
Abstract
Objective:
Increasing options for the delivery of community-based care may be one way to reduce inpatient bed pressures. This study set out to examine the effect of community-based step up/step down (SUSD) care on hospital usage for service users with multi-service usage.
Methods:
A retrospective audit was undertaken of the medical records of all individuals admitted to a SUSD unit over a 2-year period, calculating inpatient bed days for the 12 months prior to, and the 12 months after, the SUSD admission.
Results:
There was a statistically nonsignificant decrease in bed days in the 12 months following admission.
Conclusion:
It is possible that inpatient bed day reduction may not be an appropriate outcome measure for a service built on principles of personal recovery. How to translate recovery-outcomes to justifiable financial benefits for services requires further consideration and alignment of values with reporting measures.
One way to reduce pressure on public mental health service budgets is through reducing inpatient bed days. 1 In line with providing care in the least restrictive environment, increasing options for the delivery of community-based care may be a key pathway to reducing inpatient bed pressures. Across Australia, step up/step down (SUSD) units are being established to provide community-based hospital alternative care during periods of sub-acute relapse for people experiencing sustained mental illness. In 2017, a mental health service in New South Wales established a SUSD unit in inner Sydney to assist clients of the mental health service to avoid hospitals during periods of crisis (step up) as well as to assist their transition back into the community following an acute inpatient stay (step down). The SUSD unit intends to provide a safe environment to access medical, psychological, and social interventions in a residential setting. The service is based on the Prevention and Recovery Care (PARC) model, 2 offering short-term (up to 28 days) voluntary care in a residential setting through a service partnerships between government and nongovernment community mental health services. Similar services have also been established at other sites around Australia.3-7
Evaluations of these services have demonstrated mixed results related to impacts upon admissions to inpatient units, including findings of significant reductions in inpatient mental health bed days, 8 significant increases in inpatient readmissions and presentations to emergency departments, 4 and no significant differences in inpatient mental health service use. 9 A recent study suggested that significant variation in service use outcomes should be anticipated for clients with multiple admissions to community-based residential mental health services who were more likely to have had significantly greater number and length of previous inpatient admissions, as well as significantly longer index admission to community-based residential mental health services. 10
For the current study, a comprehensive 12-month evaluation of the local service identified that there was fidelity to intended scope of service when examining demographics, referrals, and length of stay; favorable clinical outcomes for consumers; and a functioning partnership model between the organizations co-delivering the service. Importantly, feedback from service users was positive. In a purpose-developed recovery questionnaire, service users reported the main recovery-related benefits of the service being the interactions with staff and the homely environment. Service users also valued the freedom, social interactions, safety of the environment, and structure of the days. As part of the overall evaluation, it was identified that there was an increasing number of service users, admitted to the unit in the first year due to high support needs who otherwise would require frequent hospitalizations and high-level community care. This study set out to examine the effect of the community-based SUSD care on hospital usage for these service users with multiservice usage.
Method
A retrospective audit was undertaken. Ethics approval was gained from the local hospital ethics committee. The medical records of all individuals admitted to the SUSD unit from (service commencement) in June 2017, and discharged up until the end of June 2018 were reviewed. This yielded a population of 90, of whom a sample of 29 met study inclusion criteria. Inclusion criteria were designed with a biostatistician and required at least one discrete local inpatient mental health admission within the 12 months prior to their first SUSD admission, excluding any inpatient admission directly associated with the SUSD admission. Primary exclusion criteria included consumers transferred out-of-area or admitted to extended-stay mental health inpatient facilities within the 12 months post their first SUSD admission. Criteria were designed to isolate episodes of illness to aid analysis. Service usage from the cohort (n = 29) was extracted for the subsequent 12-month period up to June 2019. Total number of inpatient bed days for each client in the sample was manually calculated for the 12 months prior to, and the 12 months after, the SUSD admission. Descriptive statistics were calculated for the difference in before and after number of bed days for each participant, with statistical analysis via a paired t-test, with each participant serving as their own control. A non-parametric test (Wilcoxon Signed Rank) was also conducted as a sensitivity analysis. Statistical analysis used SPSS Version 25.0. 11
Results
Average length of stay in the SUSD was 23 days (range 1–29). Nearly half the study sample (n = 14; 48%) had additional admissions to the SUSD during the study period. Summary statistics of inpatient mental health bed days in the 12 months prior to and following the index SUSD admission are displayed in Table 1. There was an overall reduction of 214 inpatient bed days for the sample group (n = 29) in the 12 months post index SUSD admission, with a median reduction of 11 bed days (interquartile range [-]31 – [+]10) per consumer in the 12 months after the index SUSD admission. This reduction in bed days per consumer was not statistically significant (t = 0.721, df = 28, p = 0.477.). The sensitivity analysis also yielded a nonsignificant result (Z = −1.395, p = 0.163).
Inpatient bed days in the 12 months pre and post the study period
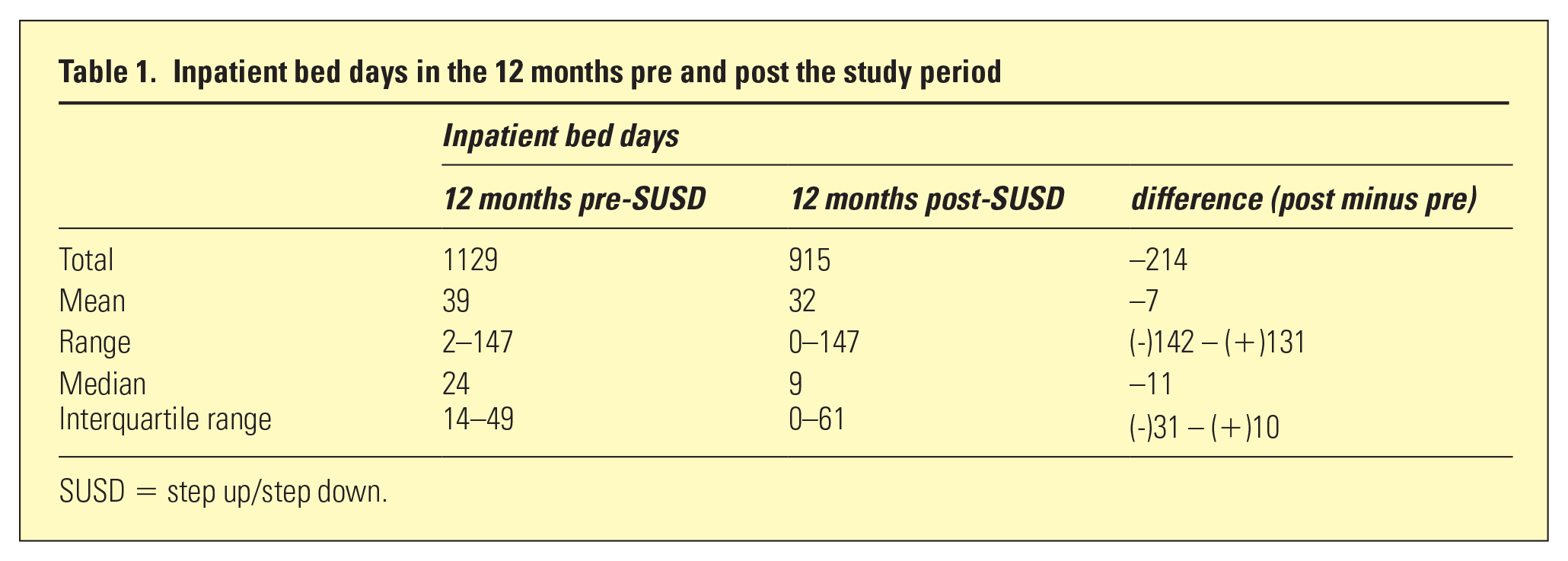
SUSD = step up/step down.
Discussion
While bed days still occurred after admission for the study cohort and the overall reduction was not statistically significant, there were less inpatient bed days in the 12 months following a first admission to the SUSD unit and it is assumed that admissions at times diverted from hospital or reduced length of stay through community transition. Any decrease in inpatient bed days provides cost benefits to services. The Australian Institute for Health and Welfare 12 costs inpatient bed days at AUD$1153 per day, suggesting that if the SUSD could be attributed to the reduction in bed days post-admission in the current study, even the reduction of 214 inpatient bed days found in the first year post commencement represents a saving of AUD$246,742. While additional admissions to the SUSD would also cost, these are estimated by the Australian Institute of Health and Welfare (AIHW) at AUD$384 per day and would still represent substantial cost savings.
The much larger evaluation of PARC services across Victoria also did not find a significant difference in mental health inpatient service use in their analysis of 20 PARC services across Victoria over 5 years of data. 9 This may speak to the challenges in evaluating such services, including identifying accurate and sensitive points of outcome measure. The units service a wide variation of individuals with diverse needs, and there is a need for consideration of how such services can measure efficacy and determine success. The current (small but expanding) literature on evaluating SUSD services is difficult to interpret across the field, due to variations in methodology, indicating a need for some way of facilitating more consistent approaches to evaluation that might support comparison across services. Issues were identified in the current study related to the quality of standard documentation, difficulty in extracting service usage data, and potential for error due to processes requiring manual extraction.
There is ongoing debate in the literature as to the validity of inpatient readmission rate as an indicator of mental health service performance. 10 Services such as the one in the current study are established based on broad principles of personal rather than clinical recovery, in line with Australian health plans and policy. This means a decreased focus on symptom reduction and restoring functioning and an increased focus on self-determination and living a meaningful life, with or without symptoms. Despite this shift, key performance indicators retain a strong emphasis on reduced service usage as an indicator of success and many evaluations (including this current study) focus on measurable collated outcomes and cost effectiveness rather than individuals. While SUSD units may reduce demand on inpatient services, they also specifically aim to enhance personal recovery and this is more difficult to measure and report. The service users from the current SUSD unit had described that the service is helpful to them and contributed to their recovery. Yet this study evolved from a need to identify a proxy measure for recovery. Inpatient admissions may indicate clinical recovery but can do little to demonstrate the personal recovery upon which the service is oriented. The benefits of a SUSD service may instead lie in the components identified by service users as beneficial (freedom, social connection, a homely environment) and the relationship of these factors to personal recovery. How to translate these recovery-based outcomes to justifiable financial benefits for services requires further consideration and alignment of values with reporting measures.
Despite the recovery focus of SUSD services, a study within a similar service in Queensland identified that staff experienced complexity in understanding what recovery-oriented practice is in relation to service delivery and recovery was varyingly seen as an outcome of care, a process that staff were to facilitate with consumers or a mindset held by consumers towards outcomes. 13 While staff provided care through a mixed lens of personal and clinical recovery, what this meant at a service level remained unclear. Similarly, the present recovery-based SUSD is searching for meaningful measures of how to determine efficacy of recovery-focused care, while simultaneously ensuring the service aligns to service user needs, and ensuring justification of funding in a climate of stretched resources. While community-based recovery-oriented care may have some impact on inpatient bed days (whether significant or not), this indeed may not be the point.
Limitations
This study had a number of limitations. If admissions were longer than the study period, only bed days that occurred within the 12 months pre and post were included. All data were manually extracted, leaving possibility of human error. Only data related to admission within the same local health district were accessible and service users may have been admitted elsewhere during the study period and not included. Inclusion and exclusion criteria determined to make analysis of the service data feasible may have inadvertently biased the results. A discrete “episode of illness” is difficult to define within this population; contiguous admissions between the inpatient units and the SUSD unit were excluded where other studies have included these episodes. 4
Footnotes
Acknowledgements
The authors thank Dr Mario D’Souza for his assistance with design and analysis; as well as all members of the Buduwa Steering Committee for their support of this work.
Disclosure
The authors report no conflict of interest. The authors alone are responsible for the content and writing of the paper.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.