
Abstract
Objective
We aimed at exploring the relationship between functional outcomes in patients on clozapine augmented with antipsychotics in treatment-resistant schizophrenia using standard outcome measures Health of Nation Outcome Scales (HoNOS) and Life Skills Profile (LSP-16).
Method
In a cross-sectional study of 83 patients on clozapine treated in a psychiatric rehabilitation hospital, the association between the primary outcome measure, LSP-16 including its subscales, and treatment with antipsychotic augmentation (AA) were analysed using linear regression.
Result
The presence of moderate-to-severe positive symptoms on the HoNOS 6 dichotomised item measure was the only statistically significant predictor of functional impairment as determined by total LSP-16 score.
The group of patients with ongoing positive symptoms (partial responders) were characterised by higher total LSP-16 scores, higher numbers of AA agents, and higher chlorpromazine equivalence. There was an inverse linear relationship between chlorpromazine equivalence of AA and total score of LSP-16 scale in the group of partial responders.
Conclusion
Augmentation with other antipsychotic agents was associated with higher functioning in a cross-sectional study of patients with schizophrenia with poor response of positive symptoms to clozapine. This might be an important clinical factor to consider when prescribing antipsychotics to patients with clozapine-resistant schizophrenia.
Between 40% and 70% of patients with treatment-resistant schizophrenia do not respond to clozapine monotherapy, 1 resulting in worsened quality of life and greater economic burden. Whilst the addition of other antipsychotic medication to clozapine is common, literature search reveals conflicting and insufficient evidence of the benefits of this augmentation strategy to reduce the severity of symptoms and hospitalisation.1–3
Although the literature on the effect of clozapine augmentation on functional outcomes as opposed to the management of positive symptoms is even less available, a recent cross-sectional study comparing parenteral and oral augmentation with clozapine showed an improvement in functioning as determined by one HoNOS (Health of the Nation Outcome Scales) item in the parenteral arm. 4 Given that positive symptoms as well as anxiety, negative, and cognitive symptoms have been shown to impact functional outcomes,5–7 this study addressed the association of antipsychotics prescribed routinely to reduce positive symptoms in addition to clozapine on functioning measures collected in clinical practice.
This study aimed to supplement the limited existing research addressing functional improvement in patients on clozapine, augmented with another antipsychotic. Using a similar approach to Mukherjee and Sazhin, 4 our research explored the association between functional improvement on the Life Skills Profile (LSP – 16) scale and antipsychotic augmentation (AA) of clozapine adjusted for relevant clinical factors.
LSP-16 is a standard clinician-rated scoring instrument recommended by Australian guidelines to measure functioning of patients with mental illness and is the abbreviated version of the LSP-39 that includes sixteen items and four subscales (withdrawal, self-care, compliance, and antisocial). LSP-16 has strong validity and accuracy and represents a real-world measure of functional improvement in hospitals and community settings. 8
Methods
Participants
This study is a single-centre, cross-sectional study conducted at a major psychiatric hospital in Sydney, Australia. The 83 subjects included in the study were inpatients of rehabilitation wards who were treated with clozapine for schizophrenia or schizoaffective disorder in 2019. The local health district Human Research and Ethics Committee provided ethical approval and waiver of consent for the study.
Data collection
Data was collected from electronic and paper medical records and de-identified. The date of data collection was selected when both HoNOS and LSP-16 scores were available on the same day (with the exception of two patients whose scores were less than 2 months apart). Demographic details were obtained in addition to the dose of clozapine, duration of clozapine treatment, and duration of hospitalization calculated on the date of the outcome scores. The doses of clozapine and augmenting antipsychotics were averaged over the period of 2 weeks prior to their HONOS and LSP-16 scores.
Chlorpromazine equivalence was calculated for each antipsychotic agent augmenting clozapine using the Defined Daily Dose (DDD) method. 9
Statistical strategy and analysis
Descriptive data was analysed using non-parametric Wilcoxon rank-sum test, chi-square test, and t-test.
Linear regression modelling of the LSP-16 total and subscale score(s) as the dependent variables, and clinical and demographical factors as their predictors was conducted using Stata-17 statistical package.
To include as an independent predictor, the 5-level categorical variable of HoNOS item 6 (Problems associated with hallucinations and delusions) was transformed into a dichotomous variable by combining the categories 0 and 1 into the ‘full responders’ group and the categories of 2, 3, and 4 into the ‘partial responders’ group. This approach to condense HoNOS items to a dichotomous variable has been commonly used to address the low numbers of events in each category to perform a statistical analysis and simplify its clinical interpretation.10,11
Results
Clinical and demographic characteristics of patients with schizophrenia on clozapine treated in a long-term rehabilitation hospital
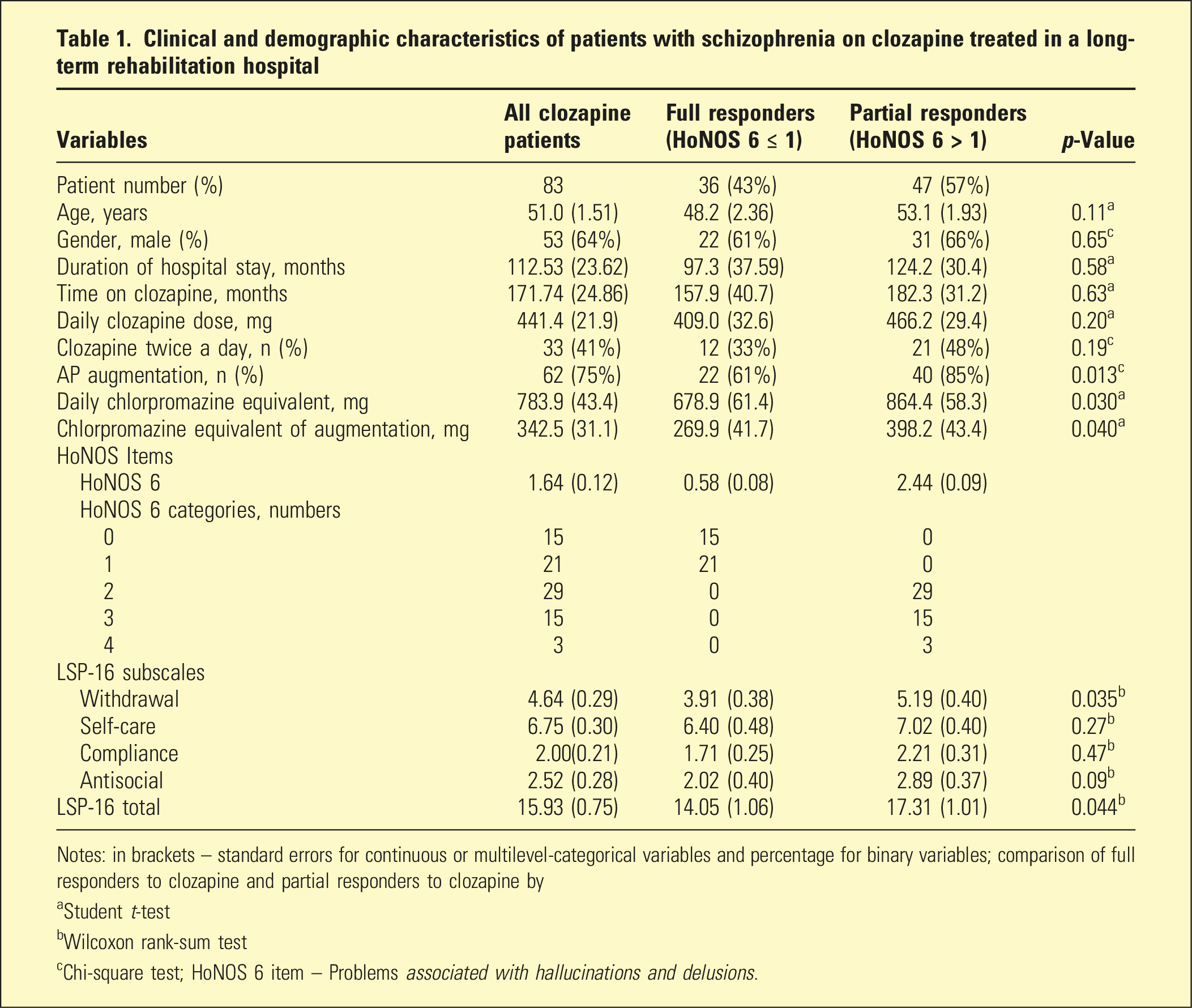
Notes: in brackets – standard errors for continuous or multilevel-categorical variables and percentage for binary variables; comparison of full responders to clozapine and partial responders to clozapine by
aStudent t-test
bWilcoxon rank-sum test
cChi-square test; HoNOS 6 item – Problems associated with hallucinations and delusions.
More than a half of all patients (47/83) suffered from ongoing positive psychotic symptoms (scores 2-4 on HONOS item 6 – hallucinations/delusions) and were considered partial responders. The group of partial responders had a higher total of LSP-16 score and higher number of AA agents than full responders.
Linear regression analysis of functional impairment on LSP-16 scale (total LSP-16 score)
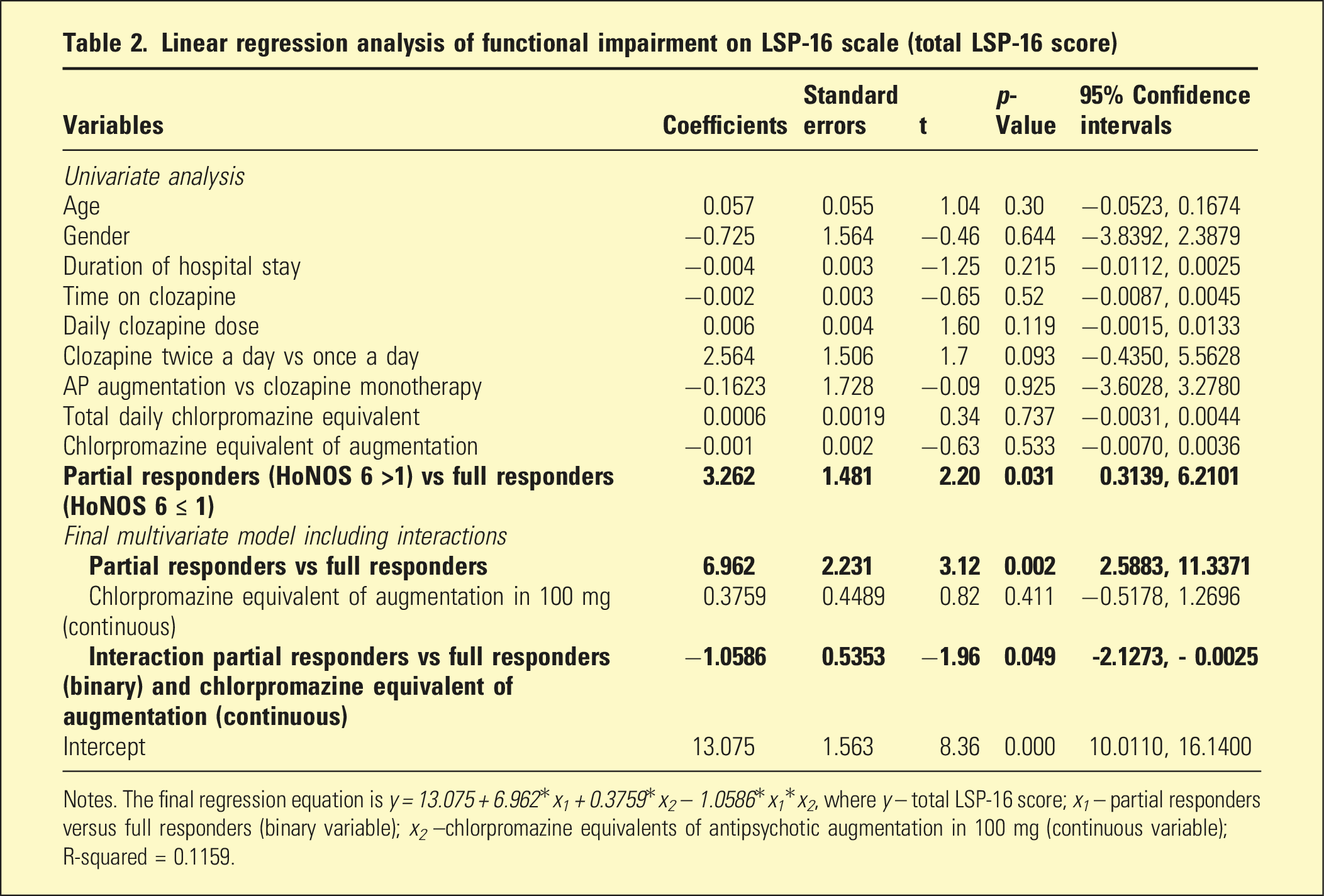
Notes. The final regression equation is y = 13.075 + 6.962*x 1 + 0.3759*x 2 – 1.0586*x 1 *x 2 , where y – total LSP-16 score; x 1 – partial responders versus full responders (binary variable); x 2 –chlorpromazine equivalents of antipsychotic augmentation in 100 mg (continuous variable); R-squared = 0.1159.
A multivariate analysis with backward stepwise elimination showed that the only statistically significant predictor interacting with HoNOS 6 item was the chlorpromazine equivalence of antipsychotic medication (Table 2). The residuals of the final model were normally distributed (Jarque–Bera normality test, p = .21) and met the condition of homoscedasticity (Breusch–Pagan test, p = .43). The final model showed that the total LSP-16 score of partial responders was 6.962 ± 2.231(p = .002) higher than those of full responders in patients on clozapine monotherapy. Augmentation of the full responders group with antipsychotics was not associated with lower total LSP-16 scores. Partial responders’ total LSP-16 score was lowered by −1.0586 ± 0.53(p = .49) with every 100 mg of chlorpromazine equivalent of antipsychotics added to clozapine in comparison to the full responders group (effect size Cohen’s d = 0.74, 95% CI [−0.08, 1.56]).
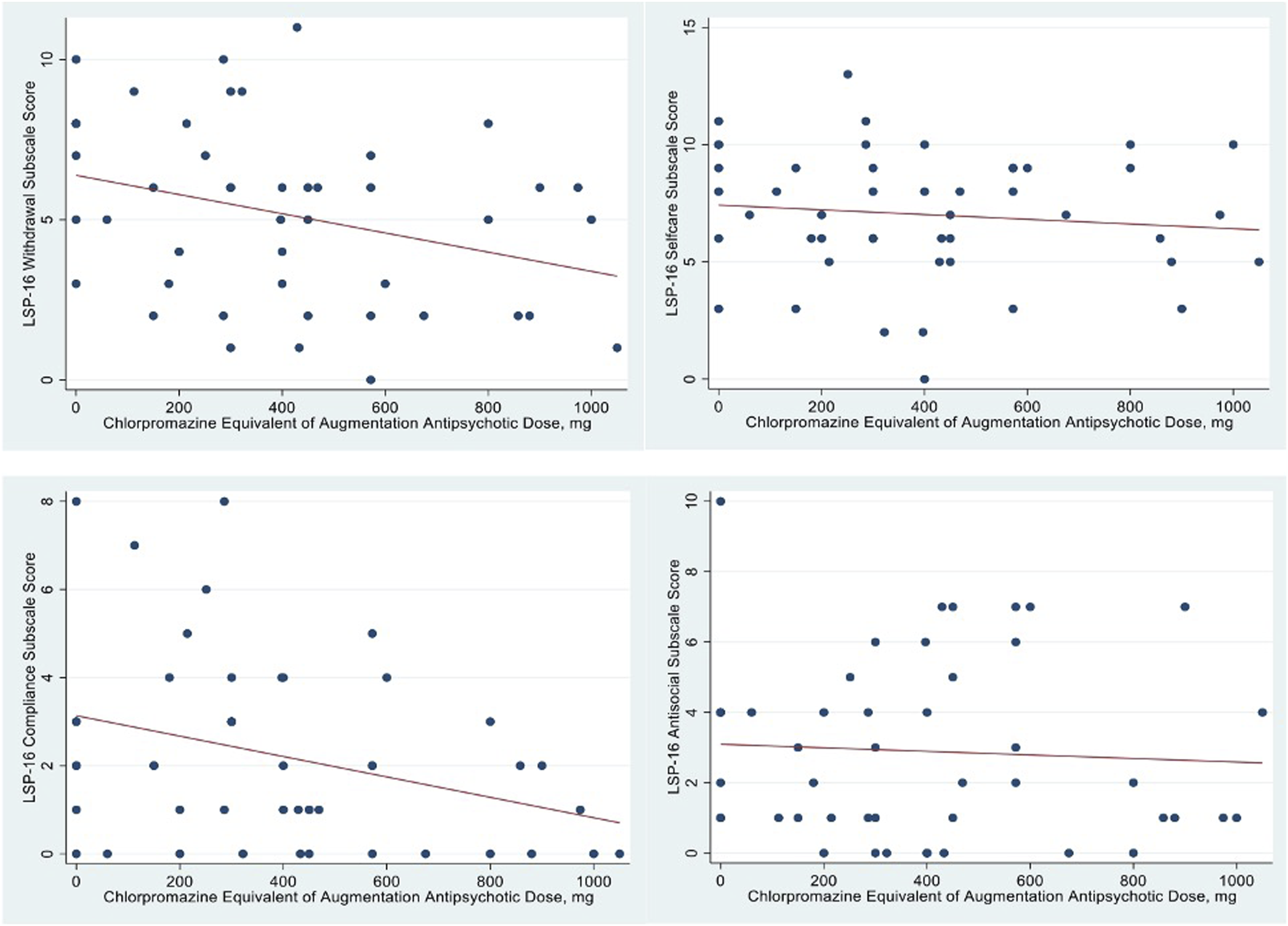
There was an inverse linear relationship between chlorpromazine equivalence of AA and total score of LSP-16 within the group of partial responders, with the addition of antipsychotic to clozapine being associated with a 20%–25% lower average impairment score for daily doses above 600 mg chlorpromazine equivalence of the augmenting agent (Figure 1). In separate linear regression analyses, the effect of antipsychotic augmentation on the subscale LSP-16 scores in partial responders did not reach statistical significance. However, the positive effect of antipsychotic augmentation on functioning appears to have been largely due to lower scores on the withdrawal and compliance subscales, reflecting the patients’ better participation in their treatment and social contacts (Figure 2). Relationship between the chlorpromazine equivalent of antipsychotic augmentation (mg) (x-axis) and total LSP-16 score (y-axis) in full responders (HoNOS 6 item ≤ 1) (left graph) and partial responders (HoNOS 6 item > 1) (right graph) to clozapine with schizophrenia (the scatter plots were fitted with linear regression lines). Relationship between the daily chlorpromazine equivalent of augmentation antipsychotics (mg) (x-axis) and LSP-16 subscale score (y-axis) – withdrawal (top left), self-care (top right), compliance (bottom left), and antisocial (bottom right) in partial responders (HoNOS 6 item >1) to clozapine with schizophrenia (the scatter plots were fitted with linear regression lines). The regression coefficients for all LSP-16 subscales were not statistically significant.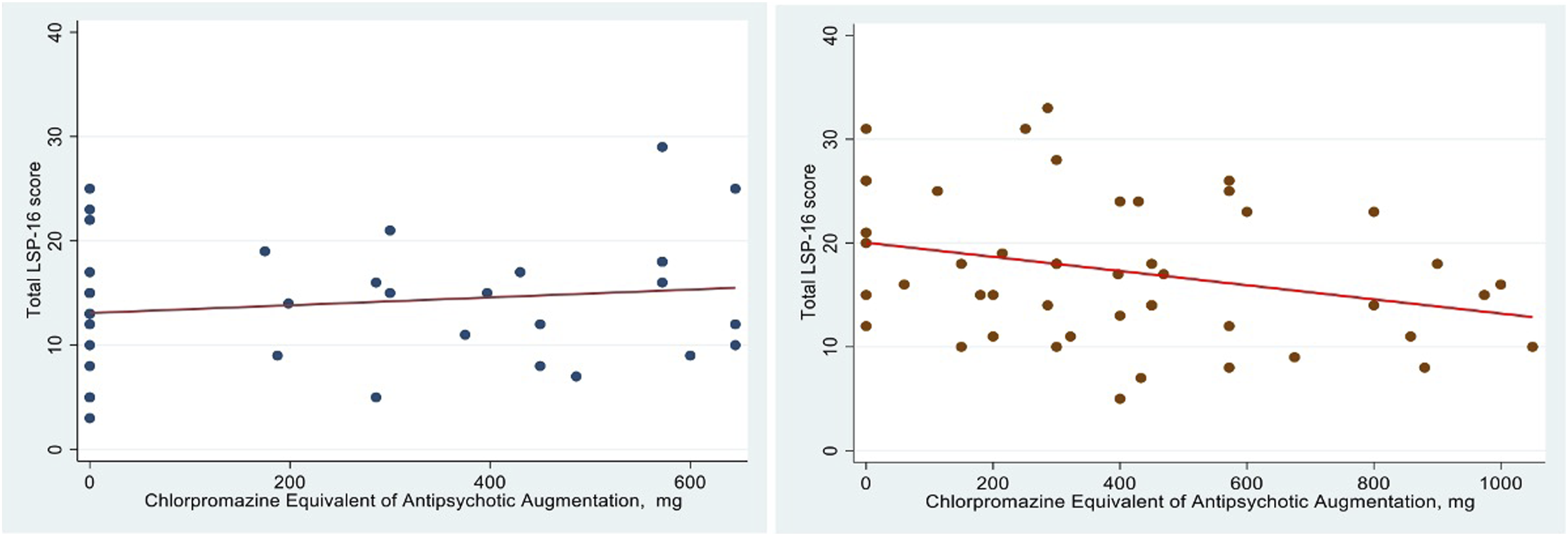
Discussion
To our knowledge, this is the first study exploring the real-world data of functional improvement across multiple domains on standardised tools in schizophrenia patients augmented with antipsychotics on clozapine, stratified by the level of response to clozapine.
Evaluating the data on LSP-16 revealed expected results and reinforced existing literature in detailing poorer functioning related to severity of psychotic symptoms in those with treatment-resistant schizophrenia. 1 Patients on clozapine in our dataset were rated higher on the LSP subscale of self-care which represents the impairment in daily activities, ability to maintain nutrition, general health, and capacity to work. The patients on clozapine also suffered from significant problems in the functional domain of social interaction and maintaining social contacts measured on the withdrawal subscale. This may reflect this cohort’s inherent struggle with social interaction due to positive and negative symptoms exacerbated by prolonged stays in psychiatric wards, an environment where social interactions are often restricted or constrained.12,13
This study revealed a significant difference between full responders and partial responders who had an average clozapine daily dose of 466 mg and ongoing positive symptoms and were very similar to the clozapine-resistant schizophrenia patients defined by Chakrabarti. 3 The group of full responders had a notable absence of psychotic symptoms and better functioning while partial responders had ongoing positive symptoms and seriously impaired global functioning, particularly, in the social interaction domain. The group of partial responders had a higher proportion on AA and a higher chlorpromazine equivalence that likely indicated a higher resistance of psychotic symptoms in these patients.
It is a common clinical practice to use AA in case of limited efficacy, poor compliance, and poor tolerance of clozapine. Although in a cross-sectional study such as ours it is not possible to assess the outcome of AA intervention, our results showed that an addition of antipsychotics to clozapine in a group of patients with chronic schizophrenia affected by ongoing positive psychotic symptoms and hospitalised for a long period of time, was associated not only with improvement in symptoms but also manifests in functional improvement.
We hypothesise that the benefits of augmenting clozapine with other antipsychotic agents in this cohort resulted in better social interaction and participation in rehabilitation activities. The results did not demonstrate higher functioning with AA in the full responders group, which can be explained by the small sample and low baseline LSP-16 scores in the full responders group.
Limitations
The cross-sectional design of the study allows only the conclusion of the association between AA of clozapine and functioning, not causality. The interrater variability and choice of standardised scales might affect the associations between the predictors. The study sample was small, and statistical power to detect predictors was limited. The lack of association between HoNOS items related to functioning outside of item 6 is potentially explained by the small sample size, as only the strongest predictors were able to be identified. The study did not evaluate the side effects of co-prescribing clozapine with other antipsychotics and their impact on general health, negative symptoms, nor was it able to gather clozapine or norclozapine levels. Another limitation of the study was that baseline cognitive functioning data apart from HoNOS item 4 was not available.
Conclusion
In a cross-sectional study of patients with schizophrenia with a poor response of positive symptoms to clozapine, augmentation with other antipsychotic agents was associated with an improvement in functioning, specifically, in areas of social interaction and compliance with treatment. The evaluation of the benefits and safety of AA in patients with clozapine-resistant schizophrenia will need to include a greater focus on the functional outcomes in future research.
Footnotes
Disclosure
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Northern Sydney Local Health District Human Research Ethics Committee provided ethical approval and waiver of consent for the study (Approval Number: 2020/ETH00864).