
Abstract
Objective
With increasing levels of cultural diversity, it is important that mental health services are relevant and accessible to new migrant populations. Efforts have been made to bring attention to the unique experiences and needs of culturally and linguistically diverse (CALD) sub-groups in clinical settings, resulting in various frameworks and professional development workshops. While some of these strategies have raised awareness and persuaded service providers to accommodate different populations, few are effective and genuinely impact consumer outcomes.
Conclusion
This paper proposes an integrated cross-cultural assessment framework comprising both clinical and organisational components to improve cross-cultural clinical encounters and consumer satisfaction. The framework underscores the importance of the therapeutic alliance through the building of rapport and trust. Moreover, the framework is designed to be organisationally feasible, and locally and practically oriented.
Increasing diversity in many Western nations necessitates clinical services that respond to the needs of a multi-cultural demographic. A number of cross-cultural frameworks and philosophies (i.e. Cultural Safety and Cultural Awareness) have been developed to equip healthcare professionals with a better capacity to understand and serve their patients and to also reduce broader healthcare inequities. Many of these approaches, however, face practical challenges, and their direct impact on health care outcomes is still unclear. One challenge is that the extent to which cultural factors and experiences are implicated in a client’s mental health concerns or behaviours vary considerably. As such, working effectively cross-culturally demands an appreciation for the heterogeneity of culturally and linguistically diverse (CALD) populations, the notable overlap between the CALD and non-CALD experience, and the individual idiosyncrasies of each CALD client. Accordingly, the following framework for working cross-culturally in clinical settings is volunteered.
A framework for working cross-culturally
The overarching aims of the framework, which can be incorporated into any clinical assessment and service at large, are to (i) improve conditions for client engagement, (ii) identify the extent to which cultural factors are present and relevant to the assessment, and (iii) identify and attenuate organisational impediments to effective cross-cultural service delivery. The proposed integrated cross-cultural framework comprises five components – three dynamic interactional stages for the clinical encounter and two that are pertinent to the broader organisation.
Clinical components
Relational
Mastering the nuances of the myriad cultural backgrounds of consumers is unachievable.1,2 Therapeutic breakdowns with CALD consumers are caused by more than just a clinical unfamiliarity with cultural norms and practices. Moreover, a consumer’s capacity to meaningfully participate in a clinical encounter rests beyond mere cultural traditions. It will reflect their unique experiential reality, their prior interactions and personal perceptions of these dynamics. Clinicians are better served employing generic traits such as open-mindedness, good listening skills, patience, flexibility, a warm verbal communication style, an empathetic posture and non-judgement. 2 This engenders an environment where a consumer will feel more comfortable sharing and educating the clinician on (cultural) issues they deem relevant to the interaction without clinical presumption.
The inability to develop rapport is a regular concern noted by CALD individuals when describing their disinclination to utilise mainstream clinical services. 3 The requirement for a robust and durable rapport is especially important when assessing or treating CALD consumers for several reasons. First, CALD consumers may feel some level of social rejection and perception of differential treatment by mainstream society and its institutions. This may stem from previous negative/discriminatory interactions in the community or other internalised stigmas. If such dynamics are not well understood by a clinician, the consumer may perceive the clinical process to be an extension of the exclusion they already experience in society. Second, for many CALD individuals, expectations of stoicism within families are prioritised, with sometimes little modelling on how to openly discuss emotions. These family dynamics can be transferred into clinical settings. Moreover, cultural stigmas about mental health may deter CALD consumers from willingly seeking assistance for mental health concerns or adhering to treatment schedules.
To minimise the non-disclosure of information and avoid triggering distress, a relational disposition and a commitment to rapport building is recommended.3,4 This process may take longer for CALD consumers, many of whom will be reluctant to divulge information they may consider to be private or shameful. Pushing for early disclosure of past traumas or intimate family dynamics ahead of current needs is a barrier to engagement. A trusted, safe and respected interlocutor is of greater importance than merely being of the same cultural background or understanding obscure cultural facts about particular groups. It is also prudent to avoid particular behaviours (i.e. patronising body language, superior/condescending tones and premature intrusiveness) that may quickly induce feelings of social rejection among CALD consumers who may be sensitive to subtle, non-verbal cues. The purpose of being relational is to provide a trusted secure space and to be keenly aware of how clinical behaviours can influence consumer engagement.
Cultural
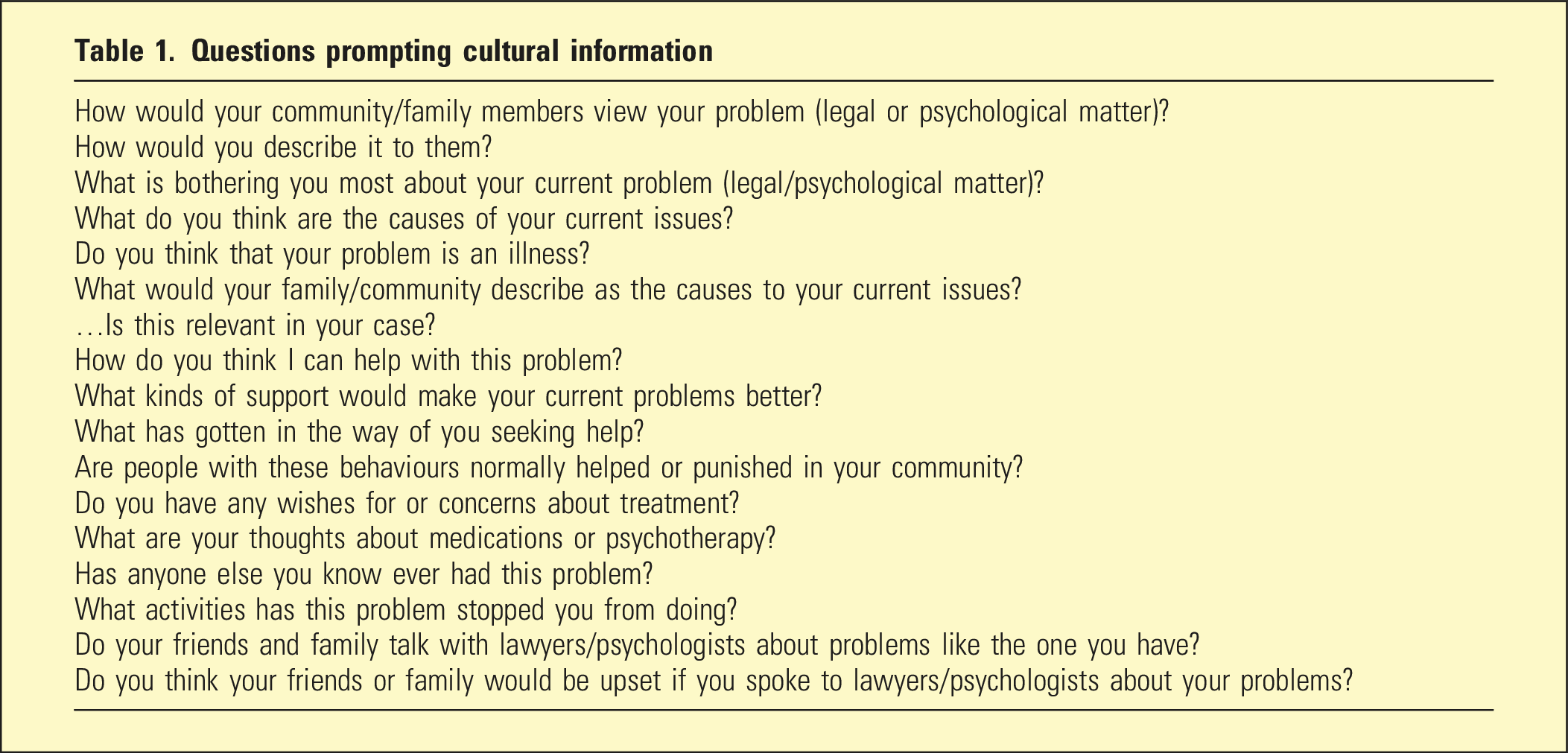
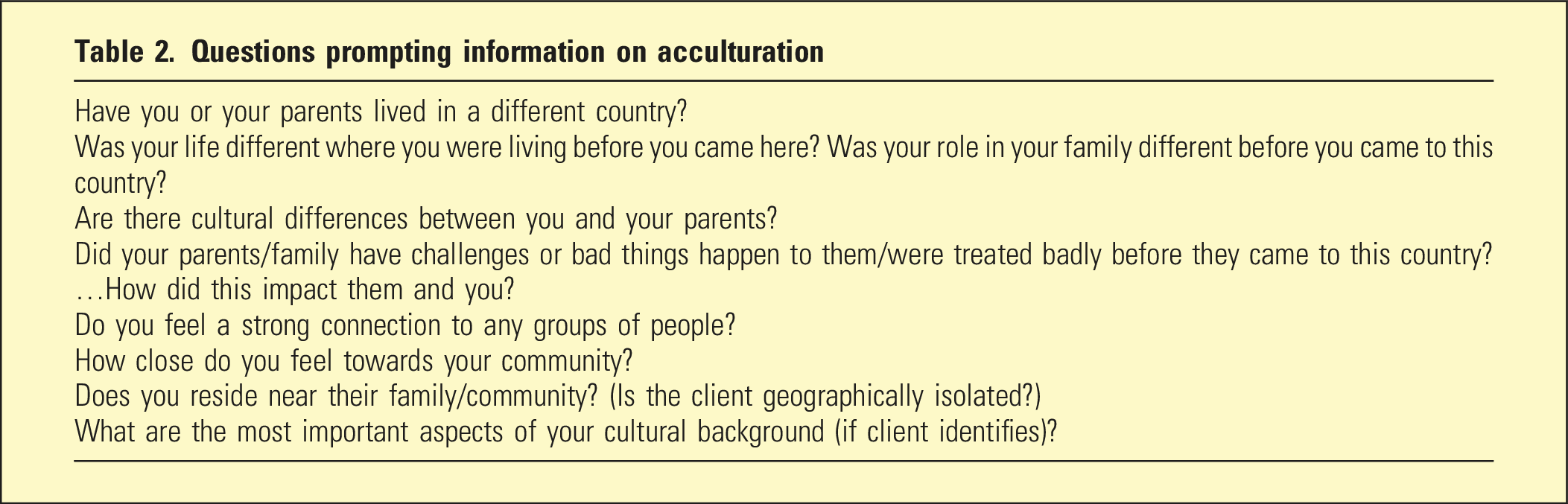
This component helps to identify the extent to which culture-related issues may be implicated in behaviour and discerning available support networks. Extracting cultural information should be an organic and subtle exercise. Once relational efforts have been made to engender a trusted dynamic, careful lines of questioning can be employed. The DSM-5 Cultural Formulation Interview 5 (and forensic iterations 6 ) and other resources7–9 provide a list of questions that gently probe cultural motivations and rationalisations for behaviours. Introduced in 2013, The DSM-5 Cultural Formulation Interview was designed to help clinicians in all mental health care settings better understand their patient’s cultural experience of illness and help-seeking behaviours. 5
Questions prompting cultural information
Questions prompting information on acculturation
Questions on culture and social challenges
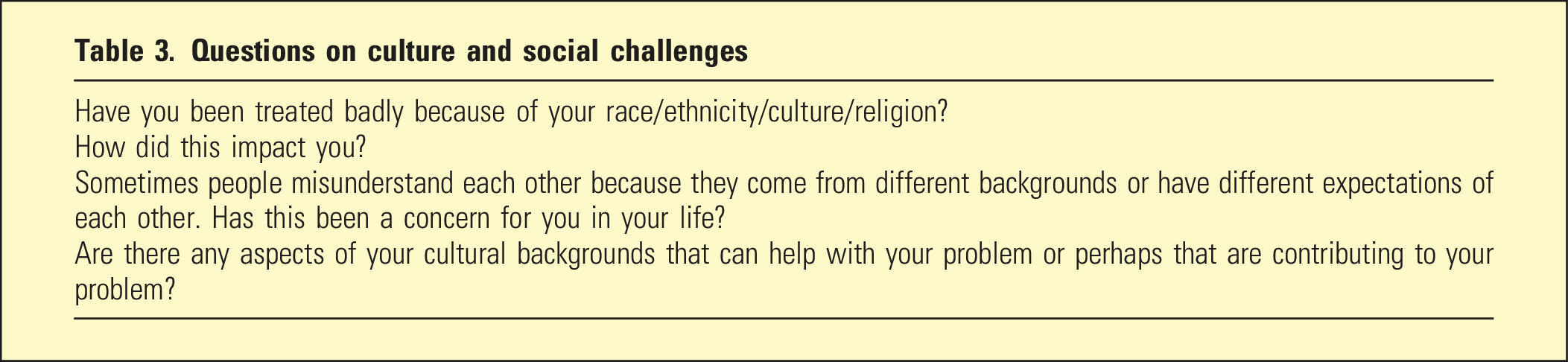
The tables are not exhaustive lists, and further information can be obtained from the original sources. Moreover, one must be judicious with the order and timing of these questions. The explicit use of medicalised vocabulary may need to be tempered initially with some consumers to avoid cultural stigmas and negative connotations associated with these terms. Confidentiality must be explicitly assured for consumers who may be concerned that members of their family or community will discover their discreet utilisation of services. Clinicians must be clear about the information they will keep on record and under what circumstances they will be expected to break confidentiality.
Individual
Every consumer, regardless of their cultural heritage, possesses a unique intersectional profile which comprises various sub-cultures and identities and their own personal expression of these identities. The relevance of cultural information can be established by considering this information with regard to other facets of their life and social context. Where cultural reasons are believed to be implicated in various attitudes and behaviours, it is important to consider other plausible and more parsimonious explanations for the behaviour. This not only avoids inadvertently linking culture and problem behaviours, but it ensures that clinical decisions are informed by relevant data. For example, there are other personal attributes that should not necessarily be conflated with culture that will impact immediate behaviour including an individual’s age, gender, level of education, socio-economic status, cognitive ability, personality type and temperament. Moreover, individuals’ identities and attributes (or various combinations thereof) may activate, or engender, unique experiences under specific circumstances.
Organisational components
Institutional
An organisation must facilitate an environment in which the above three clinical components are enabled. Over-bureaucratised services can restrict this ability, limiting the capacity of clinicians to build relationships with CALD clientele. 10 Over-burdened, time-poor staff will face difficulties engendering trust under these circumstances. Errors in judgement, biases and shortcuts are more likely to manifest under these conditions. A CALD consumer may perceive an inflexible, administrative-heavy experience to be insensitive and impersonal, deterring them from further help-seeking.
There is already a perception among some CALD communities that mainstream services are transactional rather than relational. 11 It is important that consumers do not sense a culture of compliance, which encroaches on person-centred care. Again, initial capacious interactions are important – the presence of (cultural) liaison officers pre-assessment to assist with paperwork, address any confusion, vouch for the service, and de-stigmatise the experience may be useful. Consumers could perhaps have some input over the location of initial clinical interactions. Prior work has suggested that mainstream clinical services partner with smaller culture-based community organisations to alleviate some of these concerns. 12 Such services are often in close proximity to their communities, possess unique insights into the needs of their constituents and their families, and engage in regular outreach. Last, some programmes may need to be re-named to avoid cultural stigmas if they contain explicit references to mental illness.
Educational
Services, with permission, should collect localised data on the different sub-groups that utilise the service to ascertain the presence of non-mainstream factors, behaviours and presentations. Collecting consumer data may be useful in informing practice and can also be juxtaposed with the demographics of the local catchment area to identify which groups may be under-utilising the service.
Drawing on the practical expertise of clinical staff with cultural knowledge and other practitioners from CALD communities may assist others in the organisation to navigate cross-cultural interactions. These individuals can often provide more focused practical advice and can frame their recommendations within organisational frameworks. Undertaking supervision in multi-cultural clinical settings from a clinician with practical cross-cultural knowledge is probably the strongest form of cross-cultural education. Services may benefit from identifying these resources already within their ranks or local community (i.e. staff or community outreach workers who possess specialised cross-cultural skills and intimate knowledge about particular cultures) rather than seek advice from external generic trainers and consultants.
A service provider may also benefit from the development of working groups to discuss practical cross-cultural issues. The group would engage in practically oriented troubleshooting and open discussions where staff members could air their experiences, challenges and solutions to cross-cultural clinical encounters. Ideally, the working group would be a forum where staff members can share concerns without judgement and receive mentoring and advice from other colleagues in a relaxed supportive space. Here, staff could also produce a body of knowledge that may be useful for other staff members.
Conclusion
With increasing levels of cultural diversity, it is important that mental health services are relevant, useful and accessible to new populations. This paper proposed an integrated cross-cultural assessment framework, comprising both clinical and organisational components, to improve cross-cultural assessment and consumer satisfaction. The framework underscores the importance of the therapeutic alliance through the building of rapport and trust. Moreover, the framework is designed to be organisationally feasible, and locally and practically oriented. It is recommended that all aspects of the proposed framework are rigorously evaluated.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.