
Abstract
Objective
To conduct a quality assurance study assessing the implementation of the Healthy Ageing Service Wellbeing Skills Group Program (HAS-WSGP), a novel psychosocial skills group designed to support older adults’ mental health.
Methods
Eligible participants were aged 65 years or older, presenting with mild-moderate mental health symptoms or interested in learning skills to enhance their emotional wellbeing, and living in community and residential aged care settings. Sessions were conducted weekly and facilitated by mental health clinicians and a peer support worker. Data collection involved a combination of demographic variables, outcome measures, and feedback surveys.
Results
A total of 40 consumers participated in the HAS-WSGP during the study period. Overall, participants demonstrated improvements in psychiatric, social, and occupational functioning, however no improvements in depressive and anxiety symptoms were observed. Improvements in self-reported knowledge of group program topics were observed, and participants endorsed the program as relevant, supportive, and helpful for improving their overall wellbeing.
Conclusions
It is feasible to run a psychosocial group program with older adults, and older adults report good benefits from this form of service provision. Further research will be needed to determine the efficacy of these programs on improving older adults’ mental health.
The experience of loneliness and mental health symptoms in older adults is common, and further exacerbated with increasing age and for those living in residential aged care (RAC). 1 For example, in Australia, 16% of community dwelling older adults, and 61% of individuals living in RAC experience loneliness.2,3 Approximately 8% of community dwelling older adults experience depression, and an analysis by the Australian Government of people entering RAC from 2017 to 2022 revealed that 62.5% of new residents presented with at least mild symptoms of depression on admission.4,5 Anxiety has been studied less widely in older adults, however estimates from the National Study of Mental Health and Wellbeing report that for older adults (aged 65-85 years), the prevalence of anxiety disorders (any type) ranges from 4%–6.3% for men and 5.5%–10.9% for women. 6 Meanwhile, in RAC, it is reported that over 52% of residents experience symptoms of anxiety. 5
As Australia’s population ages, providing appropriate and effective mental health and wellbeing support for older adults, particularly those in the RAC setting (which historically has had limited access to mental health services), has therefore become an important health issue.7,8 The Australian government has also recognised this, with the Primary Health Networks (PHNs) commissioning the development of psychological treatment services for RAC residents (‘Improved Access to Psychological Services in Aged Care Facilities Initiative’).8,9 In this context, the Eastern Melbourne PHN commissioned St Vincent’s Hospital Melbourne (SVHM) to deliver the Mental Health and Primary Care Partnership pilot and subsequent Healthy Ageing Service (HAS).10,11 HAS is a multi-disciplinary outreach mental health service developed to support the mental health of older adults who need more than primary mental health support, but do not meet referral criteria to access tertiary level support. 11
Aiming to further increase access to mental health support; with a strong focus on health promotion and early intervention, HAS set out to develop a psychosocial group program. While there is a paucity of research on the effectiveness of therapeutic group programs in older adults, some supportive literature does exist. For example, a systematic review of group psychotherapy programs for older adults found that it was a feasible and effective treatment approach for late life depression. 12 In a feasibility study focused on group-based Acceptance and Commitment Therapy (ACT) for older adult veterans, participants reported satisfaction with the group format, with low rates of early termination and consistent attendance suggesting a general receptiveness among participants. 13 Group-based psychosocial programs have also been found to decrease risk of perceived loneliness and social isolation in older adults. 14
Community mental health services may be uniquely suited to provide group program support to older adults as they have close connections to the communities they serve, and are equipped to address psychosocial stressors unique to older adults. 15 Engaging community mental health consumers in evidence-based, effective short-term group interventions may also be more time and cost effective for these services.
Working within the HAS brief intervention model of care, a Clinical Psychologist, Occupational Therapist, Mental Health Nurse, Peer Support Worker and Psychiatrist collaborated to develop and deliver the HAS-Wellbeing Skills Group Program (HAS-WSGP). No additional funding was sought for the development and implementation of the intervention. The aim of this project was to conduct a quality assurance study to review the implementation of the HAS-WSGP.
Methods
Participants and referrals
Consumers were eligible for the HAS-WSGP if they met the following criteria: current consumer of HAS (i.e. aged 65 years or older (or may be younger with age-related illness), dwelling in community or RAC, and experiencing mild-moderate mental health symptoms), or older adults interested in learning skills to enhance their emotional wellbeing.
The HAS-WSGP was promoted to health and clinical services, community organisations (e.g. neighbourhood houses, libraries, local community centres), local government councils, and RAC facilities (RACFs). Consumers could self-refer to the HAS-WSGP, or be referred to the group program, or be referred by their HAS clinician or an external healthcare provider.
Group program design and structure
The HAS-WSGP focused on teaching participants a range of evidence-based psychological skills to promote emotional wellbeing. The strategies were grounded in principles of Cognitive Behavioural Therapy (CBT), ACT, and Compassion Focused Therapy (CFT). The group engaged consumers through psychoeducation, skills practice, and an opportunity for questions, reflection and group discussion in each session. A bespoke workbook provided relevant psychoeducational material. At the end of the program, consumers had the opportunity to develop an individualised wellbeing plan based on the strategies learnt. Sessions were conducted weekly for 1 hour in a closed group setting. Session topics are depicted in Figure 1. Groups were facilitated by at least two HAS clinicians (Clinical Psychologist, Occupational Therapist) and a Peer Support Worker. HAS-WSGP session topics.
Data collection and analysis
Data collection included demographic variables, outcome measures, and pre- and post-feedback surveys, all of which are routinely collected at intake and discharge as part of a consumer’s clinical care and engagement with HAS.
Demographic variables
Information on age and gender was obtained prior to the group program.
Outcome measures
Key outcome measures included the Kessler 10 (K10), 16 a measure of psychological distress; The Health of the Nation Outcome Scales 65+ (HoNOS 65+), 17 a measure of psychiatric symptoms and impact on functioning, and the Social and Occupational Functioning Assessment Scale (SOFAS), a measure of overall functioning. 18
Participant pre- and post-group program feedback survey
The pre- and post-group program feedback survey assessed: self-reported rating of knowledge on program topics, general session feedback, barriers to participation, and ideas for improvement. The survey included Likert scales and free text response options.
Facilitator feedback
Facilitators completed a written reflection after each group session, providing free text responses identifying aspects of the group session that went well, and ideas for improvement.
Process measures
Process measures included: group location, number of sessions attended, and reasons for non-attendance.
Data analysis
Data were imported into Microsoft Excel and the Statistical Package for Social Sciences (SPSS V29) for analysis. Descriptive statistics and frequencies were used to evaluate demographics, process measures and data from the feedback survey. Wilcoxon signed-rank tests were conducted to compare pre- and post-group outcome data and self-reported topic knowledge as assessed by the feedback survey. Non-parametric tests were utilised as normality testing revealed that outcome measure and feedback survey data was skewed. Missing data were excluded from the analyses.
Ethical approval
Ethical approval was received from the Hospital’s Human Research Ethics Committee and Research Governance Unit. Participant consent was not required as this study was a retrospective quality assurance project using de-identified data obtained in routine clinical practice.
Results
Participants
Seven groups were completed between June 2022 to October 2023, and 40 consumers participated. Most participants (82.5%) were female (17.5% male), with an average age of 77 years (range 6-91 years; SD = 7.2).
Group location
Approximately two-thirds of the sessions were delivered in community settings (62.5%), with one-third in RACFs (37.5%). Most (72.5%) of the sessions were delivered face-to-face, and one-third (27.5%) delivered via telehealth.
Group duration and attendance
Attendance rates
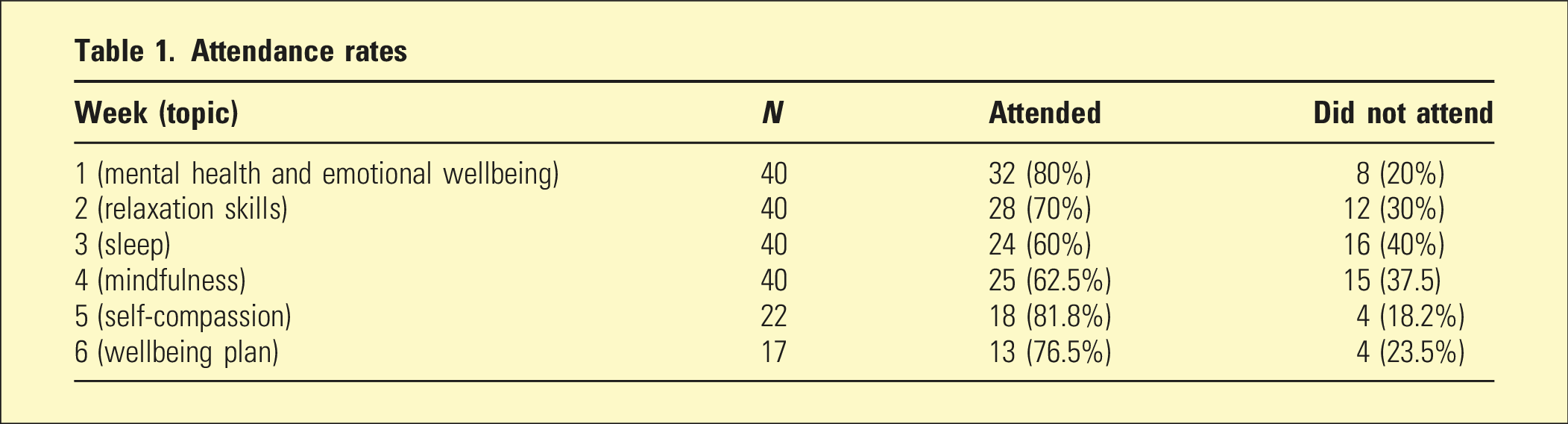
Common reasons for non-attendance (n = 14) included: schedule conflicts, illness, caring duties, and withdrawal from the group program.
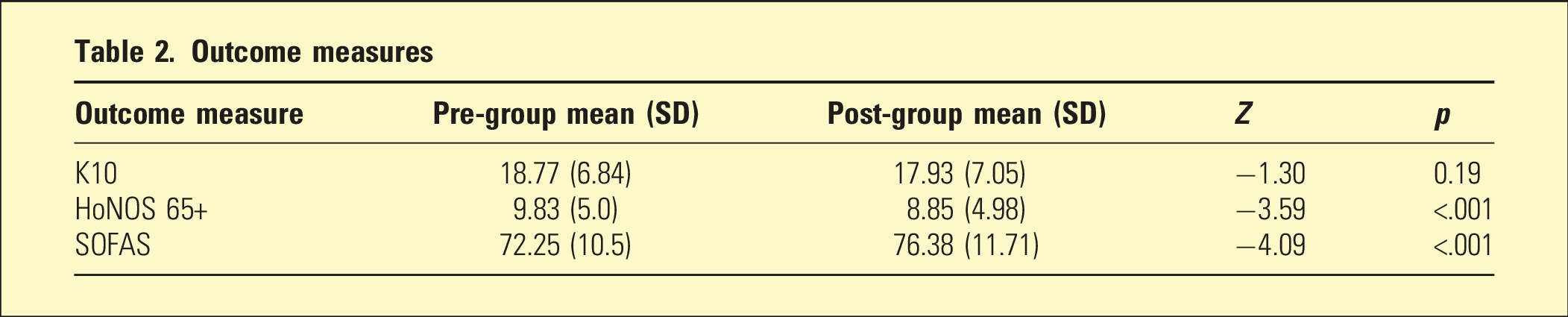
Outcome measures
Outcome measures
Feedback survey results
A total of 37 consumers completed the pre-group survey, and 21 consumers completed the post-group survey.
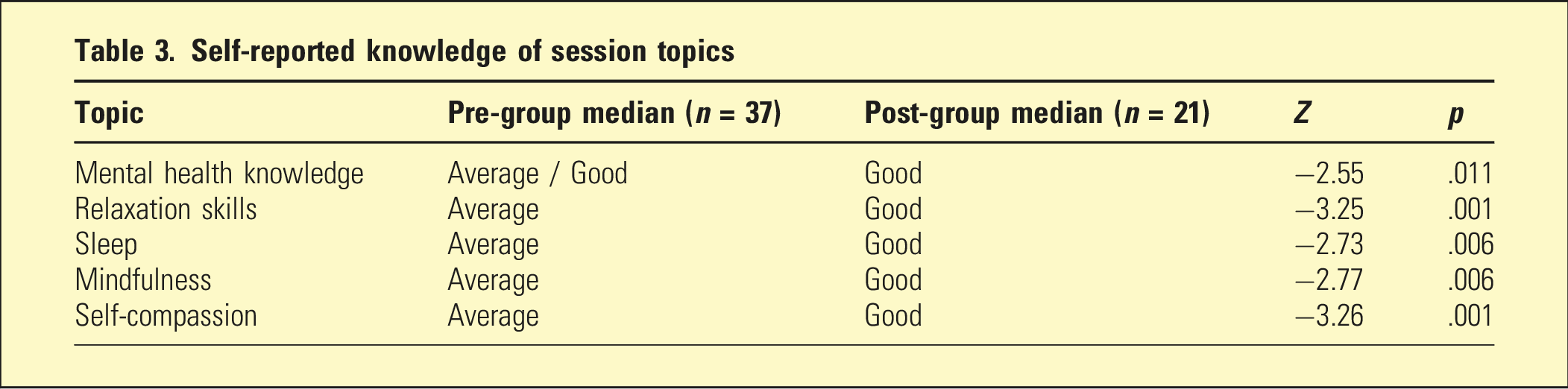
Knowledge of session topics
Self-reported knowledge of session topics
Overall program feedback
A large proportion of post-group survey respondents ‘strongly agreed’ that the sessions were relevant and met their expectations (76.2%), and that the facilitators were supportive and helpful (95.2%). Around two-thirds of respondents (66.7%) ‘strongly agreed’ that they had gained new knowledge to improve their wellbeing as a result of participating in the group program and that they felt they could implement their learnings into everyday life (61.9%). Almost all respondents (90.5%) reported enjoying the group program, and a similar number (95.2%) reported they would recommend the group to others.
When asked what went well in the program, participants reported appreciating the opportunity to be part of a group, to receive psychoeducation, and enjoying the engagement in conversation. Participants endorsed the sleep and relaxation topics as being the most interesting and beneficial to their wellbeing.
Barriers to participation
Common barriers to participating in the group program described by participants included: concerns about confidentiality, and issues with scheduling (e.g. group session time coinciding with other lifestyle activities in the RACF setting).
Areas for improvement
Common areas for improvement reported by participants included: longer group duration (more than 6 weeks), longer session duration (e.g. 1.5 hours as opposed to 1 hour), and preference for face-to-face sessions (for those participating via telehealth).
Facilitator feedback
When reflecting on aspects of the program that went well, facilitators reported that the use of audio-visual resources (e.g. YouTube videos and audio clips) were helpful in delivering session content (in addition to the workbook). They reported that sessions were timed well, and most participants were readily able to access telehealth platforms to attend the group, either by themselves or with support. Facilitators reported that the participants enjoyed being in a group setting, and engaged well with others, however found that in-person sessions were more engaging than online sessions.
Reflecting on aspects of the group that could be improved, facilitators suggested that including more directive tasks may facilitate conversation and engagement. They also reported that including strategies for consumers who have less functional capacity (e.g. are bed- or chair-bound) or medical comorbidities that impact their ability to complete some of the wellbeing skills (e.g. progressive muscle relaxation), may be helpful to make the program more inclusive. In addition, considering alternative methods of communicating the contents of the workbook for those with sensory impairments may be useful. Lastly, it was suggested that the group program may benefit from better recruitment strategies to increase participation.
Discussion
To our knowledge, this is one of the first psychosocial skills groups to be implemented with older adults in both community and residential aged care settings in Australia. The use of multi-modal service delivery also aimed to mitigate common barriers to accessing mental health services for older adults such as mobility and transportation issues, supporting accessibility and inclusivity of the program. Overall, participants demonstrated an improvement in psychiatric symptoms and functioning, consistent with previous research suggesting that group therapy programs may support or improve the psychosocial wellbeing of older adults.19–21 The Australian Government Evaluation of the PHNs’ Improved Access to Psychological Services in Aged Care Facilities Initiative had largely positive findings and recommended continuation and expansion of services. Although PHNs included group interventions, the evaluation found that ‘services have primarily comprised individual sessions’. 8 The outcome and qualitative data from our experience and evaluation is thus useful to other service providers aiming to deliver group interventions.
Our results failed to show any significant changes in depressive and anxiety symptoms as assessed by the K10, contrasting with other studies which have shown improvements in depressive and anxiety symptoms among older adults following participation in a group program.22–24 This may be attributable to some inconsistencies with the administration of the outcome measures (some participants self-reported their K10, whilst others had clinician-rated K10s). Self-reporting may have resulted in an underestimation of symptoms at both baseline and follow-up, as older adults are less likely to endorse or report mental health symptoms. 24 In addition, the presence of cognitive impairment, which was not an exclusion criterion for participating in the group program, may have impacted a participant’s ability to accurately recall or report their mood symptoms.
Interestingly, the great majority of female participants (82.5%) likely reflects the higher proportion of older females in RACFs, as well as their greater acceptance of mental health support when compared to men.25,26 Additionally, age effects are also reported for men who attend psychotherapy (with younger men more likely to initiate access to psychological support when compared to older men). 27 While this suggests that more consideration may need to be given in how to best engage men in accessing programs such as HAS-WSGP, this exploration was not within the scope of work for this project.
Our findings suggest that a group program is a useful and feasible method of mental health service delivery for older adults. Participants attended the group sessions fairly consistently, and feedback indicated that participants would prefer longer sessions over a longer time period. Furthermore, the majority of participants endorsed the group as relevant, helpful, supportive and enjoyable. Facilitators’ observations also highlighted that participants enjoyed the group setting.
However, there are several other limitations worth noting. Firstly, collection of additional demographic information (e.g. socioeconomic status, primary language, psychiatric diagnoses and medications, and engagement in psychotherapy) may help determine generalisability of the intervention, and identify characteristics that facilitate engagement and improvement in mental health symptoms. While the heterogeneity of our sample may have contributed to variability in outcomes, it also highlights the program’s inclusivity and broad applicability given this was a real-world clinical service sample with few exclusions. However, due to limited demographic data, we could not fully characterise the sample or explore subgroup differences. Future studies should prioritise collecting detailed demographic information to better understand how individual characteristics influence program outcomes without compromising inclusivity.
Also, the group program took place in multiple settings and formats. It may have been useful to compare results between groups, to determine if the environment and delivery method impacted participants’ experience of the group. Unfortunately, in this study, the small sample size did not allow for these analyses. Further to this, interpretation of our outcome data must be considered cautiously due to the small sample size. More research is needed with larger sample sizes in order to determine whether a psychosocial intervention such as the HAS-WSGP is effective.
In addition, as this was a quality assurance study, the outcome measures used were opportunistic based on usual data collected by the clinical service. This may have limited the capacity of this study to effectively measure the effects of the intervention. Future studies should therefore consider using outcome measures that are designed specifically to assess variables of interest such as depressive and anxiety symptoms, and loneliness in older age.
Lastly, it may also have been useful to include a screening measure of cognition. This data may be used to determine whether cognitive impairment limited the participant’s engagement or ability to benefit from the group program, (and subsequent tailoring of the program).
Conclusion
Whilst demand for mental health services is increasing, there are limited services available to older adults, particularly for those living in residential aged care. This study shows that it is feasible to deliver a group program to this cohort, who benefit from this form of service provision. Group programs may therefore be an efficient and scalable way of increasing an organisations’ capacity to provide mental health services. Further research will be needed to determine the efficacy of these programs on improving older adults’ mental health and addressing an area of significant unmet need.
Footnotes
Acknowledgements
The authors would like to thank all of the consumers, carers, and referrers who have contributed to the development and ongoing improvement of the Healthy Ageing Service. We are also grateful for all current and previous staff and Eastern Melbourne Primary Health Network for their partnership with us in commissioning and funding this service.
Disclosure
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: S Perin, G Billing, and T Chong were responsible for development of the Wellbeing Skills Group Program. S Perin, G Billing, and J McCurry were responsible for the implementation and delivery of the Wellbeing Skills Group Program. T Cottrell is the Healthy Ageing Service manager, and G Billing is the Healthy Ageing Service team leader. No other conflicts of interest to disclose. The authors alone are responsible for the content and writing of this paper.
Funding
The Healthy Ageing Service is funded by Eastern Melbourne Primary Health Network. The author(s) received no financial support for the research, authorship, and/or publication of this article.