
Abstract
Objective
To determine bulk billing rates, and mean, median, and 10th and 90th centile fees for outpatient consultations with a psychiatrist in Australia in 2019, by state or territory.
Method
Medicare claims data for bulk billing rates and the mean, median, and 10th and 90th centile for fees charged in Australia in 2019 were requested, for item numbers for initial and ongoing consultations.
Results
There were high rates of bulk billing overall. Initial consultations were more likely to be bulk billed. There was variation in fees between states and territories. Fees were highest in the Australian Capital Territory.
Conclusion
There is variation in fees and bulk billing rates for outpatient consultations with a psychiatrist. Fees tend to be higher in states or territories with higher median personal income. Psychiatrists were more likely to bulk bill for initial consultations, with the exception of the Northern Territory. High rates of bulk billing may indicate psychiatrists are absorbing increasing costs of service provision.
In 2019–20, 1.7% of Australians received Medicare-subsidized services from a psychiatrist. 1 The Royal Australian and New Zealand College of Psychiatrists (RANZCP) has highlighted the costs of private outpatient psychiatry to consumers. 2 There is limited information on rates of billing practices of private psychiatrists. This study analyses 2019 Medicare claims data to determine bulk billing rates and the mean, median and 10th and 90th percentile levels of fees for a range of item numbers, by state and territory.
Background
A range of mental health services is provided in Australia by various levels of government. State and territory governments provide services including outpatient psychiatric care via community mental health services. The federal government funds consultations with psychiatrists and other practitioners through the Medicare Benefits Schedule. 3 Private health insurers are prevented from funding private outpatient specialist consultations 4 based on concerns that this would lead to increases in fees and a two-tiered healthcare system, where people with private health cover would have advantages over those without it. 5 Those who cannot afford private outpatient psychiatric care are not necessarily eligible to receive care in the public system, particularly if they do not meet the criteria for acuity used by public mental health services. This population may be going without mental health care and has been termed “the missing middle.” 6
Medicare provides rebates for outpatient consultations to Medicare cardholders to offset the cost of these services. This payment is based on the schedule fee, the amount determined by the Department of Health as being reasonable, on average, for the service provided. The schedule fee for each service is published in the Medicare Benefits Schedule. 7 Medicare will cover 85% of the schedule fee. Psychiatrists may accept this amount (bulk billing) or may charge a “gap,” an amount in surplus of the Medicare benefit. The Medicare safety net provides extra rebates once an individual or family’s out-of-pocket medical costs reach a set amount in a calendar year ($495.60 and $2249.80 for the general and extended safety nets respectively in 2022). 8
There have been several “freezes” on indexation of Medicare rebates imposed by the Australian Government in an attempt to limit spending. 9 While indexation has recommenced, the Australian Medical Association (AMA) regards the pricing schedule as inadequate to cover costs associated with service delivery. The AMA issues its own recommended fee schedule. 10 It encourages medical practitioners to “charge a fair and reasonable fee having regard to their practice costs and the particular individual circumstances of their patients.” 10 There is variability in billing among non-psychiatric medical specialists. Freed and Allen found variation in fees charged by consultant physicians across states and territories. 11 They concluded that the basis for this variation was unclear, and that patients were unable to assess the relationship between quality of service and fee charged. 11 Claims data submitted to Medibank by private hospitals in 2016 shows variation in surgeons’ fees, with average out-of-pocket costs for MBS item for bowel resection varying by up to $1235 between states. 12 Media reports have highlighted the difficulty in accessing affordable outpatient psychiatric care, with consumers reporting that bulk billing has become an uncommon practice. 13
The Australian government has commissioned review of Australia’s mental health care system, which identified that reforms are needed to improve outcomes for those with mental illness, with emphasis on improved access to early community-based intervention inclusive of outpatient psychiatry consultations. 14 To date, no studies have examined billing practices of outpatient private psychiatrists in Australia. This data is important as costs are a potential barrier to accessing private outpatient psychiatric care, and may inform the implementation of service reform.
Method
Item numbers and scheduled fee for 2019
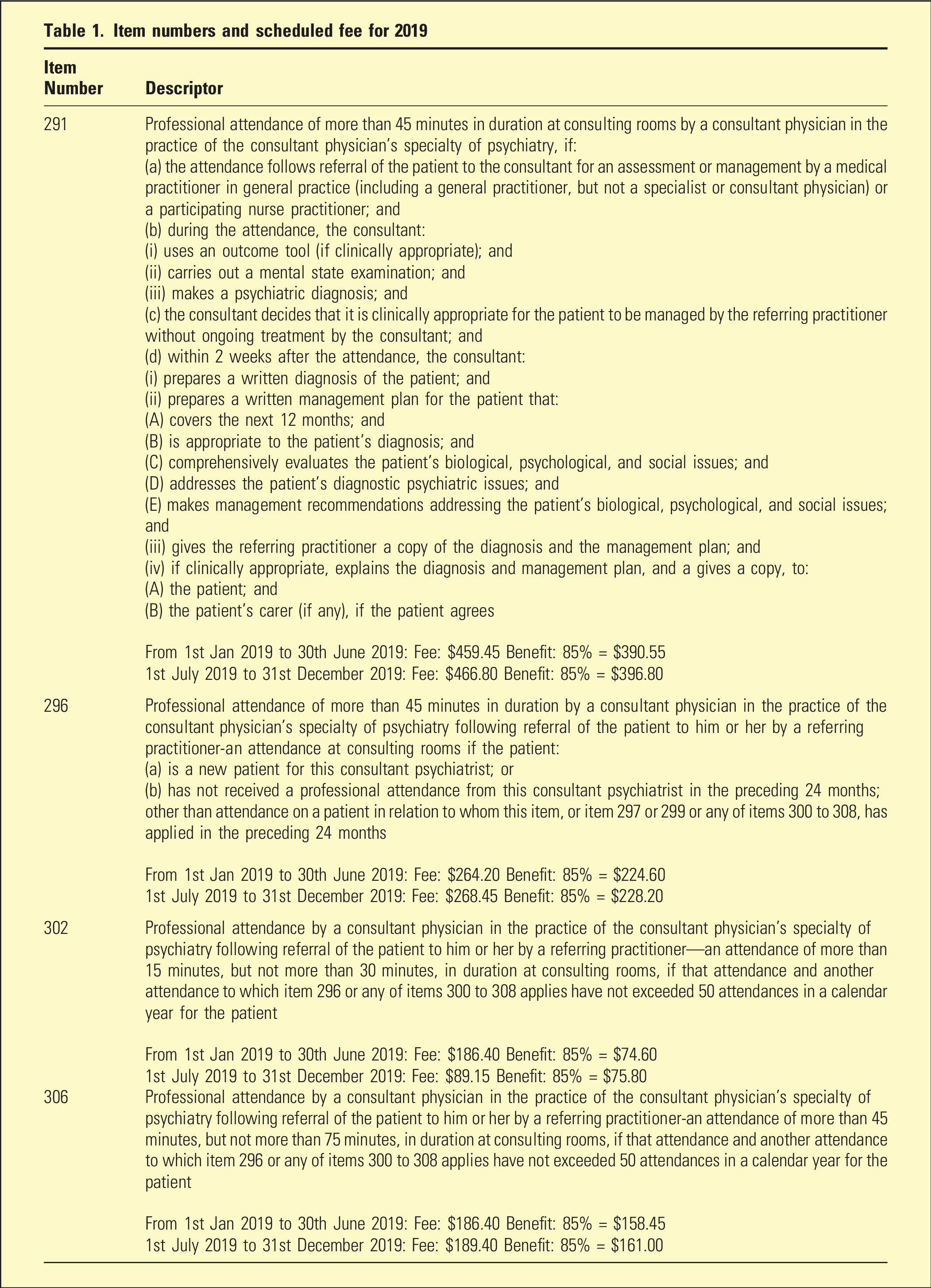
Request was made for number of services for which a claim for benefit was made, aggregated by state or territory, and item number. Also requested was number of bulk billed items by state or territory and item number. Services Australia provided mean, median, and 10th and 90th percentile levels of actual charges by psychiatrists, by item number and state or territory of the provider. To prevent providers or consumers being identified, Services Australia suppressed data when fewer than 7 services were provided in a state or territory.
Results
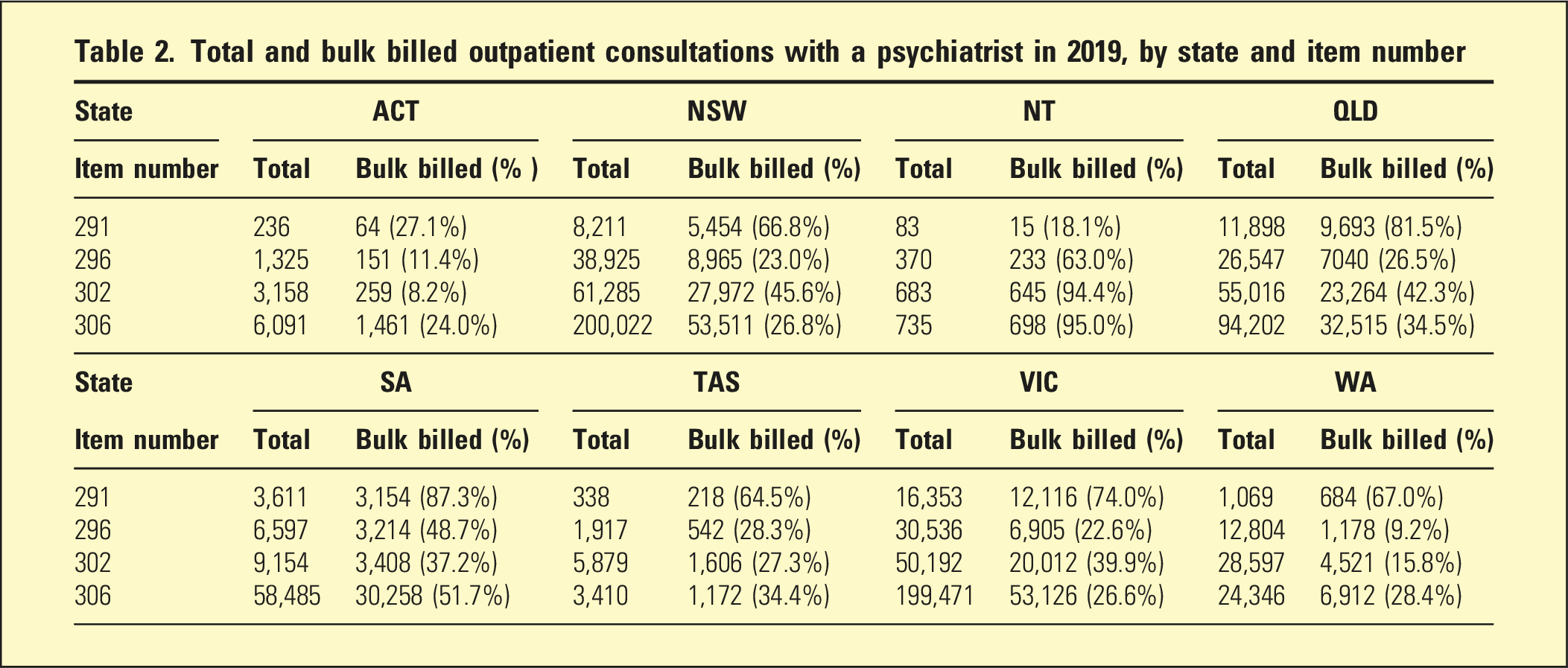
Total and bulk billed outpatient consultations with a psychiatrist in 2019, by state and item number
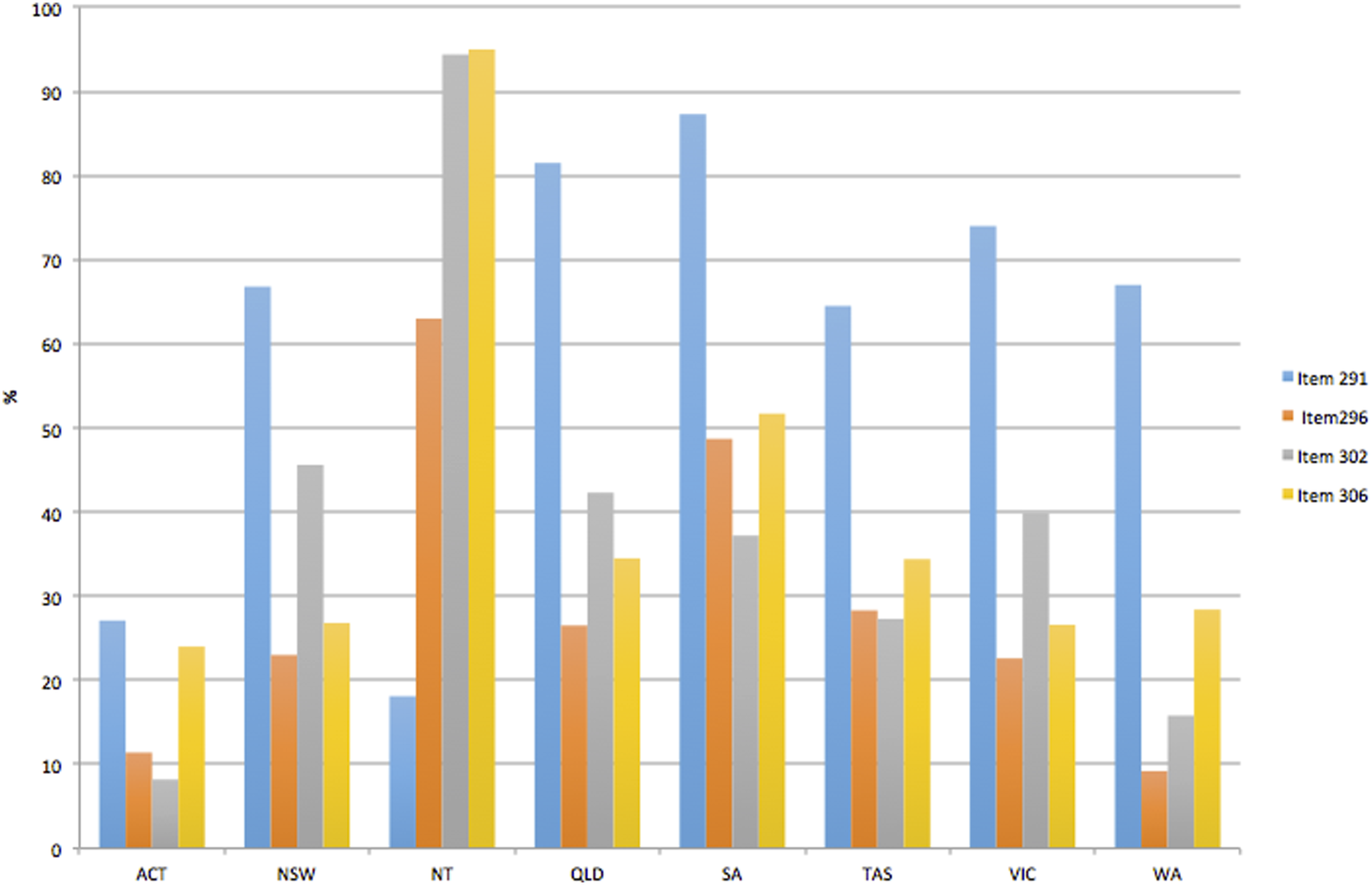
Proportion of bulk billed consultations with a psychiatrist, by state and item number in 2019.
Fees for outpatient consultation with a psychiatrist, by state or territory and item number
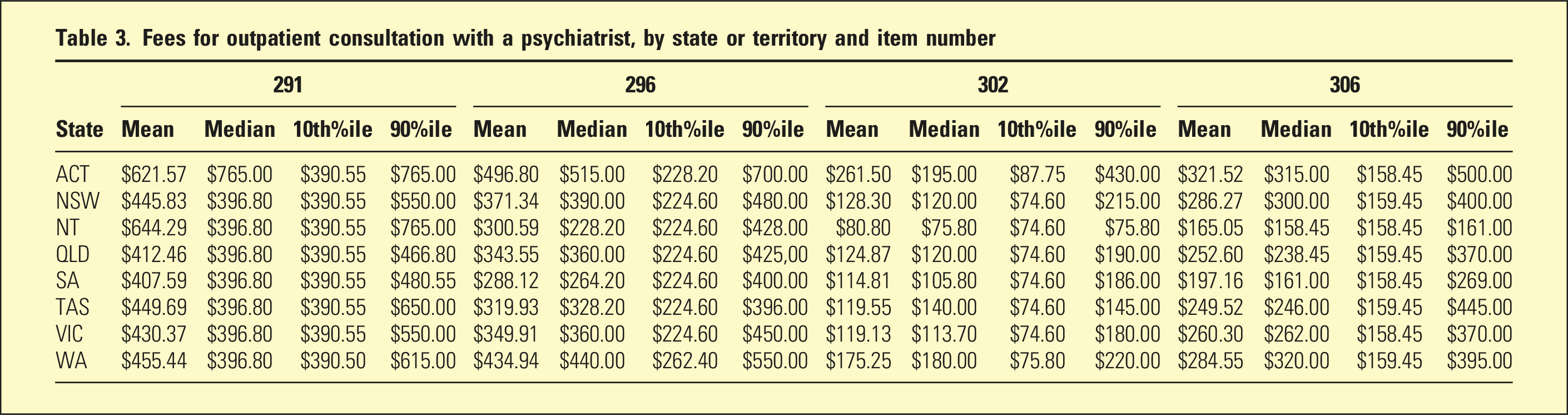
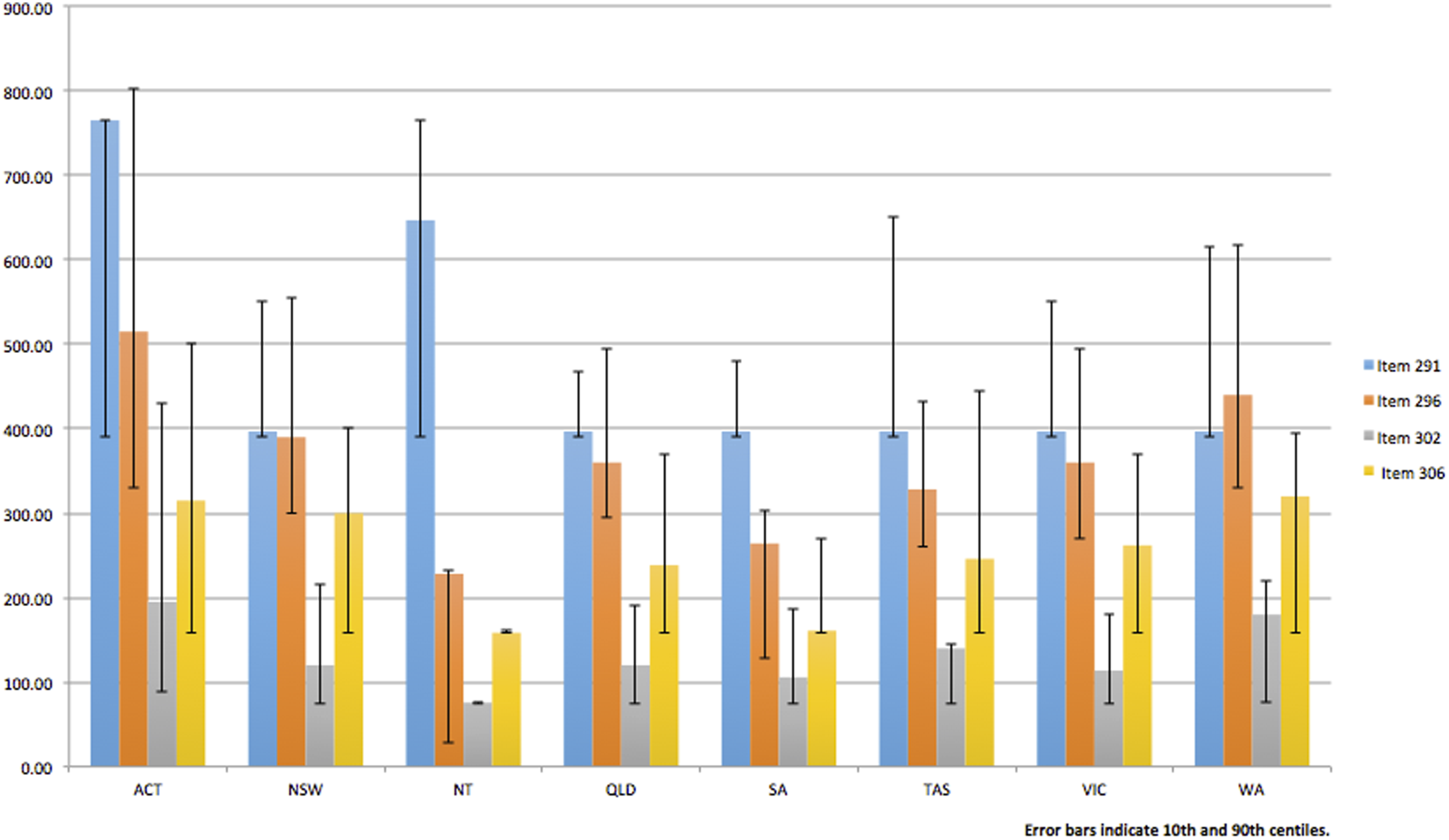
Median fees for outpatient consultations with consultant psychiatrist by item number and state.
Bulk billing
There was variation in rates of bulk billing by state or territory and by item number. The ACT had lower rates of bulk billing across all item numbers. Item 291 was bulk billed at the highest rate, with the exception of the Northern Territory (NT), where items 302 and 306 were bulk billed at a higher rate (94.4% and 95%, respectively, compared to 18.1% for the 291).
Fees
There was variation in fees charged between states and territories. The highest mean fees for all item numbers were charged in the Australian Capital Territory (ACT). Lowest average fees for item numbers 291 and 296 were found in South Australia, and lowest fees for item numbers 302 and 306 were found in the NT. The 90th centile fee was up to 490% greater than the 10th centile fee (for item 302 in the ACT).
Discussion
There was variation between states and territories in fees charged by consultant psychiatrists for outpatient consultations. Highest fees were in the ACT. This is counter to the hypothesis that areas with higher supply of psychiatrists would have lower fees, as the ACT had the highest rates of full-time equivalent (FTE) psychiatrists per 100,000 of population in 2019, at 16.9. 17 The finding may reflect that population’s higher median income. 18 Lower fees in South Australia may reflect the combination of that state’s higher number of FTE psychiatrists per capita and lower median personal income.17,18
There was also variation in bulk billing rates between states and territories and between item numbers. Overall, rates of bulk billing were high. This suggests psychiatrists may be absorbing the increasing costs of service provision in the setting of inadequate increases to the Medicare benefits schedule, rather than passing them on to consumers. There were higher rates of bulk billing for more highly remunerated items (291 and 296), to the extent that the median fee for the 291 represented the bulk billed fee in all states, but not the territories. This may reflect psychiatrists considering the impact of the higher costs of these item numbers to consumers. In the NT, there was a low rate of bulk billing of the 291 and 296, and almost universal bulk billing of items 302 and 306. A potential explanation is that many follow-up appointments in the NT may be provided by bulk billing clinics, for example, at Aboriginal-controlled health organizations.
A major limitation of this study was the inability to determine statistical significance of variation, given the lack of statistical tests of population means. Variation in the territories may be due to the smaller size of these datasets. Administrative delays in accessing data mean that study findings are not contemporaneous, reducing their relevance. In 2020, there were likely to be broad changes in the billing habits of psychiatrists in the setting of the COVID-19 pandemic. Telehealth became widely used and bulk billing was made mandatory for a period. Analysis of this data would have limited generalizability to post-pandemic practice. Another limitation was the inability to link claims data to factors such as level of experience of the psychiatrist, consumer’s diagnosis and income, total consultations per consumer per year, and cost of service provision. Future research may involve interviewing psychiatrists regarding their approach to billing. This study is also limited to providing information from a single year. Longitudinal analysis of billing would enable comparison against changes in the Medicare benefitschedule, inflation, and wage growth.
This study illustrates the actual costs to consumers of private psychiatric outpatient care in Australia. Average cost for an initial appointment (291) with a psychiatrist ranged from 40.5 to 61.8% of the median Australian weekly personal income for the 2019/2020 financial year. 18 Average cost for 15 to 30 minute follow-up appointment (302) was represented between 16.4 and 31.9% of median weekly personal income. 18 In light of findings of variation in fees set by physicians, Freed and Allen suggested that the Australian Government’s rule preventing health insurers from covering outpatient consultations had failed to prevent increases in fees. 10 In their submission to the Productivity Commission’s Inquiry into Mental Health, Health Insurance Australia noted that the rule is at odds with evidence that mental health conditions can be effectively treated in community. 19 The Productivity Commission has since recommended review of the rule. 20 Allowing health insurers to subsidize outpatient psychiatric consultations would improve access for the 45.2% of Australians who hold private health insurance. 21 However, government subsidies benefit all consumers, rather than only those who can afford health insurance. The Australian government spent 7.6% of its total health expenditure on mental health service provision in 2019/20, 22 despite mental illness representing 13% of Australia’s total burden of disease, 23 indicating scope for increased investment. Whether funded publically or privately, it is possible that increased rebates for outpatient psychiatric consultations could lead to price increases, with limited benefits to consumers.
These findings are important for consumers who may not be aware of the variation in psychiatrists’ fees. The RANZCP’s Code of Ethics states that psychiatrists should disclose the costs of any proposed treatments as part of obtaining informed consent. 24 Awareness of what could be considered a reasonable fee is important for the consumer when giving consent.
In Australia, it is not possible for consumers to know whether higher fees translate to a higher quality of care. In the United States, the Quality Payment Program has introduced the use of outcome measures that determine the reimbursement a physician receives from Medicare. 25 The Productivity Commission Inquiry into Mental Health has recommended that the Australian government should, as a priority reform, require monitoring and reporting of Medicare-rebated services. 26 While increasing workloads for psychiatrists, this may reduce unexplained variability in fees.
Conclusion
There is variation in bulk billing rates and fee setting by psychiatrists for outpatient consultations. This may be partly explained by variation in the state or territory’s median personal income and number of psychiatrists. Bulk billing rates are generally high, suggesting psychiatrists are not passing on rising costs of service provision to consumers. Fees represent a substantial proportion of median Australian weekly personal income, and may be a barrier to accessing care.
Footnotes
Acknowledgements
The authors wish to acknowledge the advice of Dr. Tacita Powell, Dr. Dave Carmody, Professor Gary Freed, and Mr. Andrew Beaufoy.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethics approval was obtained from the St Vincent’s Hospital Melbourne Human Research Ethics Committee (ID 84351). Consent statement was not required.