
Abstract
Objectives:
We compared the quality of the written informed consent forms for electroconvulsive therapy (ECT) in Australian jurisdictions.
Method:
For this comparative audit-type study, a checklist was developed to compare informed consent forms from different jurisdictions. The main information sources for consent forms were government health department websites and Google. The directors of clinical services were contacted if a consent form was not available through a web source.
Results:
Majority of the informed consent forms covered information about ECT, general anaesthesia and alternative treatments, supports available for decision making, and a reference to the right to withdraw consent. Missing information affected information areas such as likely outcome if no ECT, lack of guaranteed response and cultural and linguistic supports.
Conclusions:
A standardised consent form that can be used across all jurisdictions can help improve the ECT practice.
Obtaining consent for electroconvulsive therapy (ECT) has a long history. 1 Providing adequate information about the procedure and alternatives and presence of decision-making capacity are important in relation to informed consent. 1 A variation in the consent for ECT was reported previously. 2 In a survey of ECT practice in Canada, two questions received low scores compared to other items, and these questions were about information about alternative treatments and information that there was no guaranteed improvement with ECT. 3
An informed consent is a national standard for any medical treatment or procedure. 4 Every Australian jurisdiction has their own legal framework and consent form for obtaining informed consent for ECT. Given that the indications for and administration of ECT are based on an evidence-based and standardised approach, we wanted to explore the quality of the written informed consent forms for ECT in different Australian jurisdictions. If a written consent form has both voluntary and compulsory sections, we included section about the general information about ECT and voluntary consent section.
Methodology
This cross-sectional study included the written informed consent forms for ECT from different Australian jurisdictions – Australian Capital Territory (ACT), New South Wales (NSW), Northern Territory (NT), South Australia (SA), Tasmania (TAS), Queensland (QLD), Victoria (VIC) and Western Australia (WA). The main source for the consent forms were the government health department websites and Google. We also contacted the clinical directors of jurisdictions if a form was not available through web sources. Data was collected between 1 and 30 November 2020.
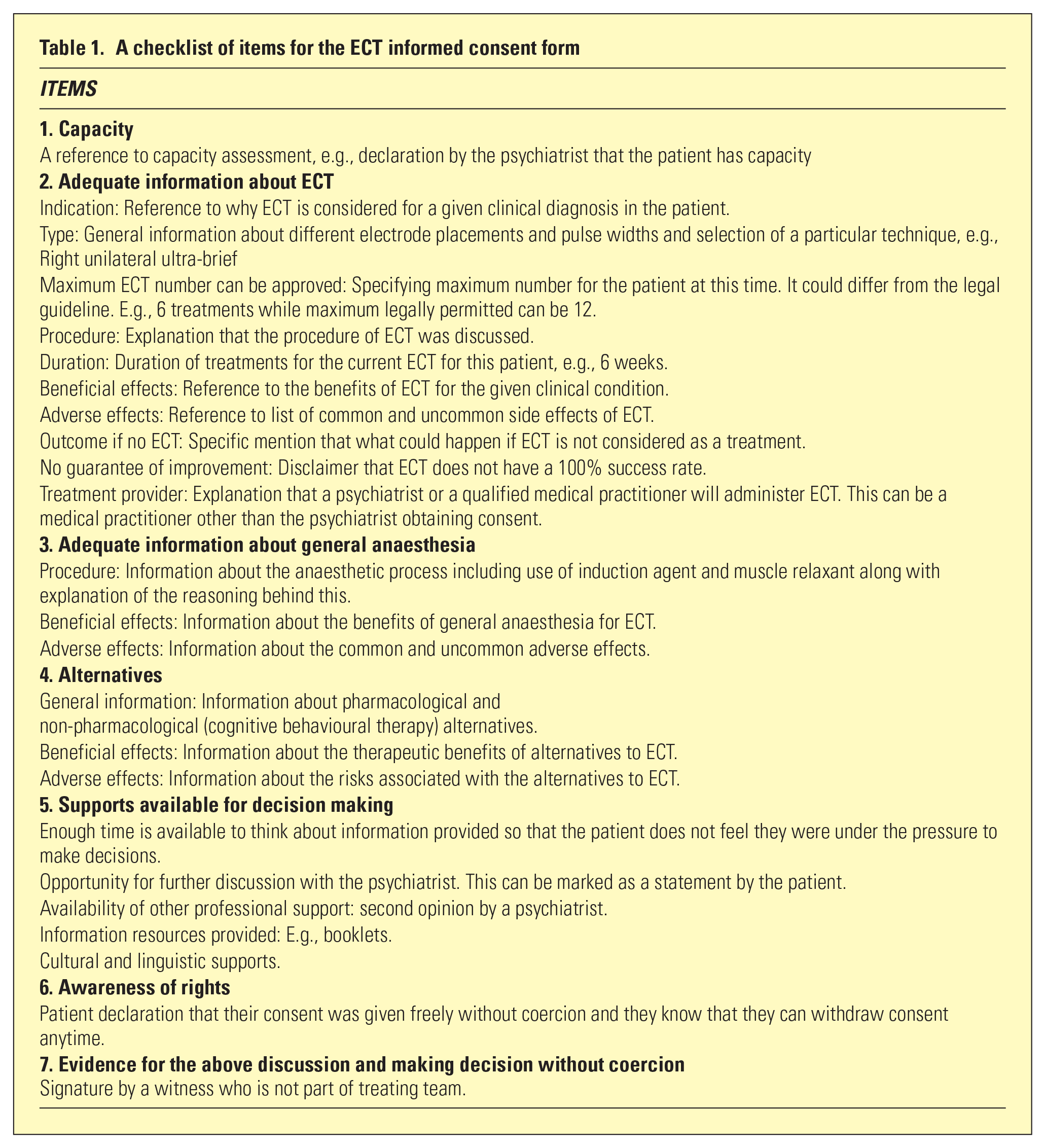
For this audit-type study, a checklist (Table 1) was developed using certain key references – Mankad, 1 Chan et al., 3 the Victorian Mental Health Act 2014 (MHA 2014) (Part 5, Sections 68–71), 5 Weiss et al., 6 and the Royal College of Anaesthetists guideline. 7 Two authors (KJ and FW) independently extracted information from the consent forms on the checklist and any discrepancy was sorted through discussion. This study did not involve any consumers or clinical records and hence ethics approval was not sought. Keeping in line with the nature of this study, findings were only summarised in descriptive terms.
A checklist of items for the ECT informed consent form
Results
Written consent forms were available for all jurisdictions. Each jurisdiction had one consent form except Tasmania that has two forms for different regions. There was a reference to capacity in some consent forms (SA, TAS, QLD and VIC). In relation to information about ECT, the indication, the nature of procedure and the maximum number of treatments were mentioned in all forms. Some forms did not specify the duration of ECT treatment, beneficial and adverse effects, type of ECT, outcome if no ECT and no guarantee of improvement.
About GA, the beneficial and adverse effects were mentioned in the most forms. However, there was no mention of beneficial effects in two forms (SA and TAS) and no information about adverse effects in one form (SA). For alternative treatments, a reference to beneficial and adverse effects was only available in a few forms (NT, QLD and VIC) (Table 2).
Comparison of informed consent in relation to ECT number and duration
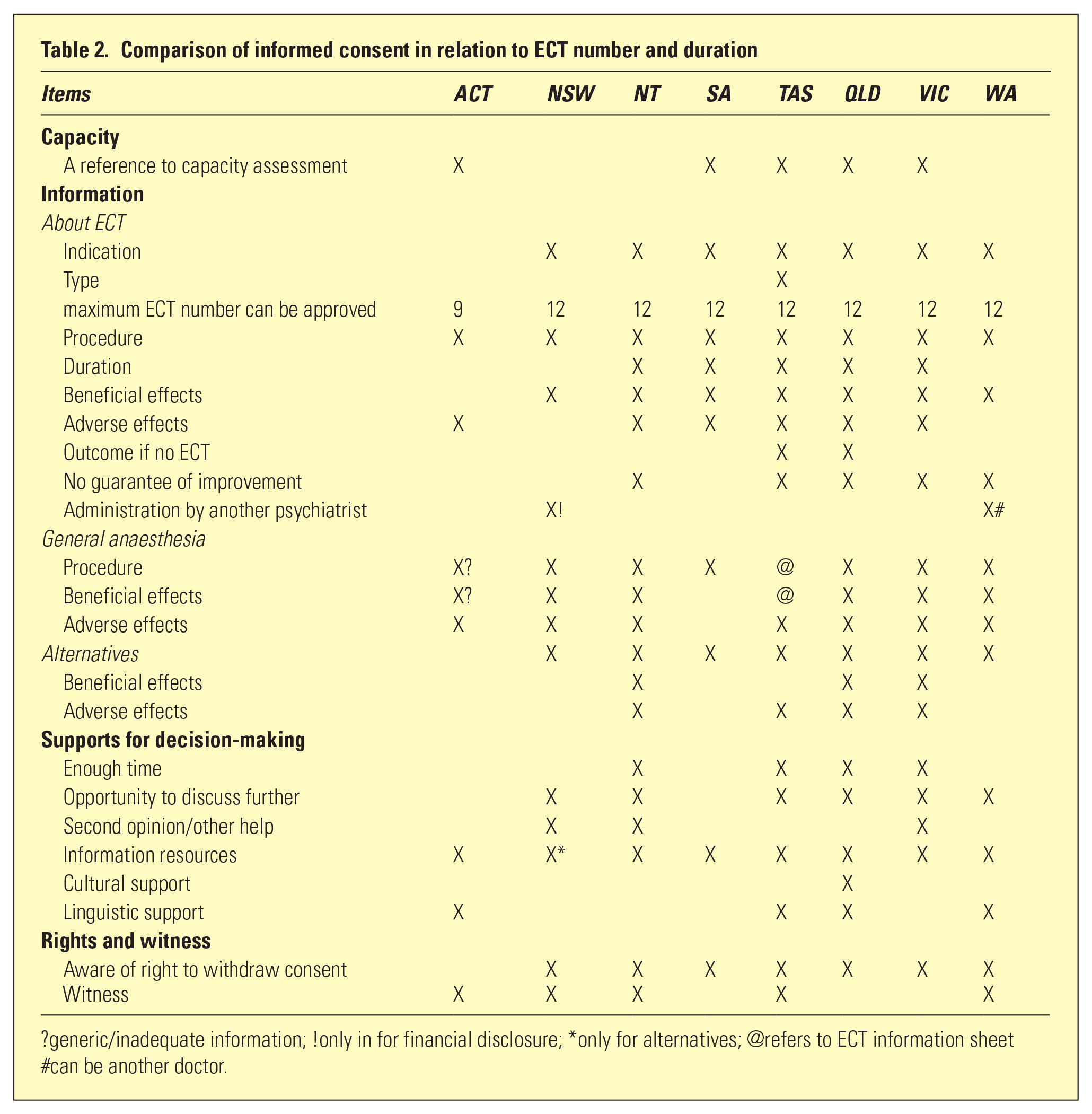
?generic/inadequate information; !only in for financial disclosure; *only for alternatives; @refers to ECT information sheet #can be another doctor.
In terms of supports for decision making, there was a statement about availability/provision of the ECT-related information in all forms. Missing information was noted in all other areas. Rights to withdraw consent was mentioned in almost all forms. Signature by a witness was needed in five consent forms (Table 2).
We also noted following additional information, that is, a statement that ECT can be administered by a medical practitioner other than the consenting psychiatrist (NSW and WA), a separate reference and additional information about GA (TAS, QLD and WA), consent for blood tests if there was needle stick injury and acknowledgement of increased risk of side effects due to pre-existing medical conditions (WA).
Discussion
This study compared the quality of written consent forms for ECT in various Australian jurisdictions. We found these consent forms were mostly comparable in their quality except in certain areas.
Only in about two-thirds of consent forms, we found a reference made about the capacity to make an informed consent. It is possible that differences in the legal frameworks governing ECT consent and the clinical practice of documenting discussions about capacity assessment in the medical records of consumers being considered for ECT could account for this discrepancy. However, given the significance of decision making capacity in relation to ECT treatment, it will be a good practice to include a comment about capacity in any informed consent form.
Largely, all written consent forms included items about various aspects of ECT and GA but inadequacy or lack of information was also evident in certain areas. These include information about the advantages and disadvantages of ECT, what would happen if the person does not receive ECT, and a disclaimer that ECT has no guarantee for clinical improvement. Only one jurisdiction made a reference to a separate GA consent form. The need for a separate consent for anaesthesia in relation to surgical consent was argued before.8,9 In the Czech Republic, consent forms for ECT and anaesthesia are separate. 10 Because modified ECT is the standard in Australian jurisdictions, a separate consent form for GA can appear redundant but sufficient information about GA should be included in any informed ECT consent form.
We noted that alternative treatments were often referred in a generic way. This needs improvement. For example, the written consent form from the John Hopkins University includes information about medications and psychological therapy and their advantages and disadvantages. 11
We found that there were clear statements about opportunity to ask questions and discuss ECT further, provision of information resources and the right to withdraw consent. However, we noted missing information in relation to linguistic and/or cultural support, witness section and availability of enough time to think about the ECT treatment. Although we have included signature by a witness as a criterion, as it can improve the transparency of the process, it is possible that this can be perceived to insinuate an underlying mistrust between the psychiatrists and consumers.
There are two main implications of our findings given the variations in the laws governing ECT.12,13 First, a comprehensive and standardised ECT consent form will align consenting process with other aspects of the ECT practice and GA that follow a standard protocol. In a larger perspective, the principles, procedures and legal frameworks for ECT needs to be comparable in different legislations and this would necessitate input from professions involved (psychiatry, anaesthetics, ECT nursing, administrators), consumers, carers, legal and ethics experts, crossing all states and territories. Secondly, the consent forms need to include clear information about alternative treatments. Additionally, inclusion of a potential list of cognitive side effects, which is partly covered in the consent form of QLD, can help to improve transparency and engagement associated with ECT process. Items in our checklist can help develop a comprehensive written informed consent form for ECT but considerations should also be given to the language and length of a written consent form (e.g., one page might not cover all the information whereas multiple pages can be cognitively demanding). Feedbacks from consumers and carers can help in optimising a written consent form. Overall, there is a need to balance person-centred care, clinical governance and medico-legal safety.
In conclusion, although there are limitations to any audit type studies, our findings shows that the written ECT consent forms are mostly comparable in their content across Australian jurisdictions. Further research is needed on this topic by including private sector and other countries. Another area to explore is how often consumers receive a copy of the signed informed consent form. A consent form is not a replacement for clinical assessment and documentation by psychiatrists, but a comprehensive ECT consent form can aid consumers to revise ECT-related information during the course of treatment. Also, a consistent and standard approach can improve the practice of ECT.
Footnotes
Acknowledgements
The authors thank the Chief Psychiatrist of Australian Capital Territory and Tasmania for their generous support in making the consent form available for our study.
Disclosure
The authors report no conflict of interest. The authors alone are responsible for the content and writing of the paper.
Financial disclosures
None to be declared.