
Abstract
Dear Editor,
Almost anyone who attends academic conferences or reads published research in paediatric transgender healthcare will be familiar with what I refer to as The Graph. Internationally replicated, these plots depict increasing paediatric gender referrals,1,2 levelling off in the most recent years. I have published the same, reporting work conducted while employed at the Perth Children’s Hospital Gender Diversity Service in Western Australia. 3
Reading Amos (2024), 4 I noted that WA data did not follow this previously observed trend. Despite a core argument of this paper stating that services are being increasingly accessed, the clear departure of the WA data from this pattern was curiously not commented upon.
Upon closer reading, I identified that these were not referral numbers but client numbers, without further definition. For services with long waiting lists and extensive assessment periods, a client could be defined as any combination of: a) newly referred patients; b) existing referrals awaiting an appointment; c) families who received triage contact and/or information, waiting for assessment; d) patients ‘activated’ formally on administrative systems (usually undergoing assessment or treatment); e) patients undergoing assessment; and f) patients receiving gender-affirming medical treatments and ongoing monitoring.
The raw data, provided directly by Dr Amos to myself upon request, included the exact wording of the responses to FOI requests, which form the basis of the data reported. Examining the FOI responses, it seems client is undefined in Amos (2024) because the label has been applied to different patient groups, both between clinics and sometimes year-to-year within the same clinic.
While this problem pervades the entire data set, this is most strikingly illustrated in the sawtooth pattern evident for WA clients, which does not reflect referral or treatment trends but rather different patient groups collated under a single label (Table 1). Inferring trends or comparing these data is inaccurate at best and actively misleading at worst. Documentation included in FOI responses also indicates the MP submitting FOIs has known about the ambiguity surrounding the clients request since at least 2018.
Examining the raw data, other challenges to accurate data harmonisation are evident. A comprehensive account of data discrepancies is beyond this comment’s scope but includes inconsistent time periods (i.e. snapshot at a single date, over calendar year, or 12-month histories [September to September]); differing staff disciplines described in FTE (e.g. some clinics including non-clinical research or admin staff); unclear inclusion of filled versus unfilled FTE; and in one case (SCHN [NSW] 2019 FTE), data was provided in the FOI response but not reported in the paper.
It is important to note that authors analysing and reporting data collected by others, including via FOI request, typically have little control over the content or quality of data provided. However, these authors do have an ethical responsibility to ensure their reporting of data meets data integrity and accuracy standards. 5 Dr Amos rightly noted, for example, where FOI responses specified total treatment versus treatment initiation rates (the latter seemingly requested in some cases). However, other pertinent details including the operationalisation of the request for ‘clients’ in the absence of more specific definitions, or the time period of statistics reported, are also important factors in ensuring the accurate and transparent reporting of data.
Relatedly, Dr Amos has claimed he aimed to demonstrate the insufficiency of data availability. Yet, analysis of missing data is overshadowed by Dr Amos’ interpretation of available data. The conclusions stated in the abstract and the paper are not limited to data availability or quality but instead make specific statements on trends as if the data were accurate and reliable. Patterns in this flawed data – not the availability of data – have already been referenced by activists seeking to restrict gender-affirming healthcare in Australia. 6
Patient groups included in ‘clients’, as specified in WA FOI request responses
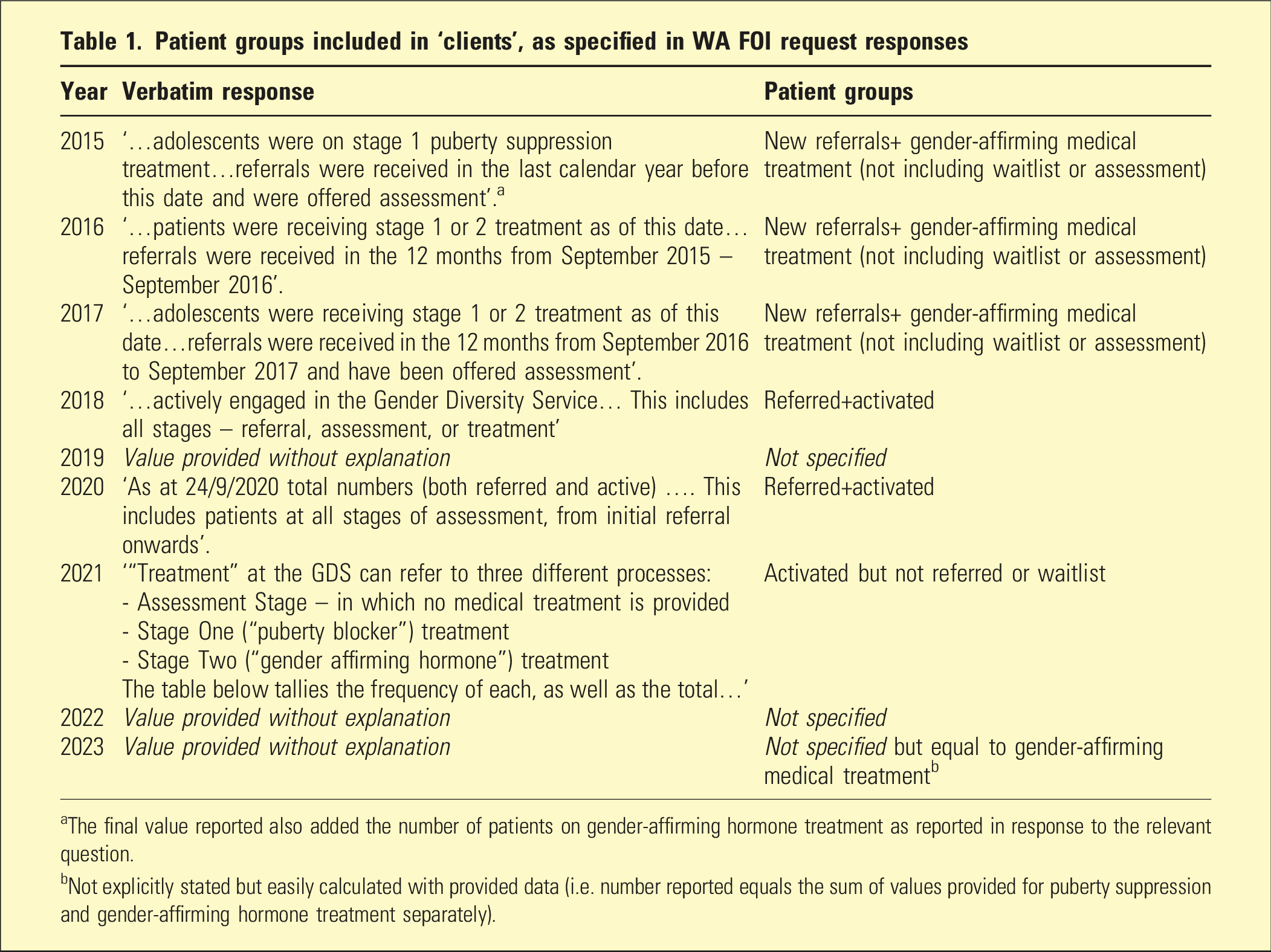
aThe final value reported also added the number of patients on gender-affirming hormone treatment as reported in response to the relevant question.
bNot explicitly stated but easily calculated with provided data (i.e. number reported equals the sum of values provided for puberty suppression and gender-affirming hormone treatment separately).
Footnotes
Declaration of conflicting interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: BC discloses previous employment with the Perth Children’s Hospital Gender Diversity Service and ongoing research collaborations with the paediatric gender clinics discussed in the original article. BC declares membership to the Australian Professional Association for Trans Health and the World Professional Association for Transgender Health.
Data availability statement
Data discussed in this correspondence article is available directly from the original article author.