reduced the sample size. BDI-II scores are subjective and may be over- or under- reported, which creates respondent bias. Objective ratings from the MBU staff and partners’ views would be valuable. It is not possible to make any conclusion about the impact on mother–baby attachment in this sample.
Conclusion
This study shows for the first time the clinical profile of mother–baby dyads admitted to this MBU, which are comparable to data from worldwide and means the results may be generalized. The results show that in a sample of mother–baby dyads admitted to our MBU in the first year postpartum, there was a statistically and clinically significant improvement in maternal BDI-II scores with an average reduction of 16 BDI-II points. The current study contributes to the field of perinatal psychiatry by providing new evidence on the positive impact of MBU on maternal depression symptoms.
Future MBU programme development and research recommendations
Research implications
The use of EPDS or the Marcé Clinical Checklist would allow even closer comparison of our MBU data with worldwide data. A concurrent objective measure of maternal depression, global assessment of function and mother–infant attachment would be useful.
Clinical implications
The identification of the key features of the MBU programme that improve maternal depression symptoms and integration of these features into home or community programmes would allow more women to access postpartum mental health care. Addressing the partners’ views and function as primary outcome variables and targets of intervention would be useful.