
Abstract
Insomnia remains one of the most common sleep disorders experienced by the geriatric population. Treatment for older adults with insomnia begins with nonpharmacological interventions. The recommended initial intervention involves behavioral or cognitive behavioral therapy strategies geared toward older adults.
Cognitive behavioral therapy for insomnia (CBT-I) is widely used in clinical practice to improve sleep quality as a nonpharmacological treatment. A regulated CBT-I approach contains five core components, including sleep hygiene, stimulus control, relaxation training, sleep restriction, and cognitive restructuring (1). Although many meta-analyses have examined the effects of CBT-I on insomnia among the general population, only one study reported the efficacy for the treatment of insomnia in older adults (2). During the study period, many original studies were conducted on CBT-I in older adults with insomnia. Therefore, we aimed to assess the efficacy of CBT-I for the treatment of insomnia in older adults.
Methods
The protocol of this meta-analysis has been registered in PROSPERO. The present report followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. (Supplementary Table S1)
Search strategy
We systematically searched six databases from database inception until June 12th, 2021. The search was last updated on January 30th, 2022. Search strategies were customized for each database and included medical subject headings (MeSH) and text terms. There were no restrictions on language, publication year, or publication type.
Inclusion and exclusion criteria
Studies were included if they met the following criteria, established by using the PICOS strategy. We only included RCTs. (Supplementary Table S2)
Study selection
The study selection process was conducted by two researchers. After excluding duplicates, the researchers used the inclusion criteria to screen the study titles and abstracts to identify potentially eligible studies. The full texts were obtained and reviewed again for final inclusion. Any differences between the two reviewers were resolved through discussion with a third reviewer.
Data extraction
Quantitative data were extracted from the included studies by one reviewer and then cross-checked for completeness and accuracy by two reviewers. We used a standardized form to extract the following information from all included articles: publication year, insomnia definition used, age of the participants, treatment format (individual and group), control group (e.g., waitlist and sleep hygiene), and type of intervention. We contacted the article authors via email (with a maximum of three attempts) for missing information, but unfortunately, we did not receive any responses.
Quality evaluation
The Risk of Bias 2 (RoB 2) tool was used to assess the methodological quality of the included studies. Five domains were assessed, including the randomization process, deviations from the intended interventions, missing outcome data, measurement of the outcome, and selection of the reported results. Each item was rated as having “low risk,” “high risk,” or “some concerns.” Two reviewers independently performed the assessment.
Statistical analysis
The MD (Cohen’s d) was used to calculate differences in continuous variables between the intervention and control groups. We used inverse-variance methods to combine continuous data for the meta-analysis. Cochran’s Q statistic was used to evaluate the heterogeneity among studies, and heterogeneity was considered to be present when p < 0.05. The level of heterogeneity was measured by the I-square (I 2 ) statistic. I 2 values of 25%, 50%, and 75% were, respectively, considered low, medium, and high heterogeneity. If heterogeneity existed, a random-effects model was used to calculate the weighted effect size to accommodate the heterogeneity in the study. Otherwise, a fixed effects model was used. Sensitivity and subgroup analyses were performed to explore potential sources of heterogeneity. Funnel plots were used to analyze publication bias. All statistical analyses were performed with RevMan 5.3 (The Nordic Cochrane Centre, the Cochrane Collaboration, Copenhagen, Denmark) and Stata 16.0 (StataCorp LLC, College Station, TX, USA).
Results
Study selection
In total, 496 records were identified by searching six databases, and 287 potentially eligible articles were identified after removing duplicates. Forty studies were retrieved and reviewed by a more detailed assessment after screening the titles and abstracts. After reviewing the full-text articles for eligibility, 13 articles were included. (Figure 1, Supplementary Text S1 and Supplementary Text S2) Flow diagram of the search for and selection of the included studies.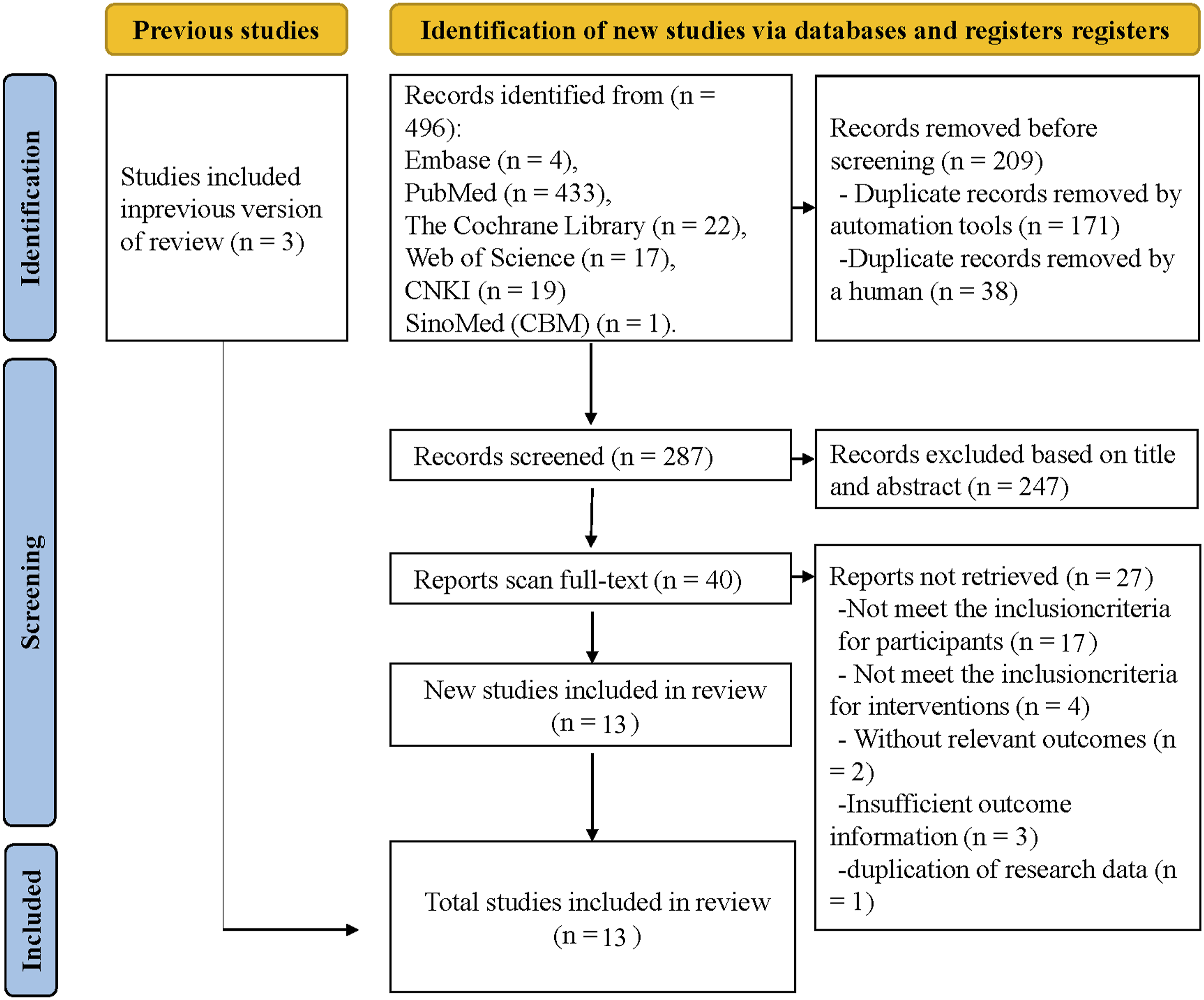
Characteristics of the included studies
Characteristics of the studies included in the meta-analysis
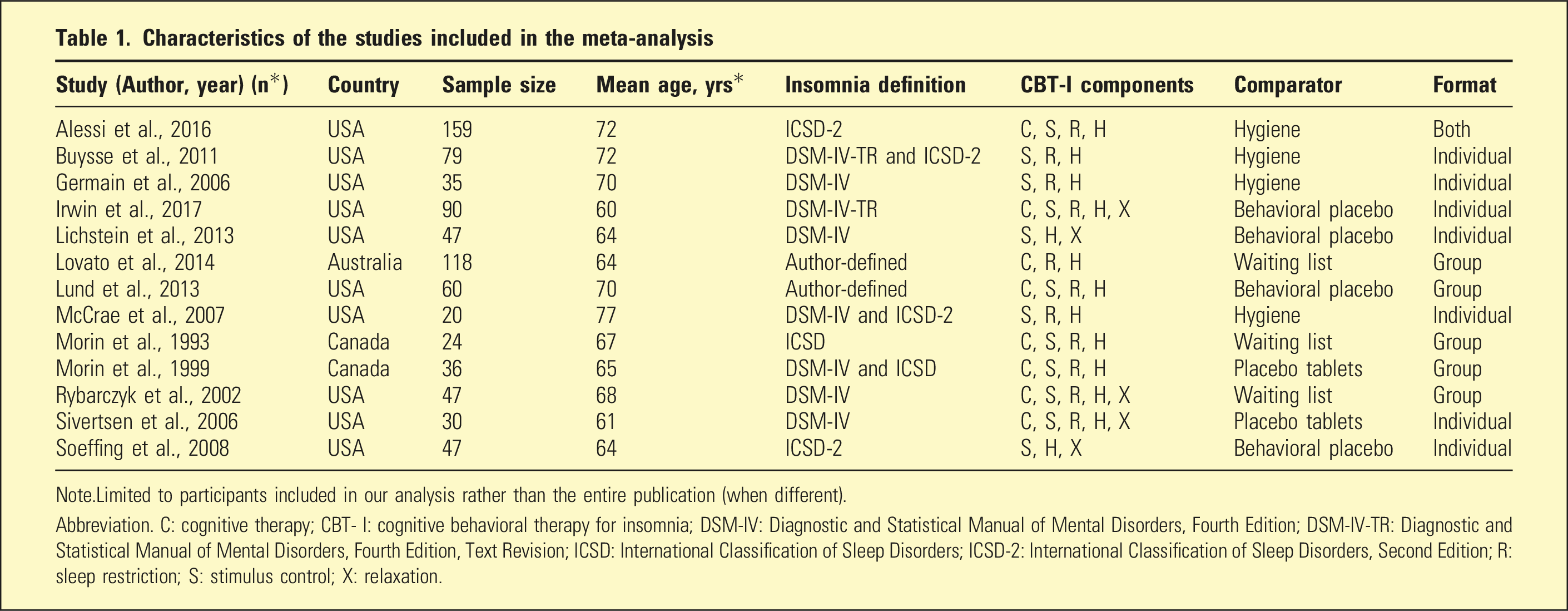
Note.Limited to participants included in our analysis rather than the entire publication (when different).
Abbreviation. C: cognitive therapy; CBT- I: cognitive behavioral therapy for insomnia; DSM-IV: Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition; DSM-IV-TR: Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision; ICSD: International Classification of Sleep Disorders; ICSD-2: International Classification of Sleep Disorders, Second Edition; R: sleep restriction; S: stimulus control; X: relaxation.
Quality evaluation
Seven studies mentioned the methods of randomization, including automated computer-generated random number tables (3–5) and random sequence blocks managed by a spreadsheet program (6–9). Six studies mentioned randomization but did not mention how the authors executed randomization (10–15). Four articles mentioned concealed allocation, including sealed envelopes (4, 9) and numbered boxes (3, 7). Ultimately, 4 articles were rated as low risk and 9 were rated as some concern.
In terms of deviating from the intended intervention, eight studies used a blind method, including single blindness (n = 5) and double blindness (n = 3). Finally, 5 articles were rated as some concern, and 8 were rated as low risk. All studies were assessed as low risk in terms of the missing outcome data, measurement of results, and selective reporting of results. Finally, 9 studies were assessed as some concerns, and 4 were assessed as low risk. (Figure 2 and Supplementary Fig. S1) Risk-of-bias distribution across studies.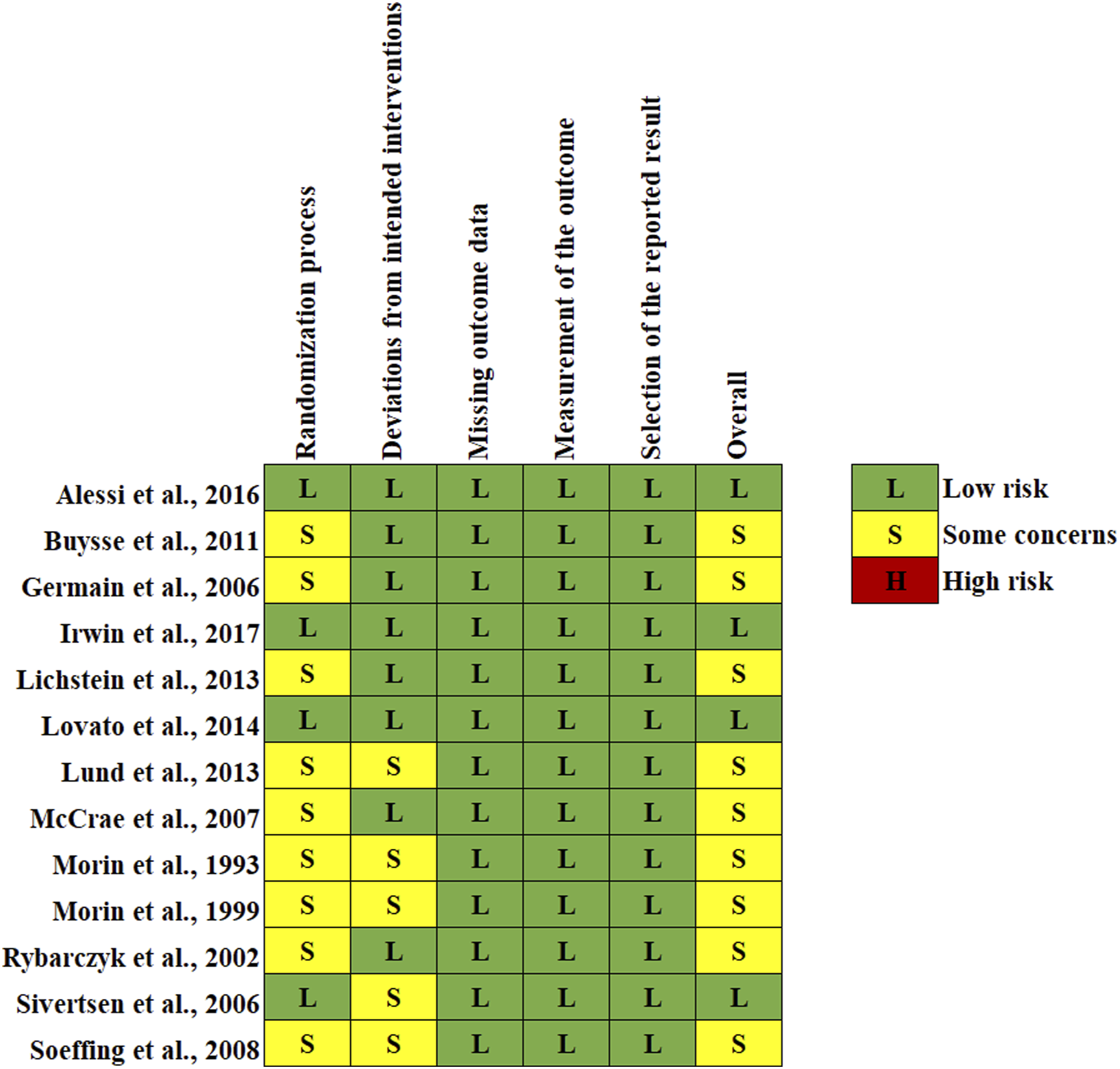
Synthesis of results
Based on the results from the sleep logs, a significant pooled effect size was observed for sleep efficiency (SE%) (MD = 8.36; 95% CI, 5.96–10.76; I
2
= 77%; p < 0.00001), sleep onset latency (SOL) (MD = −9.29; 95% CI, −13.62 to −4.96; I
2
= 64%; p < 0.0001), wake after sleep onset (WASO) (MD = −23.44; 95% CI, −32.41 to −14.47; I
2
= 85%; p < 0.00001), and total sleep time (TST) (MD = −12.35; 95% CI, −21.27 to −3.42; I
2
= 63%; p = 0.007). The heterogeneity of all the results was medium to high significantly. (Figure 3) Effects of CBT-I in older adults with insomnia.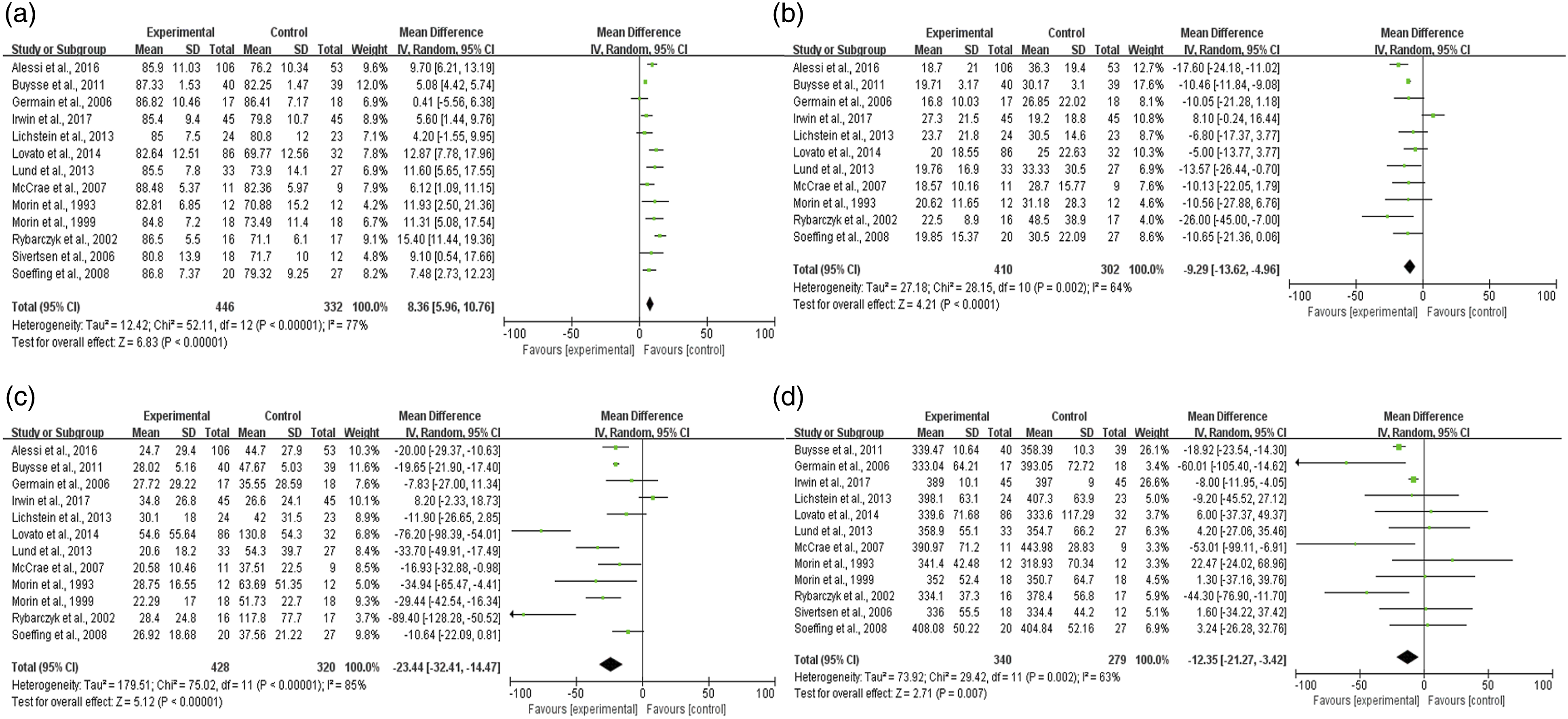
Publication bias and sensitivity analysis
A visual inspection of funnel plots revealed no publication bias among the included studies. (Supplementary Fig. S2)
Sensitivity analysis was performed to evaluate the effects of the individual studies on the pooled estimates. (Supplementary Table S3 and Supplementary Fig. S3)
Subgroup analysis
We conducted subgroup analyses by the models and forms of CBT-I to determine the source of heterogeneity. (Supplementary Table S4 and Figure S3)
Discussion
Summary and interpretation
Insomnia is a common public health problem, which is related to mental disorders, comorbidities, functional defects, and other diseases (16, 17), leading to a decline in patients’ quality of life. Our meta-analysis not only verified the impact of CBT-I on insomnia but also further explored which intervention characteristics contributed to greater impact.
Our results found that CBT-I was effective in improving insomnia in older adults in sleep diary outcomes, with significant improvements in SE%, SOL, WASO and TST. The TST outcome may be that sleep restriction directs patients to reduce time in bed to improve SE% and may also be influenced by sleep relaxation to increase sleep time. Differences in the specific style of CBT-I intervention, the level of quality supervision, and the delivery style of therapists may account for the moderate to high heterogeneity of outcomes.
We formulated strict inclusion criteria to minimize the heterogeneity and conducted subgroup analysis on SE% and SOL of the CBT-I model and form to further explore the sources of heterogeneity.
We found that the CBT-I models (whether it contained a cognitive restructuring component or not) may have been a reason for the heterogeneity and found that the treatment of insomnia was better in the CBT-I subgroup than in the BBT-I subgroup. We believe that cognitive therapy is important in CBT-I by improving the ability to prevent and weaken the recurrence of sleep disturbances. Future studies can focus more on the individual effects of the components of CBT-I intervention and compare their effects. Similarly, we found that the form of CBT-I was also a source of heterogeneity, and group intervention was more effective than individual intervention. We believe that group intervention can help patients achieve self-help and mutual assistance among those who have similar experiences or troubles and encourage patients to learn, supervise and encourage each other, which can improve compliance, promote functional recovery and strengthen therapeutic efficacy (18). Additionally, group intervention encourages patients to apply the learned methods to their daily life and interpersonal interactions, which is beneficial for patients to transfer their re-established behavioral and cognitive patterns into daily life, which may produce lasting therapeutic effects.
Limitations
However, there are some limitations. First, the quality of the studies included in this study varied, and publication bias cannot be ignored, which may affect the accuracy of the conclusions. Second, there was no follow-up analysis of the CBT-I interventions to determine long-term outcomes. Third, we only compared the effectiveness of the interventions without assessing the acceptability of and compliance with CBT-I, which will need to be supplemented by future mixed studies. Fourth, we only analyzed sleep diary results to assess insomnia, and future research should consider standardized procedures for insomnia diagnosis and comprehensive and objective assessments of sleep.
Implications
By demonstrating the effectiveness of CBT-I, we hope to further stimulate the family, society and healthcare system to better explore the potential value of this intervention in old people with insomnia. Furthermore, our findings may be used in future research to design more effective interventions and ultimately improve sleep quality. In the future, CBT-I interventions can be tailored considering the group and full CBT-I.
Conclusion
CBT-I is a safe and effective way to improve insomnia in older adults. However, due to study limitations, CBT-I needs further research and expansion in clinical application for middle-aged and elderly patients, and providing substantial evidence for well-designed multicenter clinical trials with more participants is urgent.
Supplemental Material
Supplemental Material - Efficacy of cognitive behavioral therapy for insomnia (CBT-I) in older adults with insomnia: A systematic review and meta-analysis
Supplemental Material for Efficacy of cognitive behavioral therapy for insomnia (CBT-I) in older adults with insomnia: A systematic review and meta-analysis by Kexin Huang, Su Li, Rendong He, Tangsheng Zhong, Haiqi Yang, Li Chen, Hui Gao, and Yong Jia in Australasian Psychiatry.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research supported by the Fundamental Research Funds for the Central Universities (415010300071), the Jilin Scientific and Technological Development Program (20210508003RQ), the Educational Commission of Jilin Province of China (JJKH20211152KJ), and the Jilin Association of Higher Education (JGJX2022B6).
Supplemental Material
Supplemental material for this article is available online.
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.