
Abstract
Objectives:
Demand for places in postgraduate psychiatry training programmes has increased over recent years. All systems have capacity limits, and concerns have been raised regarding the sustainability of the current intake. This paper presents a modelling exercise to exploring the presence and strategies to resolve bottleneck in the Queensland training programme.
Methods:
Mathematical modelling based on the RANZCP training regulations and the characteristics of the accredited training programme.
Results:
A training bottleneck was identified which has been impacted by increased training intake, demand for Advanced Training certificates, and location factors.
Conclusions:
This investigation raises important questions regarding the future management of postgraduate training in psychiatry in Queensland that may be applicable more widely across Australia and New Zealand. In particular, it highlights the large impact that can result from even small incremental increases in trainees across varying levels of the postgraduate programme and the importance of limiting trainee intake in a manner proportional to the availability of mandatory terms.
Over recent years, an increasing number of doctors have sought entry into postgraduate training in psychiatry across Australia. Drivers for this may include the dramatic expansion in medical graduates over the past two decades, 1 focused initiatives to generate student and junior doctor interest in the speciality, 2 and increased service demand driving recruitment into training positions. 3 Increasing interest in psychiatry as a profession reflects a shift from the profession being historically viewed as relatively unattractive by medical students.3,4
The psychiatry training programme in Queensland is one of the largest and most diverse single training programmes across Australia and New Zealand. A single Branch Training Committee (Queensland Branch Training Committee (QBTC)) covers the entire state, with the programme including >370 active trainees, >400 training positions and >500 accredited supervisors. Diverse training experiences are available across metropolitan, regional and rural areas, with positions being available in public Hospital and Health Services (HHSs), private hospitals, private clinics and non-government organisations. There are 10 individual training sites with over 20 active trainees (range 23–60) and 19 sites with <20 trainees (six of which are private clinics/hospitals with a single trainee). Furthermore, QBTC has taken a flexible approach with regards to approval of Breaks in Training and part-time training to ensure trainees are supported to achieve and maintain work–life balance. The flexibility and diversity of opportunities make Queensland an attractive place to train.
The effective functioning of a training programme requires the ability to ensure the smooth progression of trainees through the stages of training. The availability of ‘Child and Adolescent Psychiatry’ (CAP) and ‘Consultation–Liaison Psychiatry’ (C–L) positions to meet the mandatory Stage 2 training requirements is a key rate-limiting factor to trainee progression. When demands for these positions exceed capacity, individual trainees face delays in their training progression.
Several factors add complexity to the management of trainee progression in Queensland. Importantly, QBTC has no control over trainee employment and allocation decisions, which are managed by the individual HHSs. Furthermore, there is no longer a mandatory rural training experience 5 to encourage trainee movement to HHSs, where CAP and C–L position vacancies more often arise. For these reasons, QBTC cannot direct the movement of trainees across services to limit site-level bottlenecks and vacancies. Additionally, training demand is actively driven by HHSs to encourage the employment of junior doctors as trainees rather than non-training registrars as a recruitment strategy.
Increasing demand for training entry necessitates consideration of the capacity of a training programme to support trainees to attain Fellowship in a timely manner. A modelling exercise was completed to better understand the limits on the capacity of QBTC to intake new trainees without the emergence of bottlenecks to trainee progression. This paper presents the model and the knowledge gained through the modelling process.
Methods
Mathematical modelling of trainee progression is based on: (1) Royal Australian and New Zealand College of Psychiatrists (RANZCP) regulations 6 and accreditation standards 7 relating to trainee progression; (2) trainees (new intake, Stage 1 trainee, Stage 2 trainees and CAP and C–L advanced trainees (ATs)); (3) historical variation in trainee numbers and (4) accredited training position availability (see Table 1). To develop and test the model, data on the Queensland training programme in Queensland was collated and categorised from the databases maintained by QBTC in May 2020.
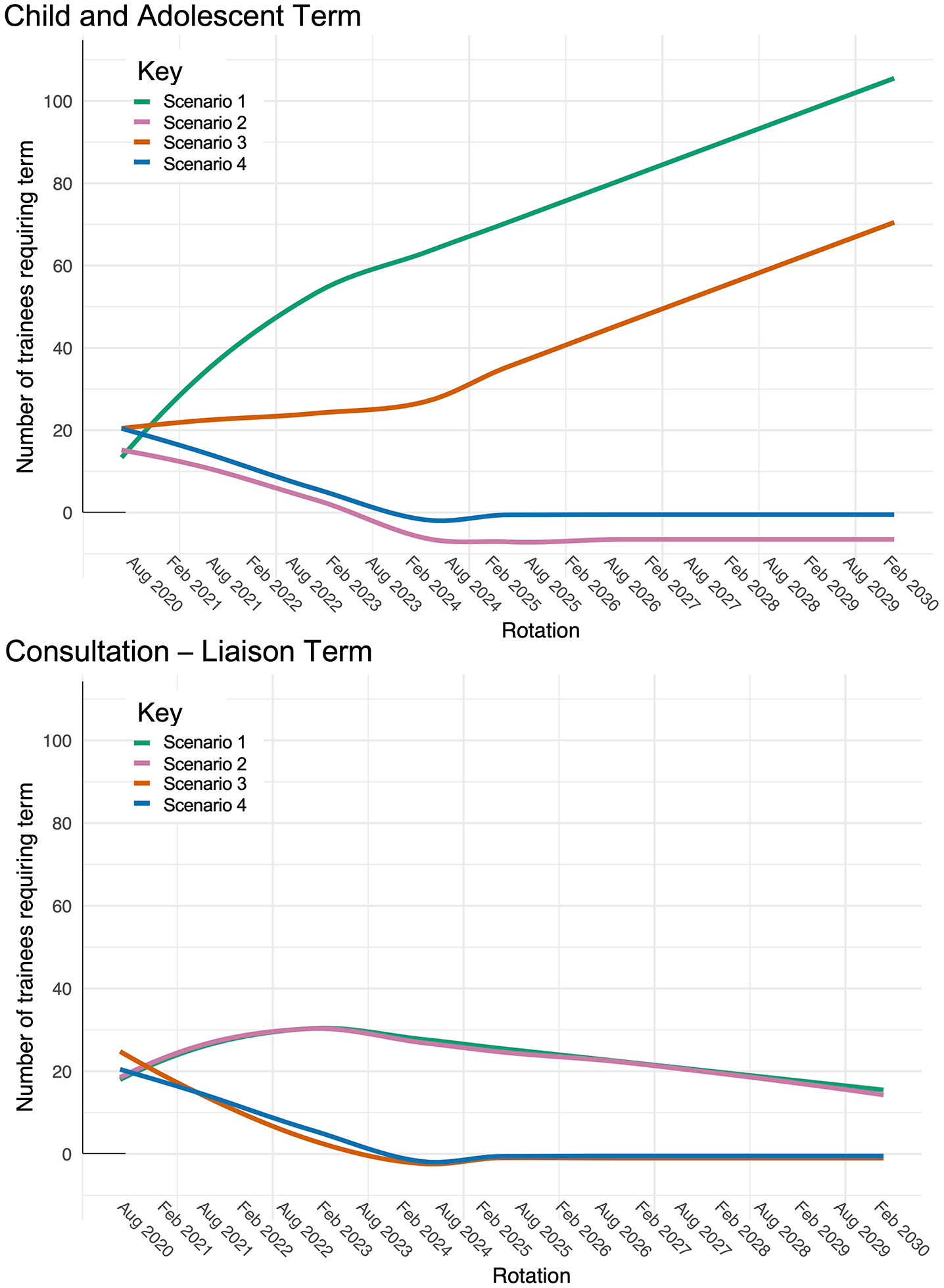
Components included in the model
Note. AT = Advanced Training (certificate), BIT = Breaks in Training, CAP = Child and Adolescent Psychiatry, C–L = Consultation–Liaison Psychiatry, FTE = Full-Time Equivalence (training time), IMG = International Medical Graduates, RANZCP = Royal Australian and New Zealand College of Psychiatrists, RPL = Recognition of Prior Learning.
Assumptions built into the model.
Delaying access until the second year limits position availability for the trainees transitioning to Stage 2 in the subsequent year and the bottleneck risk.
Results
Current training situation
The trainee intake in Queensland has demonstrated an annual growth between 3% and 5% over the last 15 years (Figure 1). Occupancy of accredited Stage 2 CAP and C–L positions at the statewide level is less than 100% (90% and 82%, respectively); vacancies predominantly occur at the regional training sites. An additional consideration is the extent to which Stage 2-accredited CAP and C–L positions are occupied by the ATs, which is a bigger issue for CAP than C–L (23% vs 5% AT occupancy, respectively).
Growth in annual trainee intake numbers (blue bars), including projected intake for Term 2 2020 based on historical data (grey bar) and trend line demonstrating average growth of 3%–5%.
Modelling training programme bottlenecks (and their resolution)
We modelled a projected growth in trainee cohort and the capacity of the training network to meet the Stage 2 mandatory term requirements. The final model is available to view online (https://espace.library.uq.edu.au/view/UQ:2368c31) and its components and assumptions are detailed in Table 1. The preferred configuration of training would be that Stage 2 trainees should access the mandatory CAP and C–L experiences in the first 12 months of Stage 2, as delaying access to the second year of Stage 2 limits flexibility to accommodate unexpected developments. This ideal principle was incorporated in the model.
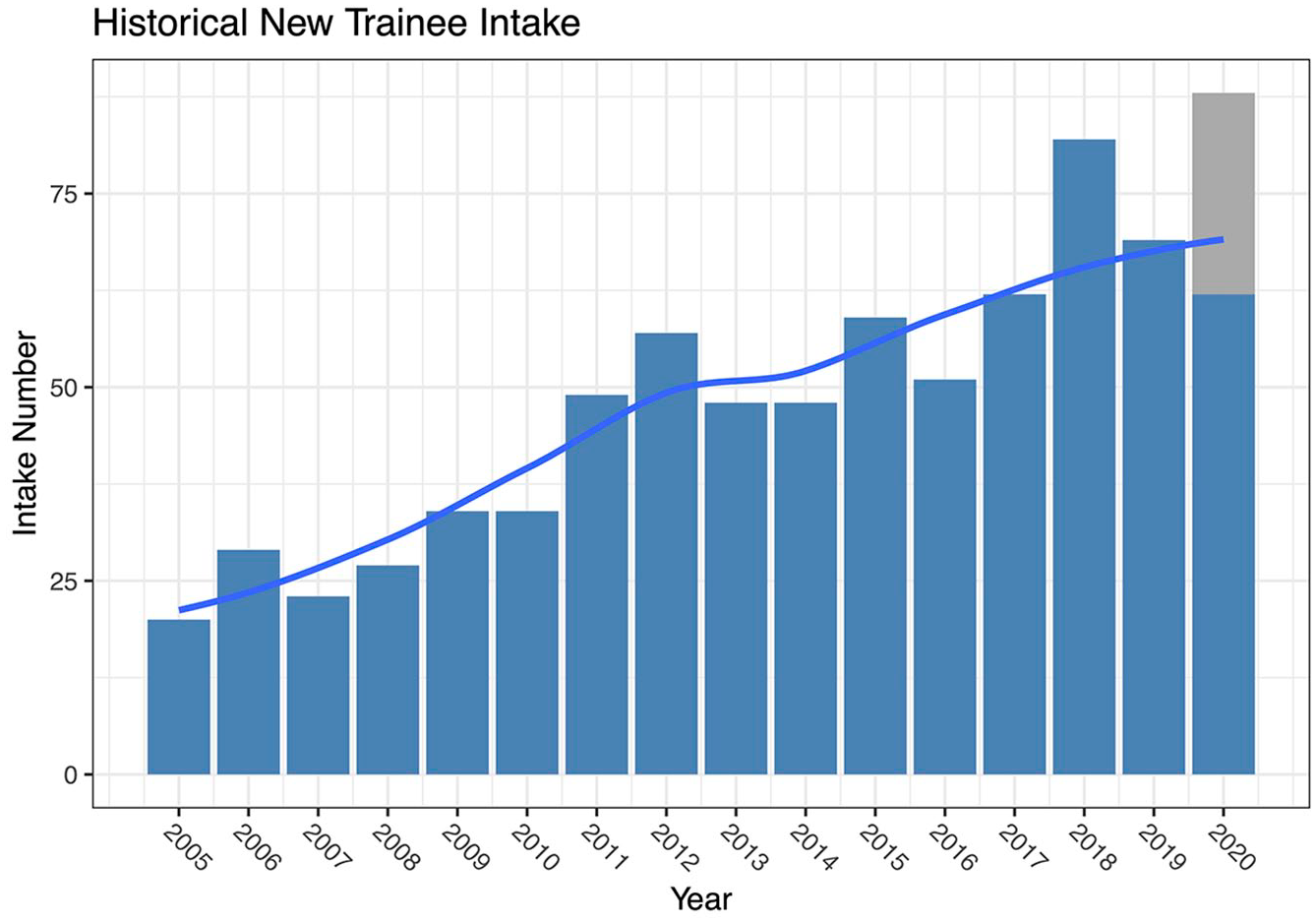
The model was applied to understand drivers of training bottlenecks in the Queensland training programme. This process indicated that the current trainee numbers are 14% and 35% greater than the number of available places for the Stage 2 CAP and C–L positions, respectively. As of August 2020, this issue immediately had affected 12%–26% of the cohort (Figure 2). Projected growth over future years results in accumulation effects, with bottleneck gradually increasing until a ‘tipping point’ is exceeded in 2025, when the problem escalates exponentially (Figure 2). The tipping point approximates the annual intake exceeding four times the number of available Stage 2 CAP and C–L training positions (i.e. the number of terms each trainee can potentially complete the mandatory terms in the 24 months of Stage 2). At this point, delayed progression to Stage 3 training becomes unavoidable for increasing numbers of trainees.
Modelling of projected impact of increase in trainees on the capacity of mandatory terms. Panel 1: Overcapacity of mandatory terms with projected worsening of bottleneck without assertive action. Note that small ongoing increases in trainee numbers (black line) result in dramatic bottleneck worsening after the tipping point is exceeded. Panel 2: Increase in trainees awaiting a mandatory term, based on 5% annual growth. The ‘tipping point’ represents the time at which the number of trainees awaiting a mandatory term is four times greater than the number of places available. From this point, the number of trainees above the line will be inevitably delayed in their training progression.
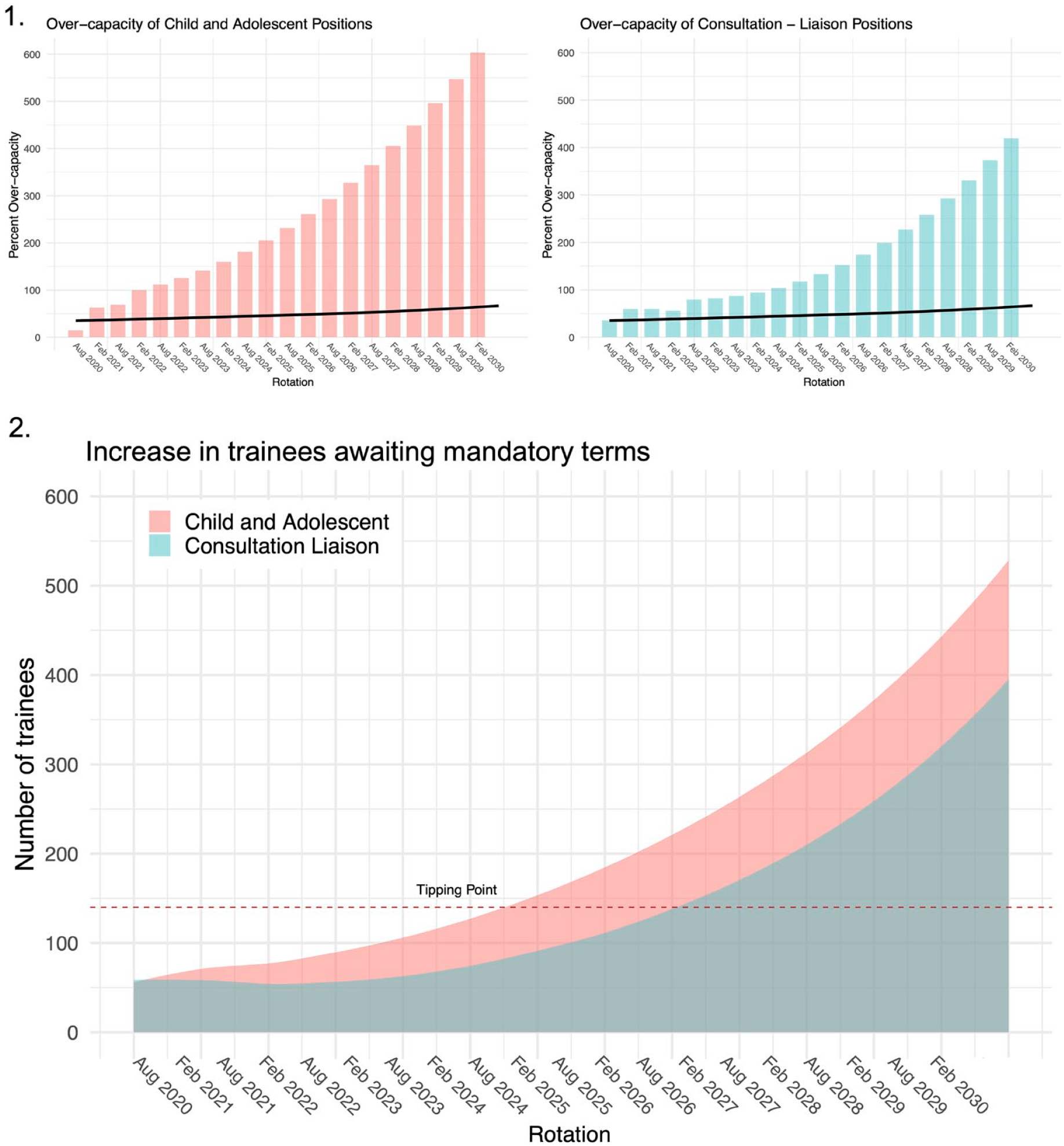
Stabilising training capacity requires limiting trainee intake to match the availability of mandatory terms. Intuitively, the ‘optimal intake’ should be capped at twice the smallest number of mandatory positions available, but adjustments are needed for key variables such as AT numbers and programme attrition rates. Modelling identified that for Queensland, a critical factor affecting trainee access to mandatory Stage 2 experiences is the occupancy of these positions by ATs completing the CAP and C–L certificates. Without concurrently restricting AT certificate intake, the emerging bottleneck worsens dramatically – and for the Queensland programme in the longer term, this is driven by CAP ATs (Figure 3, scenario 1). This is because unlike the AT CAP trainees, the AT C–L trainees minimally occupy the available Stage 2-accredited C–L positions.
Modelling scenarios for actions to resolve and prevent training bottlenecks. Modelling of scenarios for managing training programme and impact on availability of Child and Adolescent and Consultation–Liaison terms. Optimal trainee numbers were calculated at twice the number of available mandatory terms for each speciality. Scenario 1 is immediate application of determined optimal trainee numbers, with no alteration to AT occupancy of terms. CAP terms will continue to remain oversubscribed, with ongoing capacity issues, due to AT occupancy. C–L will gradually stabilise, but remain overcapacity by a small number of positions for at least 10 years. Scenario 2 is application of determined optimal trainee numbers with AT occupancy of Stage 2-suitable terms reduced to zero. This results in rapid recovery of CAP capacity, but has minimal impact on C–L capacity as very few ATs are occupying Stage 2 positions at this time. Note that CAP will have a minor oversupply of positions with this strategy, as there are more CAP positions than C–L positions, meaning that C–L term availability is the determining factor in the trainee intake cap. Scenario 3 is modest short–medium term reduction in trainee intake, with no AT limitations. This results in ongoing overcapacity in CAP, while delayed Scenario 4 is modest short–medium term reduction in trainee intake, with AT occupancy for Stage 2 CAP positions set to 12%. This model demonstrates rapid bottleneck resolution for both CAP and C–L terms within 5 years.
Several positions are jointly accredited for Stage 2 and Stage 3 CAP/C–L. Limiting the access to Stage 2-accredited CAP terms to only Stage 2 trainees results in a resolution of the bottleneck relating to CAP position availability within 3 years (Figure 3, scenario 2). However, under this scenario, the bottleneck relating to C–L position availability will not be resolved within 10 years.
The bottleneck resolution can be accelerated by a short-term reduction in the trainee intake. Scenario 3 (Figure 3) demonstrates a reduction in annual intake of 50% (i.e. from ~70 to ~35 trainees) for a period of 1 year prior to return to the ‘optimal intake’. This approach results in a stable position for C–L and delays worsening of the CAP oversupply, though not permanently. Additional gains in the bottleneck resolution are achievable by additionally limiting the AT occupancy of Stage 2-accredited positions to 12% (from the current 23%). This additional step achieves a resolution of Stage 2 bottleneck within 5 years.
Discussion
The modelling process demonstrates the presence of a training bottleneck in Queensland and the importance of assertive action to address this. Small incremental increases in trainee numbers in excess of position availability can have dramatic compounding effects on the number of trainees who will be affected by the bottleneck. Short-to-medium term restriction of new trainee intake below the ‘optimal intake’ offers a means to accelerate the resolution of the existing bottleneck; but in the longer term, addressing this issue from a Branch Training Committee (BTC) perspective is not as simple as introducing a cap on the entry of new trainees based solely on the availability of the Stage 2 mandatory terms. Active consideration of the impact of increasing entry into AT certificate programmes is also required.
Solutions to training bottlenecks outside of the direct control of the BTC should also be considered. These include advocating for short-term funding of additional training capacity and adapting existing positions to meet the CAP/C–L accreditation requirements. These measures would limit the extent and duration of the existing bottleneck, and if permanent funding was available, it would ultimately allow for growth in future training intakes.
Regular review of the training landscape is needed to manage ongoing bottleneck risks and balance workforce needs and distribution. Such reviews will also require input from individual services about their ability to accommodate new trainees or ATs to ensure a balance of supply and demand for training positions. It may not be practical to anticipate all factors affecting the system (e.g. withdrawals and Breaks in Training), so a conservative approach with some underutilisation of positions could increase flexibility and prevent stress within the system.
These findings raise important questions relevant to psychiatry training and workforce development in Australia and New Zealand. Workforce projections have demonstrated an increasing need for psychiatrists and child and adolescent psychiatrists in particular. 8 Concerningly, this modelling exercise demonstrates that there can be far-reaching impacts from increasing AT intake that could compromise overall trainee progression.
The current training environment and service demand needs may be in conflict. Services may make efforts to attract trainees in order to meet workplace demand or to ensure employee retention. These strategies are rational attempts to build service capacity that may have unintended consequences for the overall workforce and a detrimental impact on trainees. There is clear need for strong advocacy and funding to match any policy push for increased psychiatrists with increased funding for mandatory training experiences.
Footnotes
Acknowledgements
The collection of data in support of this project was facilitated by the administrative staff of the Post-Graduate Training (PGT) Psychiatry Office. Feedback on the modelling process and outcomes was provided by the members of the Queensland Branch Training Committee and other key stakeholders.
Disclosure
The authors report no conflict of interest. The authors alone are responsible for the content and writing of the paper.