
Abstract
Objective
An inner-city hospital purchased a local hotel to provide support, digital engagement, skill development groups and referrals to partner agencies. Being aware of the hotel’s importance to the local community, we sought feedback on a model of care relevant to perceived gaps and needs in support for mental health.
Methods
Four online focus groups included healthcare professionals, nominated opinion leaders from local Non-Government Organisations (NGOs), consumers and carers to reflect a range of views. Focus group data were qualitatively analysed.
Results
Participants made useful suggestions about WHAT educational, preventative and therapeutic services were needed. They emphasised the importance of HOW people engage with the service, the balance between accessibility and security. Other themes included targeting people with limited health literacy, integration with existing services, building on site heritage and ongoing evaluation of objectives and needs.
Conclusions
This pilot study demonstrated clear support for providing safe and welcoming access to services, with resources and access to services to improve their health and wellbeing built on principles of social justice and inclusion. Participants had constructive ideas of what was needed, and ongoing patient and public research is anticipated.
The purchase of a landmark local pub, a well-loved ‘watering hole’ by an inner-city hospital, has given reality to the vision of an urban health hub providing a drop-in space, face-to-face support, digital engagement and groups for skills development, and referrals to partner agencies. The services aim to be innovative, inclusive, collaborative and accessible. We were well aware of the hotel’s special place in the heart of many locals and the importance of the premises providing services that are meaningful for the local community.
The HeathStreet model in Florida 1 provided an example of a service providing the local community with mental and physical health-related information, service navigation, work-related skills and recreation combined with ongoing research concerning the local community’s health needs. HealthStreet focusses on those with poor access and complex health needs.
We saw value in including community participatory research from the outset. A recent Australian study reviewing patient and public involvement (PPI) in the development, delivery and improvement of healthcare noted that involvement in how it is used has been under‐reported. 2 This pilot qualitative study is intended to be the start of ongoing engagement with the local community and service providers and consumers to allow an opportunity for engagement in service design and ensure a meaningful model of care relevant to local needs.
Method
Design
Focus group facilitator question guide
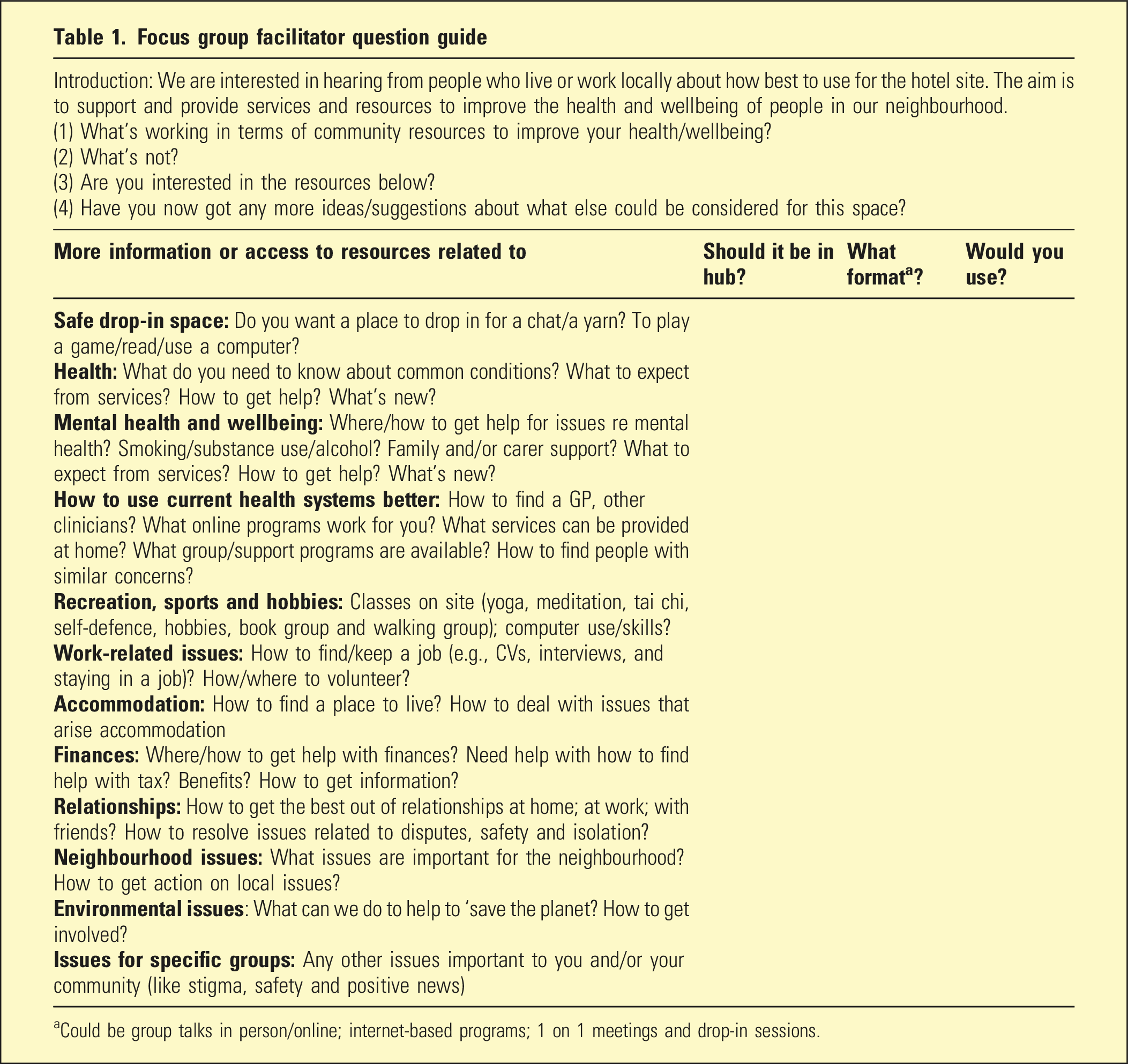
aCould be group talks in person/online; internet-based programs; 1 on 1 meetings and drop-in sessions.
Setting
Four focus groups were held online using Microsoft Teams (enabling recording of sessions and automatic transcription).
Procedure
After gaining ethics approval from the relevant hospital ethics committee, all participants gave informed consent prior to focus group participation. The groups were facilitated by two members of the research team. All groups were observed by the researcher responsible for the qualitative analysis. Each focus group lasted about 90 min. A donation enabled participants to receive a US $100 voucher in recognition of their time.
Participants
There were 33 participants, including consumers (N = 6), carers (N = 5), healthcare professionals (N = 12, comprising local GPs (N = 3), pharmacist (N = 2), clinicians from homeless, drug and alcohol and chronic care services, social work (N = 7) and community members (N = 10, representing local non-government organisations and community services that related to the hospital).
Data collection and analysis
Inductive thematic analysis was used to synthesise information obtained from focus group transcriptions from the 33 participants in the four groups. To improve rigour, purposive sampling, respondent validation and triangulation (data source, environmental and investigator) were conducted. 3
Results
Qualitative analysis produced themes concerning what and how services were offered and the uniqueness of the site, as described below. Participants’ quotes in italics are referenced by the participant group (clinician, consumer and community [member/carer]).
1. The WHAT: clarity around services
Participants prioritised a healthcare model that promotes and educates around health issues and provides a more day-to-day approach to health education (in contrast with acute hospital-based services).
They envisaged a hub, with access to information and services around common mental and physical health conditions; recreation, sports and hobbies (for socialising); and issues around work, finances and relationships. Other ideas included a small garden, access to computers (for information searching and access to online treatment programs) and spaces for private chat talks with peer workers and clinicians and groups (for therapy, education and recreation).
Participants discussed opportunities for work-skill development. They suggested using the bar for hospitality training, using computers to enable relevant work-related skills and inviting groups from various community services to provide guidance and advice.
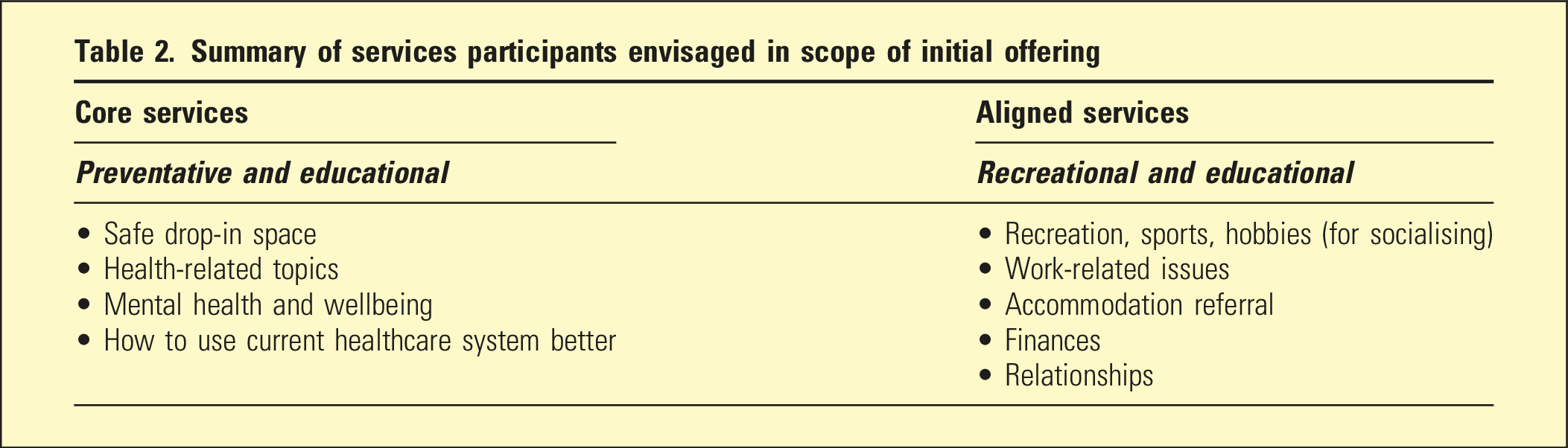
Participants emphasised the need for a safe, welcoming nonclinical space where one could find information related to health and wellbeing and potential referrals to clinical and community services. The suggested services were grouped into preventative, therapeutic and educational categories.
Preventative
accent on wellbeing and social inclusion, so that people felt welcome into a non-stigmatising space for socialisation, information and activities related to health promotion and wellbeing. They saw an opportunity in recreational offerings, but recommended more detailed examination of what is already on offer locally.
Therapeutic
initial triage, consultation and brief interventions with referrals to general practitioners, specialists and community services.
Educational
Summary of services participants envisaged in scope of initial offering
They recommended ‘starting small’, with ongoing community-based research about what was working and inform future directions. HealthStreet in the United States provides a model for this. 1
2. The HOW as important as the WHAT
Participants recognised hospital’s values of social justice and inclusion but felt it should be demonstrated in a less ‘clinical’ model.
You can have all of the expertise in the world inside your building, but unless people feel comfortable walking in the door, it’s completely useless [clinician].
You can go out, get a coffee, sit down on a couch and get yourself back into some sense of normalcy [community member].
Participants emphasised how the look and feel of the premises and staff communicate a sense of inclusivity and partnership in what they provide. They envisaged nonclinicians, such as peer workers, leading the engagement but noted the need for skills training, especially the frontline workers… This isn’t an acute services program, and there’s a need for a different set of skills in this [clinician].
As safe drop-in space, HOW people engage with the service was critical. It was seen as ‘not simply a place to go to when I have an issue…I can go to for another activity or experience (using a computer, gardening, social activities) and use that activity as a conduit to more direct engagement with services…[consumer]’.
I go in for a cup of tea, then can talk to someone about a health issue [consumer].
We all talked about, quiet zones, places for sitting by yourself, or with other people where it's quiet and secure…not too modern and slick [carer].
Participants expressed concern about safety for those experiencing trauma and the need for extended hours, with a 24-h call service. They acknowledged the paradoxes between safety and security needs, being informal and nonclinical but providing clinically informed information. Clinicians and consumers commented that they had seen security done well when the security guards have been happy and welcoming [consumer].
3. The HOW: retaining the uniqueness of the site
All groups recommended retaining the hotel’s heritage as a sociable place with a colourful local history. There was a strong appeal to reference the local area’s history, with photos and stories that delivered a sense of history and/or belonging to the space.
Such an ideal spot for a service like this…for that sort of outreach and making people feel safe…making this centre visible so people know what they can come there for, because the location is perfect. It…doesn't look like a hospital from an outside perspective. It's a very beautiful warm looking building [community member].
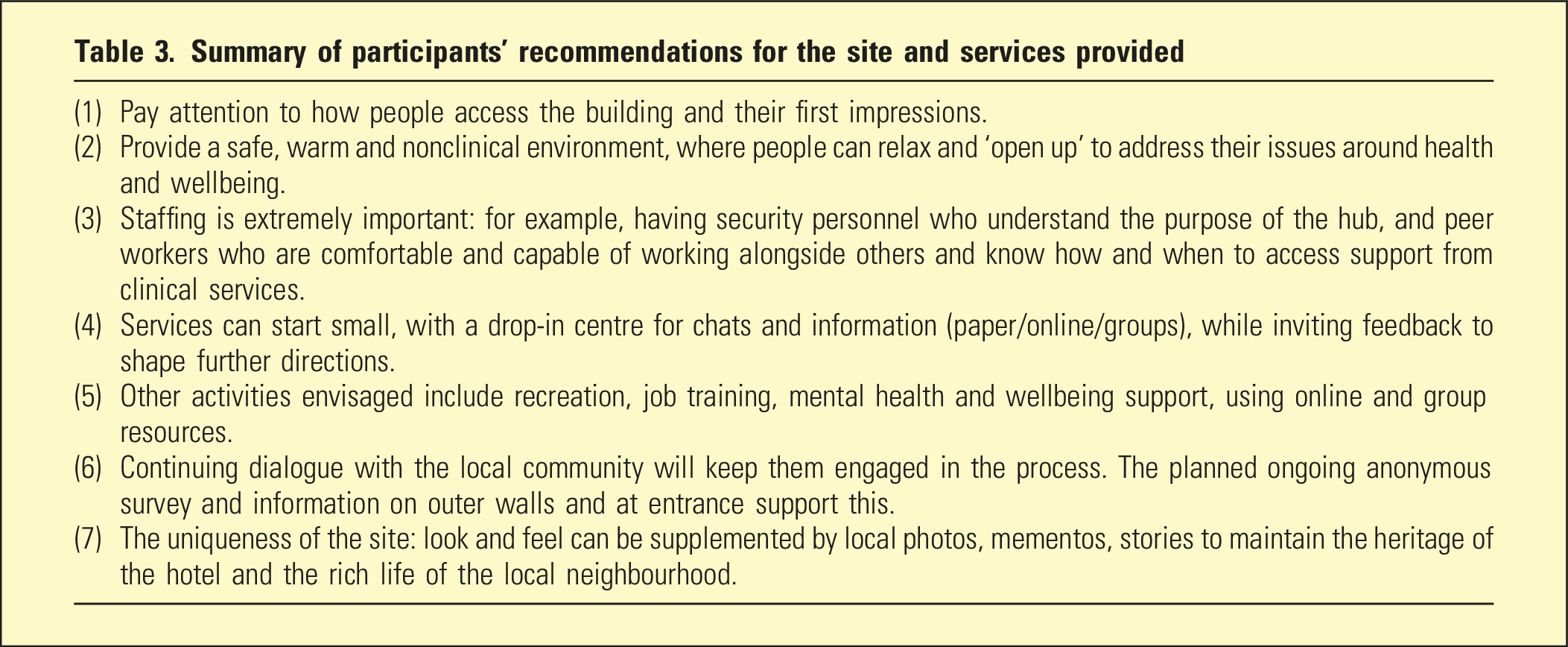
Summary of participants’ recommendations for the site and services provided
Discussion
Participants voiced clear support for the site providing access to resources and services to improve the health and wellbeing of those using the service. They reinforced the need to retain principles of social justice and inclusion that respected their previous experience of the hotel. They stressed the need for ongoing feedback from the community both during redevelopment of the site and when services are underway.
While the recommendations taken from the study pertained to the local site, the issues of providing welcoming community-based spaces that provide a sense of social inclusion and empower consumers and carers to be better-informed about their health and wellbeing are translatable elsewhere.
The study’s strengths include input from a range of people who have provided some very helpful insights. The data were analysed in an unidentified format. The limitations include small number of participants (approached as opinion leaders, service providers or nominated at users and carers) who did reflect a range of appropriate views and suggestions. There is some potential bias as participants were nominated by their services or organisation (for service providers), or by their clinicians (for consumers) as people who could contribute in the online format.
These findings are in line with the report from the Productivity Commission 4 address issues raised about improving person-centred care, linking consumers to resources, access to online resources and experiences beyond the health system. The hospital has access to a suite of online therapeutic programs with potential to provide navigation to other online resources. Additionally, the Mental Health Service will use the site for current group therapy programs, and we envisage an ongoing group program to improve mental health literacy and empowerment in an effective and cost-effective manner.
Cluley et al 2 recommended PPI research from outset and continuation over community projects to gain feedback on services provided. This was also recommended by participants. This study represents the first small start of such research and has already highlighted the value of partnering with the local community to meet its needs in understanding perceived gaps and expectations improving mental health and wellbeing.
A systemic review 5 of 42 reviews of PPI health, social care and patient safety reported concern over lack of input from marginalised and seldom heard groups, with little discussion about how to address these concerns. Our study was more focussed towards those who were service providers to these groups but the site itself will enable more attention to individual voices from these seldom heard groups. Besides quantitative outcomes such as rates of service use and satisfaction, we have designed an ongoing anonymous survey for those attending the site and the local community to give ongoing feedback as the project develops. We also propose further focus groups after the service is underway.
Footnotes
Acknowledgements
The authors would like to thank Andrea Millar and Denise Yates for administrative support.
Authors’ Contributions
1. Kay Wilhelm: Chief Investigator, co-design of project, focus group leader and wrote the first draft.
2. Brooke Short: Co-design of project, focus group leader, input in qualitative analysis and manuscript preparation.
3. Lyn Chiem: Co-design of project, input into strategic planning and manuscript preparation.
4. Megan Son Hing: Focus group, attended 2 groups as support for participants, feedback on focus group material and manuscript preparation.
5. Francesca Schiavuzzi: Member of project team from outset, project manager, co-facilitator for groups as support and resource member.
6. Sean Evans: Member of project team from outset, advice and support for project.
7. Matt Taylor: Member of project team from outset, input on design of materials and process and output of focus groups, and preparation of manuscript.
8. Pat Grant: Member of project team from outset, observed all focus groups and responsible for qualitative data analysis.
Conflicts of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed the receipt of the following financial support for the research, authorship, and/or publication of this article. This work was supported by the St Vincent's Hospital Curran Foundation for providing donation to cover costs of vouchers for participants and qualitative analysis by Kernel group.
Ethical Statement
The study was approved by SVHS Human Ethics Committee (HREC 2021/073,778). All participants gave informed consent prior to focus group participation.