
Abstract
Objective
The systematic review evaluated the association of subclinical hypothyroidism (SCH) with metabolic syndrome (MetS) and specific MetS components in people with major psychiatric disorders.
Methods
A systematic review and meta-analysis was conducted to evaluate the association of SCH with MetS and its components in people with major psychiatric conditions.
Results
Five studies incorporating 24,158 participants met the inclusion criteria. All five studies comprised patients with depression and/or anxiety. Three studies incorporating 3365 participants were suitable for the meta-analysis. The pooled Odds Ratio (OR) of MetS was 3.46 (95% Confidence Interval/CI = 1.39–8.62) in major depressive disorder (MDD) and anxiety disorders patients with concurrent SCH compared to those without SCH. Meta-analysis showed a significant positive association between SCH and high body mass index (OR = 2.58, 95%CI = 1.33–5.01), high fasting plasma glucose (OR = 3.05, 95%CI = 1.79–5.18) and low high-density lipoprotein cholesterol (OR = 2.30, 95%CI = 1.82–2.92).
Conclusions
These findings suggest a significant positive association between MetS and SCH in people with MDD and anxiety disorders. This review informed the clinical implications of MetS in MDD with comorbid SCH and the importance of early diagnosis and treatment for SCH and MetS in psychiatric patients.
Keywords
Subclinical hypothyroidism (SCH) with mental illness is of high clinical importance because of the consequences of neuropsychiatric, 1 and cognitive disorders, 2 metabolic syndrome (MetS) 3 and cardiovascular diseases. 4 SCH is more common than overt hypothyroidism among people with MetS. 5 Additionally, SCH is associated with more severe symptoms of psychiatric disorders and poorer response to treatment in people with major depressive disorder (MDD). 6 Although SCH increases susceptibility to underlying psychiatric and metabolic conditions, there is limited evidence on the relationship between MetS and SCH among the psychiatric population.
Routine screening and early intervention of SCH in at-risk groups may prevent the onset of overt hypothyroidism and benefit early diagnosis and treatment of both SCH and MetS. 3 Before recommending routine screening for SCH among psychiatric patients with comorbid MetS, it is important to gain insight into the link between both disorders in psychiatric patients. Thus, we conducted a literature review on MetS and SCH in psychiatric patients.
The aims of this review were to evaluate the association of SCH with MetS and with specific MetS components in people with major psychiatric disorders.
Methods
A systematic review and meta-analysis were conducted and reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). 7
A systematic and comprehensive search strategy was developed. The search was adapted according to the database and librarian’s advice. PsychINFO, MEDLINE and Embase were searched (Appendix-1). A hand search of reference lists was also conducted to identify eligible articles. Two reviewers independently screened and retrieved each record for eligibility.
Studies were included if they investigated all three conditions: SCH, MetS or metabolic components and major psychiatric disorders, defined below.
Non-English studies, non-human studies, case reports, reviews and articles that did not investigate all three conditions were excluded. Studies conducted among people age<18, pregnant women, severe medical conditions, eating disorders and severe substance use disorders were excluded.
SCH – an elevated serum thyroid stimulating hormone (TSH) concentration higher than 4.0 mIU/L (normal = 0.4–4.0 mIU/L) with a normal free thyroxine (FT4) concentration (10–20 pmol/L). 8
MetS – a cluster of at least three of five medical conditions, according to the modified National Cholesterol Educational Program Adult Treatment Panel-III criteria (NCEP-ATP-III): Increased waist circumference (≥102cm-men, ≥88cm-women), elevated triglycerides cholesterol (TG-C)≥1.7 mmol/L, reduced HDL-C (high-density lipoprotein cholesterol)(<1.0 mmol/L in men,<1.3 mmol/L in women), elevated BP ≥ 130 systolic or ≥85 diastolic, or elevated fasting plasma glucose (FPG) > 5.5 mmol/L. 3
Major psychiatric disorders included were schizophrenia spectrum and other psychotic disorders, depressive disorders, bipolar affective disorders and anxiety disorders.
The Agency for Healthcare Research and Quality (AHRQ) test was used for the quality assessment of cross-sectional studies. Two reviewers independently reviewed the quality assessment.
Meta-analysis was performed to assess the risk of MetS or each component of MetS in people with major psychiatric disorders and comorbid SCH by calculating the Odds Ratios (OR) with 95% Confidence Intervals (CI).
Statistical heterogeneity across studies was assessed through Cochran-Q and I2 statistics. Considering the diversity of included studies, a random-effects model was used. Heterogeneity was further assessed by conducting a sensitivity analysis that removed a study identified as a potential outlier. Publication bias was evaluated through funnel plots, Begg and Egger tests.
Results
The selection process of included studies is shown in the PRISMA flow diagram (Figure 1).
7
PRISMA flow diagram of the selection of studies.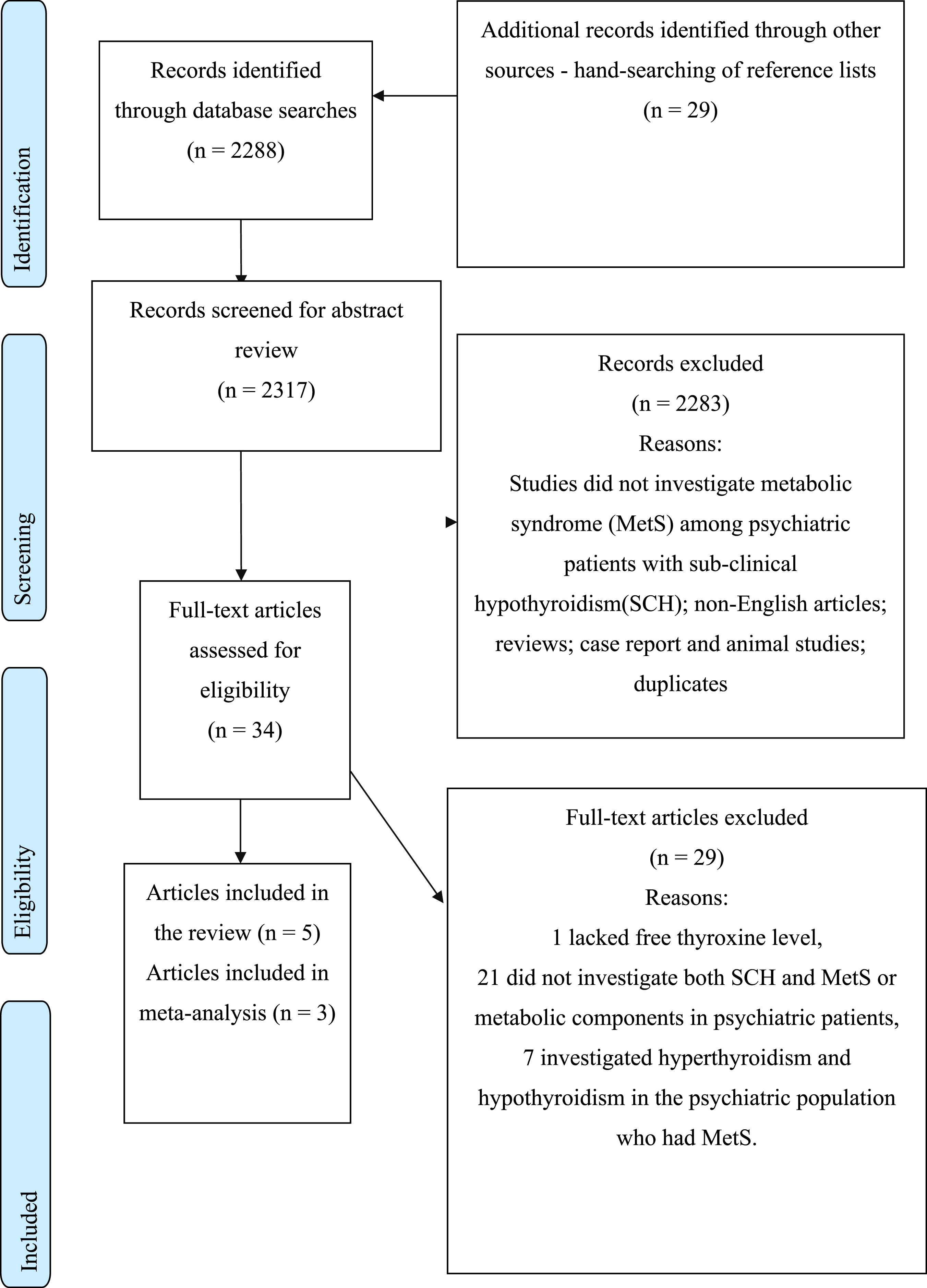
Five studies were included(Characteristics in Appendix-2).9–13 All included studies examined SCH and MetS or metabolic components in people with MDD and anxiety disorders.9–13 Out of 24,158 participants in the review, 2995 had a first episode, drug-naïve MDD,11,12 2157 had a single and recurrent MDD,9,10 and 19,006 had mild depression and anxiety. 13
Quality assessment of included studies.
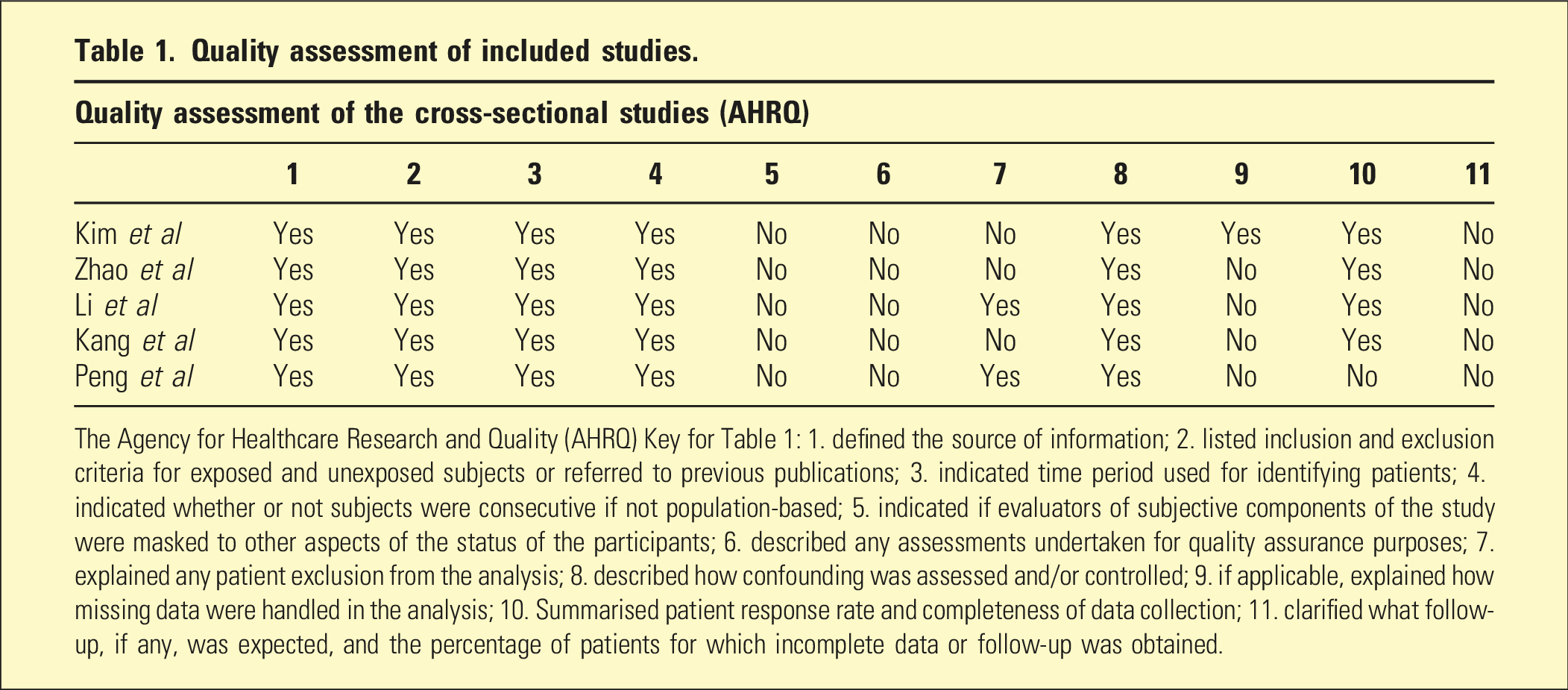
The Agency for Healthcare Research and Quality (AHRQ) Key for Table 1: 1. defined the source of information; 2. listed inclusion and exclusion criteria for exposed and unexposed subjects or referred to previous publications; 3. indicated time period used for identifying patients; 4. indicated whether or not subjects were consecutive if not population-based; 5. indicated if evaluators of subjective components of the study were masked to other aspects of the status of the participants; 6. described any assessments undertaken for quality assurance purposes; 7. explained any patient exclusion from the analysis; 8. described how confounding was assessed and/or controlled; 9. if applicable, explained how missing data were handled in the analysis; 10. Summarised patient response rate and completeness of data collection; 11. clarified what follow-up, if any, was expected, and the percentage of patients for which incomplete data or follow-up was obtained.
Descriptive characteristics and assessment criteria of depression, anxiety, MetS and SCH in the included studies are mentioned in Appendix-3.
The meta-analysis of three studies reported a significant positive association between MetS and SCH among people with MDD and anxiety (Figure 2, Table 2).10,12,13 Forest plot showing the association between subclinical hypothyroidism and metabolic syndrome. The association between subclinical hypothyroidism and metabolic syndrome and each component of metabolic syndrome. CI: confidence interval, I2: Heterogeneity, TG-C: triglyceride cholesterol, HDL-C: high-density lipoprotein cholesterol, FPG: fasting plasma glucose, *; p < .05 (statistically significant).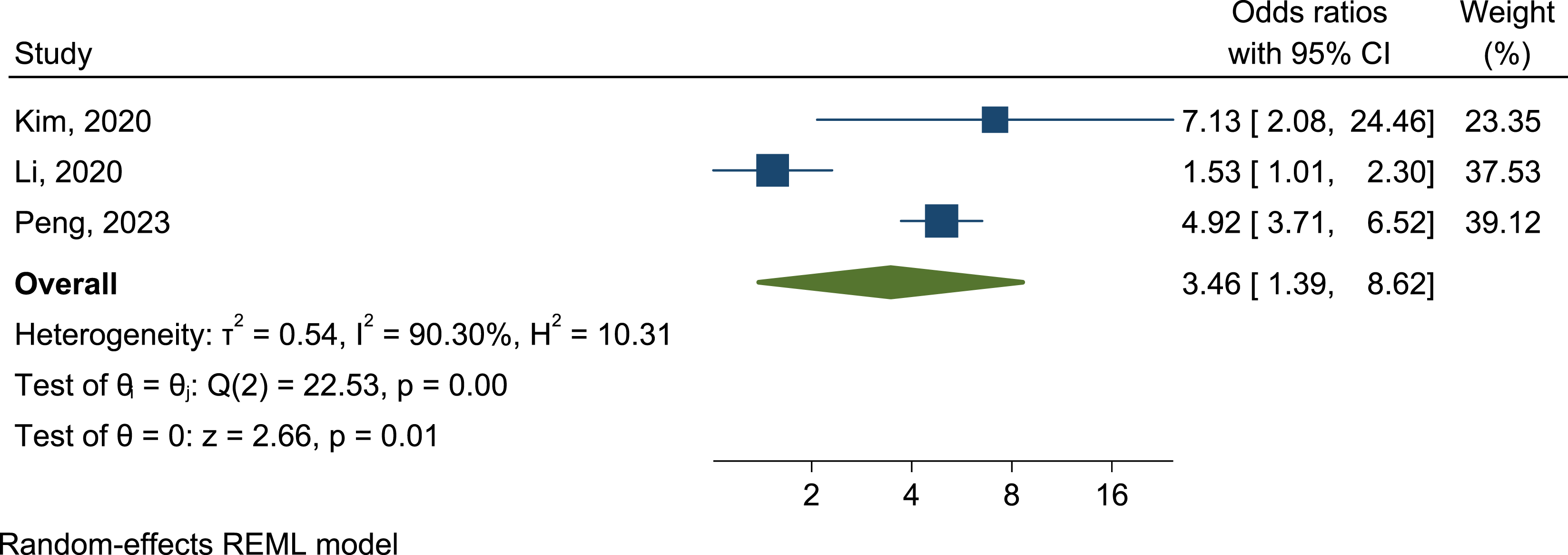
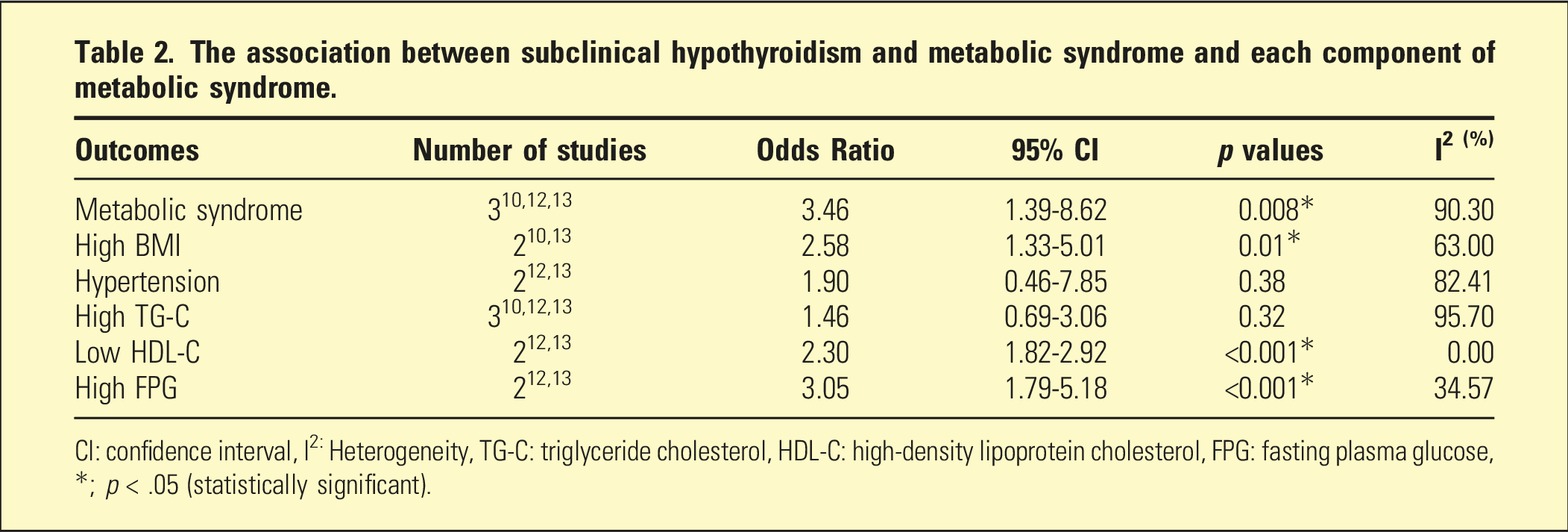
The results from three included studies with available data on each specific metabolic component showed a positive association of SCH with high BMI, hypertension, high TG-C, low HDL-C and high FPG levels.(Table 2, Figure 3) The association of SCH with hypertension and high triglycerides was not statistically significant. Additional results on metabolic components and assessment of publication bias are presented in Appendix-4. The association between subclinical hypothyroidism and each component of metabolic syndrome.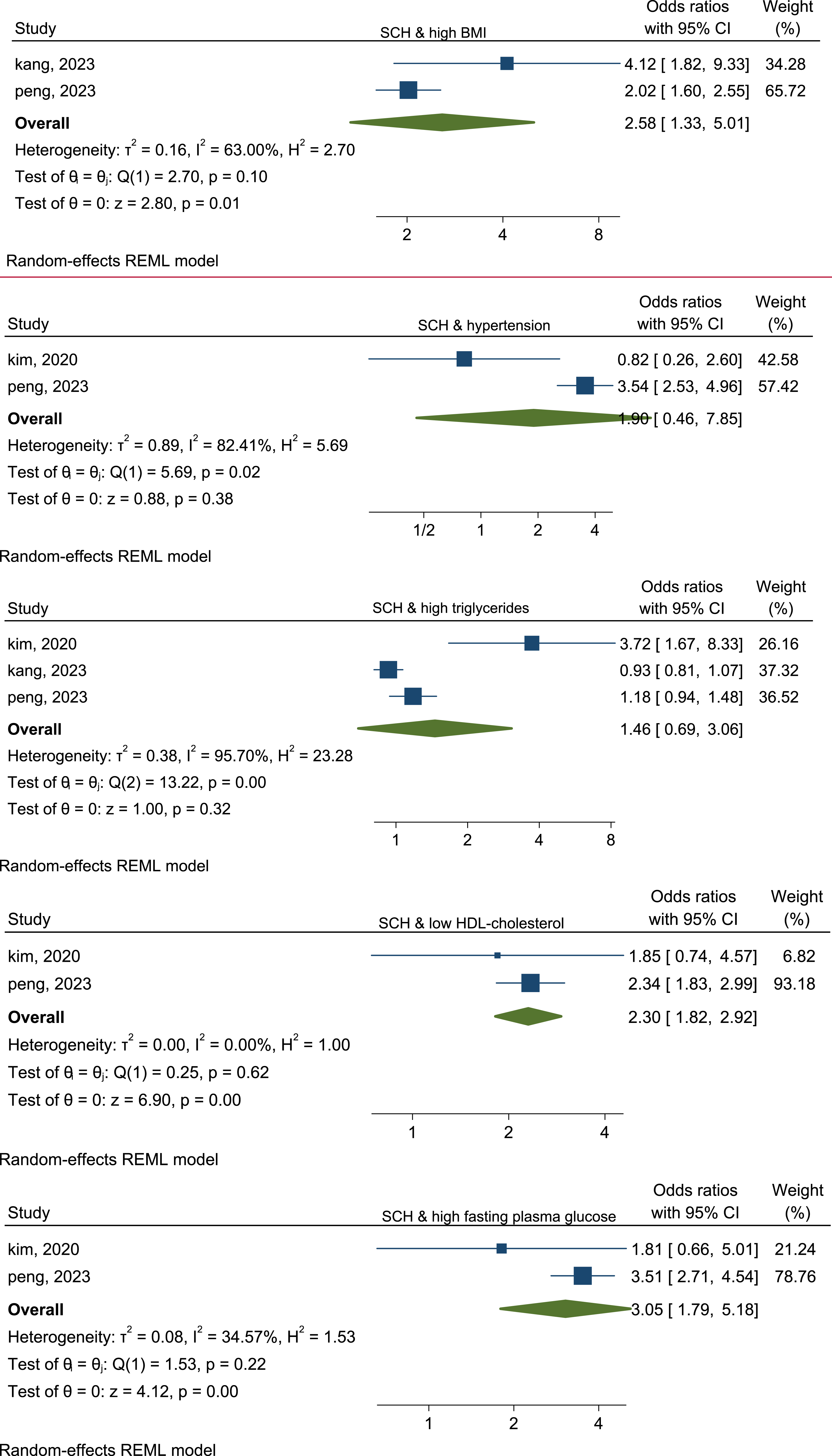
A sensitivity analysis was conducted among two studies which investigated only MDD and excluded Li et al. 13 Li et al. examined the association between SCH and MetS in MDD and anxiety disorders. SCH seemed to increase the odds of MetS in people with MDD approximately five-fold (OR = 5.01, 95% CI: 3.81–6.59).
Discussion
This systematic review of five cross-sectional studies investigated the association between SCH and MetS among psychiatric patients. A meta-analysis was conducted on three studies on MetS in people with MDD and anxiety disorders with concurrent SCH.
Major psychiatric disorders included in the literature search were schizophrenia, psychosis, depression, mania, anxiety and bipolar affective disorders. However, all included articles in the review focused on depression and anxiety disorders. Interestingly, no studies examined the association between SCH and MetS in other major psychiatric disorders, schizophrenia and bipolar disorders.
This review showed that SCH increased the likelihood of MetS around three-fold in people with MDD and anxiety disorders compared to the group who did not have SCH. After removing the study on participants with anxiety, the odds of MetS rose around five-fold in MDD patients only. This result was relatively higher compared to a previous meta-analysis on the non-psychiatric population with SCH, where the OR of MetS was 1.28. 14 The co-occurrence between MDD, anxiety, SCH and MetS suggests possible pathological overlap, which may amplify the risk of MetS. The common pathological processes include an HPA axis, inflammatory activation and autoimmune conditions.15–19 Besides, psychotropic medication, unhealthy life-style, and substance use contributed to a higher risk of MetS in MDD.15–19
Greater severity of depressive symptoms, higher BMI and lipid disorders were associated with SCH and reported in several studies.20,21 A recent meta-analysis observed a positive association between obesity and depression. 22 The association between SCH, MetS and depression could be explained by the likelihood of MetS amplified in people with depression and comorbid SCH. This effect was observed by Peng et al., which showed a positive association between MetS and suicide attempts, anxiety and psychotic symptoms in people who had SCH. 12 Similarly, more prolonged depressive illness duration and severe depressive and psychotic symptoms were closely associated with SCH. 11
The meta-analysis demonstrated that SCH was associated with high likelihood of all five components of MetS: high BMI, hypertension, high TG-C, low HDL-C and high FPG levels. SCH was significantly associated with a two-fold increase in the odds of high BMI and low HDL-C and a three-fold increase in the odds of high FPG. These results were similar to previous studies suggesting that SCH was associated with obesity, high TG-C and low HDL-C in the non-psychiatric population.23–25
The odds of each MetS component in MDD and anxiety in our study were relatively higher than a meta-analysis conducted on 79,727 non-psychiatric individuals, which observed that SCH had a significant positive association with central obesity, hypertension, high TG-C and low HDL-C. 14
The risk of MetS in SCH seemed to differ with variations in age, ethnicity, sex and their definition criteria. The risk of SCH increases with age. 26 All included studies were undertaken in Asia, which could increase the risk of SCH due to their iodine-rich diet. The higher prevalence of SCH among females in included studies could be explained that females were more susceptible to develop SCH than males, particularly those with MDD and anxiety disorders,9–12 mood disorders, 1 and in the non-psychiatric population.2,27
Among the included five studies, participants in two studies were first episode drug-naïve individuals with MDD.11,12 This could have minimised the potential confounding effects of SCH and MetS, like the effects of psychotropic medications and duration of depressive illness.
Given that MetS is a multifactorial disorder, the link between SCH and MetS could be confounded by other factors if potential variables were not properly adjusted. All included studies adjusted age, gender, education and marital status. Most studies did not adequately address potential confounders like life-style factors11,12 such as exercise, diet or smoking and medication history. Adjusting these variables might have affected the meta-analysis findings, which might indicate that findings were not true reflections of the actual relationship between SCH and MetS.
Since TSH vary by time of the day and from day-to-day and laboratory-to-laboratory, it is important to obtain repeated measurements to diagnose SCH. However, the diagnosis of SCH was made in all included studies based on a single reading of thyroid hormone level. This may result in a misclassification bias. Thus, these findings warrant further large prospective, longitudinal study considering serial assessments of thyroid hormone levels and MetS outcomes with confounding factors adjustments to clarify the causal relationship between SCH and MetS among the psychiatric population.
Several limitations should be considered. The findings could have limited generalisability to other psychiatric populations with major psychiatric disorders and the psychiatric population from other regions because all studies were conducted among individuals with MDD and anxiety disorders and the East Asian population. All studies were cross-sectional, with no serum TSH and T4 levels before the onset of MetS. Hence, the causality of both SCH and MetS conditions could not be ascertained. Likewise, the thyroid function of the population in the studies before the onset of depression was unknown, making it difficult to clarify whether SCH precedes the occurrence of depression or occurs as a consequence of depression.
Publication bias might exist due to small number of included studies and exclusion of non-English or unpublished journals.
Substantial heterogeneity was observed in the included studies when analysing MetS and its components. This could be the combinations of various diagnostic criteria used for MetS and MDD, concomitant medication use, a wider age range of participants, onsets of MDD and SCH, substance use and anti-thyroid antibodies. Utilising other assessment tools rather than DSM-IV for the diagnosis of MDD and anxiety may result in a misclassification bias10,13 Lastly, we acknowledged the cautious interpretation of meta-analysis results due to probable limitations of the random-effects model for the meta-analysis with a small number of studies.
Regarding the strengths, this study is the first systematic review and meta-analysis examining the association of MetS in people with major psychiatric disorders who had concurrent SCH compared to those without SCH. Following the PRISMA guidelines, it included a comprehensive search strategy with broader search terms that captured the most relevant studies.
This review highlighted the impact of SCH on metabolic parameters in depression and anxiety disorders. These findings suggested the importance of early screening and preventive measures for MetS and SCH in people with MDD and anxiety disorders. The link between thyroid and mood disorders has been recognised for many years, 28 with evidence that hypothyroidism and SCH were associated with poorer response to antidepressants and mood stabilisers in bipolar patients.1,29,30 Currently, no national guidelines exist for screening SCH in the psychiatric population, despite the link between SCH and MetS. The risk of developing overt hypothyroidism from SCH was eight-fold if either the thyroid peroxidase (TPO) antibody was positive or serum TSH levels were over 2mIU/L.26 Therefore, current clinical practice for thyroid screening tests among people with SCH should include TPO antibodies besides serum TSH and FT4 levels. This review’s findings will inform clinicians about the clinical implications of MetS in people with MDD and anxiety disorder who have concurrent SCH. This review gave insight into the importance of early diagnosis and treatment for SCH and MetS in psychiatric patients. Specifically, these findings suggest regular assessment of thyroid function, and screening of SCH could be useful in detecting MetS early in psychiatric patients.
Conclusions
This systematic review included a total of five studies. The meta-analysis suggested the likelihood of MetS increased around three-fold in people with MDD and anxiety disorder who had SCH compared to those without SCH. The likelihood of MetS in MDD patients with SCH was higher, with a five-fold increase. SCH was positively associated with high BMI, hypertension, high TG-C, low HDL-C, and high FPG levels in MDD and anxiety disorders. However, these results were based on limited single-centred, retrospective cross-sectional studies. The review findings did not inform the causality of observed associations.
Supplemental Material
Supplemental Material - Subclinical hypothyroidism and metabolic syndrome in psychiatric patients; A systematic literature review and meta-analysis
Supplemental Material for Subclinical hypothyroidism and metabolic syndrome in psychiatric patients; A systematic literature review and meta-analysis by The The Aung, Win Wah, Arnob Chakraborti, Vikas Garg in Australasian Psychiatry
Footnotes
Acknowledgements
This research project was conducted as the scholarly project of the RANZCP (Royal Australian and New Zealand College of Psychiatrists) Fellowship Program
Author contribution
TTA; Conceptualisation, data extraction, quality assessment, validation, writing-original draft, writing-review and editing, WW; Methodology, data analysis, validation, writing-review and editing, AC; Data extraction, quality assessment and validation, VG; Data extraction, quality assessment and validation.
Disclosure
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no funding.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.