
Abstract
Objective:
The United Nations Convention on the Rights of Persons with Disabilities (CRPD), 2006 has influenced the evolution of mental health legislation to protect and promote human rights of individuals with mental illness. This review introduces how the human rights agenda can be systematised into mental health services. Exploration is made of how some principles of CRPD have been incorporated into Queensland’s Mental Health Act 2016.
Conclusion:
Although progress has been made in some areas, e.g. heavier reliance on capacity assessment and new supported decision-making mechanisms, MHA 2016 has continued to focus on involuntary treatment. A Human Rights Act 2019 has been passed by the Queensland parliament, which may fill in the gap by strengthening positive rights.
The United Nations Convention on the Rights of Persons with Disabilities (CRPD), 2006, which came into force in 2008, is the first international treaty which embeds the rights of persons with disabilities into international law. 1 It includes mental impairments in its purpose (Article 1). The CRPD is a powerful machinery against discrimination against the mentally ill as Article 4 of the CRPD requires States Parties (the signatory countries) to take measures to modify or abolish discriminatory laws, regulations and practices; and to provide programs to protect and promote the rights of persons with disabilities.1,2 As a result, various countries have amended or are in the process of re-fashioning their mental health legislations. 3 Most new mental health acts in Australia are incorporating a heavier reliance on the ‘capacity assessment’ criteria for involuntary treatment 4 and are strengthening the supported decision-making mechanisms in legislation. 5 This aligns with human rights framework by ensuring that support is provided to help a person with mental illness in decision-making and involuntary treatment is only used as the last resort, if the person lacks capacity to consent to treatment and supported decision-making provisions have been exhausted.
The CRPD highlights positive rights (economic, social and cultural rights, e.g. right to health, education, employment and social inclusion) as well as the so-called negative rights (civil and political rights, e.g. freedom from cruel, degrading or inhuman treatment, arbitrary detention and torture). 6 Most mental health laws continue to focus on involuntary treatment and negative rights. The need to legislate positive rights has been emphasised by some commentators.6,7
Principles and systematising of human rights agenda in mental health services
The CRPD sets a balancing point for all human rights and fundamental freedoms and draws on cross-cutting themes including empowerment, citizenship, recovery and community living as a viable alternative to institutional living. 8
Coercion in care, such as restraints, seclusion, forced medications, locked inpatient units, warehousing and forensic institutions, must be curtailed. 9 The optimal attainment of liberty and freedom in care processes entails systematisation of availability of practical voluntary alternatives: open doors, open communities, open dialogues, free access, community engagement, advance directives, joint decision-making and co-production of policy with stakeholders and recovery orientation of all services. 8
It is highly unlikely that an absolutist insistence on the abandonment of all forms of involuntary treatments straight away will work, but CRPD has undoubtedly opened a new debate and is setting a new horizon for psychiatry to approach. Deinstitutionalisation is a necessary step, by substituting community for hospital care and voluntary for involuntary care wherever possible and changing legislations accordingly.
In the following section, we discuss the opportunities and challenges related to incorporating human rights framework into mental health legislation by citing the example of new mental health legislation in Queensland, Australia.
Introducing a new mental health act
Review of the now repealed Queensland Mental Health Act 2000 (MHA 2000) started in 2013 with many rounds of consultations, meetings, forums and workshops held across the State. The MHA 2016 commenced operation on 5 March 2017. 10
The MHA 2016 covers many contemporary human rights principles such as recognising the same human rights as others, respect for a person’s human worth and dignity as an individual, encouragement to participate in treatment decisions, taking the person’s views, wishes and preferences into account when making decisions, and presuming capacity until proven otherwise. 10
Treatment Authority
A Treatment Authority (TA) is the basis for involuntary treatment under MHA 2016. The criteria for TA include that the person does not have capacity to consent to be treated for the mental illness. This is a change from the Involuntary Treatment Order (ITO) under MHA 2000, which stated that ‘the person either lacks capacity to consent to be treated or has unreasonably refused proposed treatment’ (Section 14f). 11 The latter was a clear violation of the spirit of CRPD, implying that a person with mental illness could be treated against their consent, even if they had capacity to consent, if the psychiatrist deemed their refusal as ‘unreasonable’. MHA 2016 supports the human rights agenda by legislating that a person can be subject to involuntary treatment only if they lack decision making capacity and when other less restrictive ways have been exhausted. There must also be an imminent risk of serious harm or serious mental or physical deterioration and no less restrictive way to receive treatment and care. When a person regains capacity for a sustained period, the TA must cease. The category of TA can be inpatient or community, the latter being the default category, unless otherwise specified.
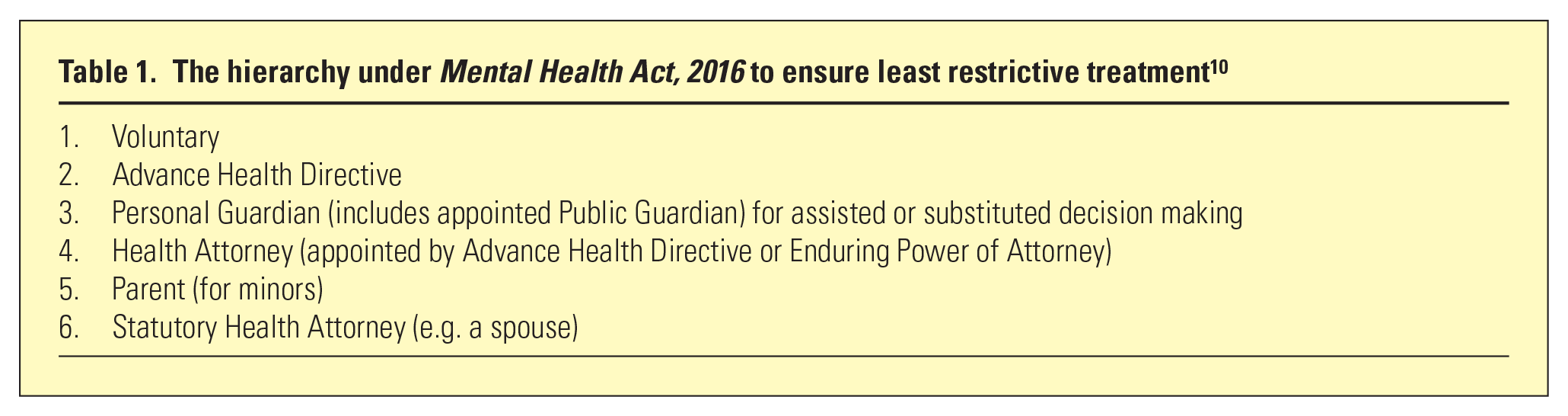
MHA 2016 allows a hierarchy of less restrictive care which should be considered before a TA is made (Table 1). Some of these mechanisms, such as personal guardian, have existed under the previous legislation but had received limited consideration or practical application in the mental health space until now. 12
The hierarchy under Mental Health Act, 2016 to ensure least restrictive treatment 10
The following table shows a steady increase in involuntary treatment since 2012. MHA 2016 hoped to reverse this trend by having stricter criteria for making the TA and being able to cease the TA sooner, however, the number of TA’s has increased in the year 2017–2018, as shown in Table 2 and Figure 1. This increase may be attributed to practice and culture of reliance on involuntary psychiatric treatment; lack of social and primary care support; lack of operationalised and well-resourced voluntary alternatives; clinician uncertainty about when capacity returns, in addition to a steady increase in population of Queensland. However, further evaluation and research is needed to understand the reasons. Of the 4764 TA’s as at 30 June 2018, 3924 (82%) were community category and 840 (18%) were inpatient. 14
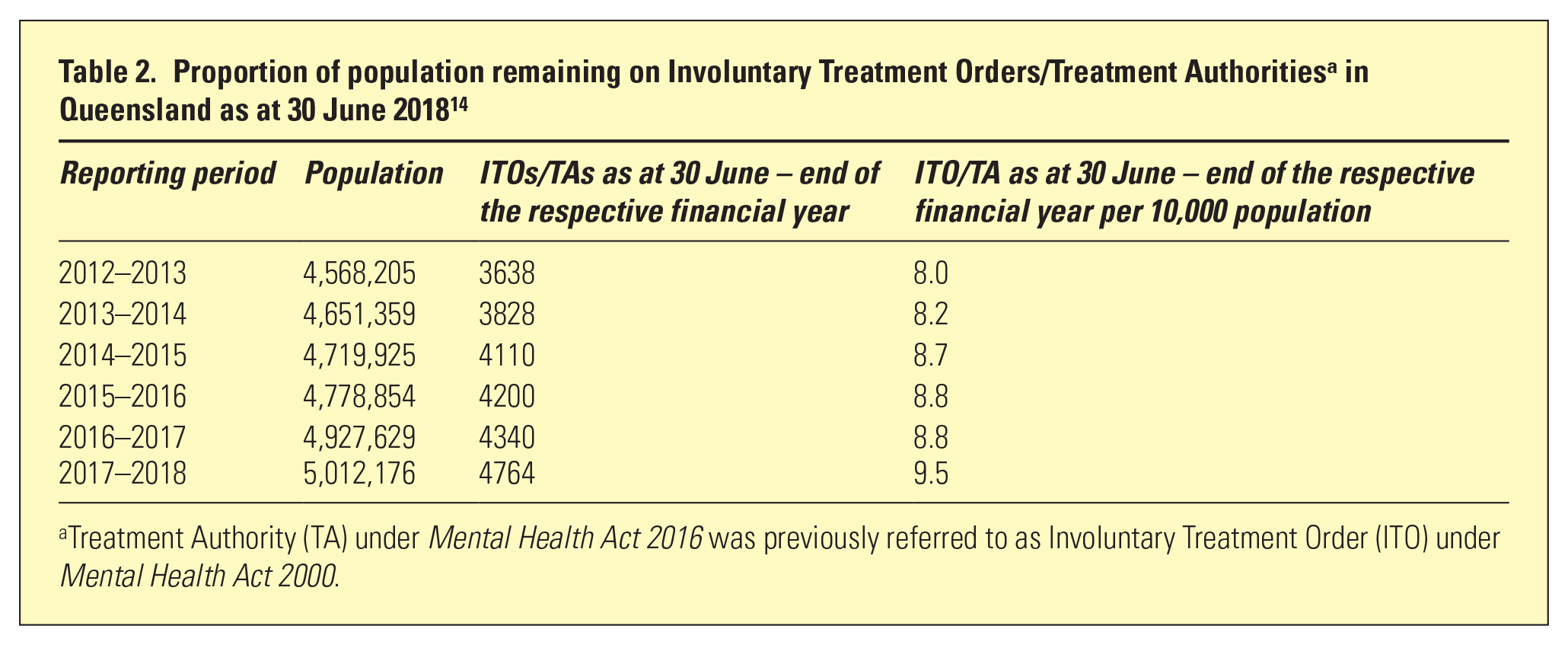
Treatment Authority (TA) under Mental Health Act 2016 was previously referred to as Involuntary Treatment Order (ITO) under Mental Health Act 2000.
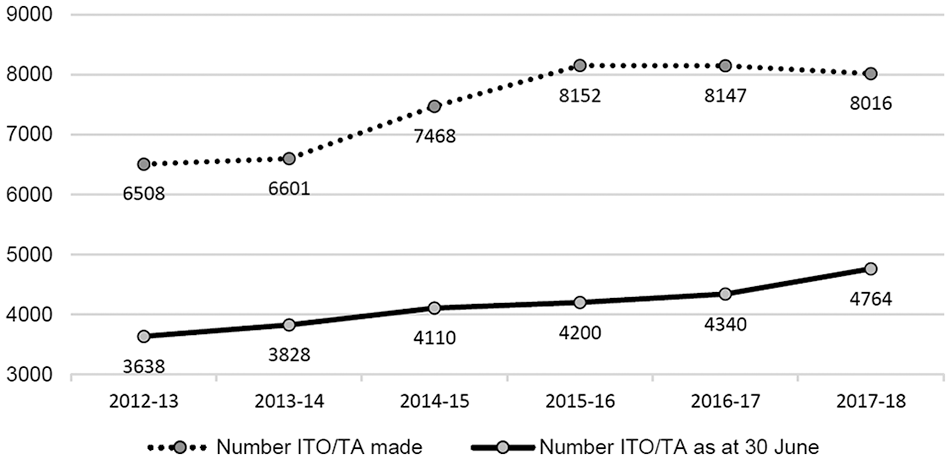
Comparison of ITOs and TAs made and as at 30 June across reporting periods. 13
Advance Health Directives
An Advance Health Directive (AHD) is made under the Powers of Attorney Act 1998, 15 which is the same as used for the treatment of physical illness, and adapted for mental health conditions. An AHD enables a person to give directions about their healthcare and comes into effect if the person loses capacity to make healthcare-related decisions in the future.
AHDs can cover things such as views, wishes and preferences about treatment and care (e.g. medication, therapies, electroconvulsive therapy and disclosure of information), the use of physical restraint and inpatient treatment. All admissions under an AHD must be reviewed within 14 days to ensure that AHD-consent is still appropriate and appointing an attorney to consent to healthcare.
AHDs cannot cover seclusion or mechanical restraint as attempts are being made to reduce these across Australia. The AHD is to be used only if clinically appropriate. Evidently, some would see AHD as a futile exercise in such case, if it can be ruled out by clinicians. However, if a TA is made for additional reasons, clinicians must honour the AHD as much as possible. Between 1 July 2017 and 30 June 2018, there was a 46.5% increase (from 402 to 589) in the number of AHDs made by patients who had been involuntary, while voluntary patients AHDs increased by 3.9% (from 916 to 952), possibly indicating that those who had experienced involuntary care were taking steps to be more in control in the future. 14
Personal Guardian
A Guardian can be appointed by Queensland Civil and Administrative Tribunal (QCAT) to make decisions for the consumer under Guardianship and Administration Act 2000. 12 Given the sensitive nature of this issue, the Public Guardian has issued a position statement on the interface with MHA 2016, stating that all decisions are to be considered on a case by case basis, and where a client objects to treatment, the more appropriate mechanism for providing treatment and care is under the TA with appropriate legislative procedural safeguards and review mechanisms under MHA 2016. 16
Independent Patient Rights Advisers
Independent Patient Rights Advisers (IPRAs) are statutorily recognised and funded under MHA 2016. In the interest of independence, IPRAs are not employed by the mental health service. However, some are employed by the same hospital and health service of which mental health service is a division, and hence, their ‘independence’ may be debatable. IPRAs ensure that consumers are advised of their rights, help them communicate their views, wishes and preferences, and provide support at MHRT hearings. A total of 28 IPRA positions were funded across all public sector authorised mental health services. 14 In 2017–2018, IPRAs had 12,356 interactions with consumers and/or support persons, and provided 18,859 service delivery activities. 14
Changes in criminal justice system to support human rights
Queensland Magistrates Courts now have new powers to dismiss charges if the person appears to have been of unsound mind at the time of the offence or is currently not fit for trial. The Queensland Health Court Liaison Service provides free assessments of persons, which supports timely disposition of court matters and assists into treatment options. Moreover, under MHA 2000, a person under TA charged with any offences was automatically referred for unsoundness of mind and fitness for trial assessment. MHA 2000 respects patient choice and supported decision regarding whether they wish to apply for unsoundness of mind defence or go through normal course of law. There is evidence that the number of psychiatrist reports required has reduced dramatically. 14 This is expected to decrease the number of individuals going on Forensic Orders.
Conclusion and way forward
While progress has been made in some areas, e.g. capacity-based criteria for involuntary treatment and strengthened supported decision-making provisions, MHA 2016 continues to focus on involuntary treatment and there is a scope for further improvements. A Mental Health Act can be both practical and programmatic: it should start from where services are presently but can, and should, also provide a way forward in terms of humane clinical management and facilitating human rights. It can legitimately prompt government to ensure safe and well-staffed community residential and support re-provision. A new act ideally should provide a lead time to do so as patients and clinicians become more comfortable with the inherent principles.
Evaluation of the implementation of MHA 2016 has incorporated whether key changes to the legislative scheme have been implemented effectively and if the objectives and principles have been applied. 13 Further evaluation and research is required into the effect of legislative changes on actual human rights provisions. As case law develops, there would be clearer direction leading from principles to practice.
A dedicated Human Rights Act 2019 has been passed by the Queensland parliament, which includes right to education (Article 36) and right to health services (Article 37). 17 This aims to ensure positive rights for everyone, not just the individuals with mental illness. The interface between Mental Health Act and Human Rights Act merits further research.
There is an emerging evidence base for the proposition that optimizing human rights is inherently therapeutic and contributes to healing. Effective action on the basis of human rights framework includes challenging social exclusion and inequality, by acting on social determinants of health like quality and stability of home, work, income, supports and social participation. Political, legal and social action has to be combined with our own emancipation, as mental health clinicians, from institutional thinking and practices in mental health and social care, to improve the prospects of a whole life and full citizenship and rights for persons with mental illness. 8