
Abstract
Objective
Use of seclusion (in particular inequitable use) continues in mental health services in many countries, despite evidence against it and substantial endeavour to reduce or eliminate it. Aotearoa New Zealand’s national quality improvement agency Te Tāhū Hauora Health Quality & Safety Commission has since 2018 led a project to eliminate use of seclusion in mental health inpatient units.
Method
The ‘Zero Seclusion: Safety and dignity for all’ project co-designed a bicultural change package and implemented it nationwide in a formative collaborative with clinical teams, consumers, families, and whānau. Outcome measures included seclusion rates, duration, and average number of episodes, by ethnicity, with a focus on equity.
Results
From a baseline mean of 6.4% of mental health service consumers secluded monthly in the 12 months to September 2019, the mean rate of seclusion reduced to 4.3% by June 2024. The seclusion rate of Māori mental health service consumers fell from 9.9% to 6.0%, and of non-Māori/non-Pacific consumers from 4.0% to 2.3%.
Conclusion
Reduction and elimination of seclusion, especially its inequitable use with indigenous populations, is possible. True co-design, strong leadership, partnership with indigenous populations and those most affected, and an embrace of robust measurement were critical to these good results.
Keywords
Seclusion is a form of coercive restrictive practice in mental healthcare settings, defined by Aotearoa New Zealand’s Ngā Paerewa Health and Disability Services Standard 2021 as ‘restraint where a person is placed alone in a room or area, at any time and for any duration, from which they cannot freely exit’. 1 It is incompatible with Article 14 of the United Nations Convention on the Rights of Persons with Disabilities, 2 and the United Nations Convention against Torture and other Cruel, Inhuman or Degrading Treatment or Punishment. 3 It is a practice physically and psychologically harmful to consumers of mental health services (consumers), and to those who care for them.4,5
Use of seclusion, however, continues in mental health services in many countries, despite the evidence against it and substantial endeavour to reduce or eliminate it.
Furthermore, ethnic disparities in use of seclusion and other restrictive practices have been identified globally.6,7 In Australia, people of Indigenous Aboriginal and Torres Strait Islander ethnicities experience seclusion at higher rates than other ethnicities.8–10 Both the Australian government alongside states and territory governments have made reduction or elimination of seclusion a priority, but with limited success.11–13
In Aotearoa New Zealand, seclusion and inequity for indigenous peoples is also a pressing and long-term issue. Māori represent only 17% of the population, 14 yet routine data analysis suggests in 2017 made up approximately 31% of all people admitted to adult inpatient facilities, and, compounding the inequity, 41% of Māori admitted experienced seclusion. Academic studies and ministry publications support the fact Māori were more likely to experience seclusion than other ethnicities.15–17 Reduction or elimination of seclusion both for Māori and all other New Zealanders had been a national priority, if unrealised, for many years.18–20
Many attribute the persistent inequitable health outcomes Māori face 21 to a systematic ‘cultural competence’ gap in services.22,23 Māori are signatories with the Crown in Aotearoa New Zealand to Te Tiriti o Waitangi (the Treaty of Waitangi 1840), which, with subsequent interpretation, provides principles for Māori partnership, active participation, tino rangatiratanga (self-determination), equity, and options, and this includes in healthcare. 24 Healthcare workers have been given the responsibility of upholding and aligning service processes and practices with Te Tiriti, and one solution to these persistent inequities has been to provide Māori consumers and their whānau better access to their own culturally informed models of care driven by their worldview knowledge systems and practices. 25 (Whānau is the smallest unit of Maori society; the individual is seen in the context of the whānau which is generally described as a collection of people connected through a common whakapapa (genealogy) or purpose. 26 ) This ideal of culturally informed models of care, alongside the principles above, has shaped the approach of the Zero Seclusion quality improvement project, 27 which has focused on inequity for Māori in use of seclusion using a co-designed bicultural approach.
As reported in this journal in 2023, 28 the Zero Seclusion project has been associated with a national reduction in the rate of seclusion for Māori from the August 2019 baseline to mid-2022.
Since then, this work has continued and developed. More recent data to June 2024 now show further reductions in seclusion rates both for Māori and for people of non-Māori/non-Pacific ethnicities.
Objective
Aotearoa New Zealand’s national quality improvement agency, Te Tāhū Hauora Health Quality & Safety Commission (Te Tāhū Hauora), leads work nationally to improve quality and safety across the health and disability system. One focus has been mental health services, and Te Tāhū Hauora’s national mental health and addiction quality improvement programme developed five priority areas of work with sector, clinical, and consumer guidance: 1. Zero seclusion: safety and dignity for all 2. Connecting care: improving service transitions 3. Learning from adverse events and consumer, family, and whānau experience 4. Maximising physical health 5. Improving medication management and prescribing
29
Since 2018, building on work begun in 2009 by Te Pou, known as the ‘six core strategies,’ 30 the Zero Seclusion project (the project) has, through co-design and quality improvement methodologies, supported district health services to find alternatives to seclusion, test these and measure efficacy, then implement successful changes at scale. A strong focus on rates of seclusion for Māori was developed in response to inequitable rates of seclusion, and in recognition of Te Tiriti o Waitangi rights of Māori to equity of treatment and outcomes.
Method
Critical elements of the project are Māori partnership in governance, strong leadership driving the work, true co-design, and collaborative testing of interventions.
Partnership in leadership and governance
The small national team guiding and overseeing the work is comprised of clinical, cultural, and consumer leadership with a senior respected Māori elder (known as a kaumātua). The project is supported by both a Māori advisory group and a consumer advisory group.
True co-design
‘True’ co-design in this context implies direct involvement in design of the project of those with lived experience, consumers, families and whānau. This direct involvement is established early in the problem definition and prioritisation stages of the work (known as ‘frontloading’ consumer engagement 31 ), as well as through the intervention design and testing stages.
Collaborative testing of interventions
In the reduction of seclusion practices, successful strategies are available in other contexts 32 and also in work locally by Te Pou. 30 However, no pre-existing ‘bundle,’ in the quality improvement sense, 33 of discrete, proven, evidence-based interventions existed, especially in the case of reducing seclusion rates of Māori. Therefore, consumers, families, and whānau were engaged in workshops with project teams, quality improvement experts in the national team and clinicians in all health districts to identify potential interventions to aid in reducing seclusion practices. Promising interventions were then tested using a ‘formative’ model of the Institute for Healthcare Improvement’s collaborative breakthrough series methodology. 34 This methodology provides a structure for organisations to collaborate on the selection, testing, and implementation of change in specific clinical areas where current practice deviates from best scientific knowledge, improved results would improve quality of care, and the possibility of improvement has been demonstrated by at least some sentinel organisations. 32
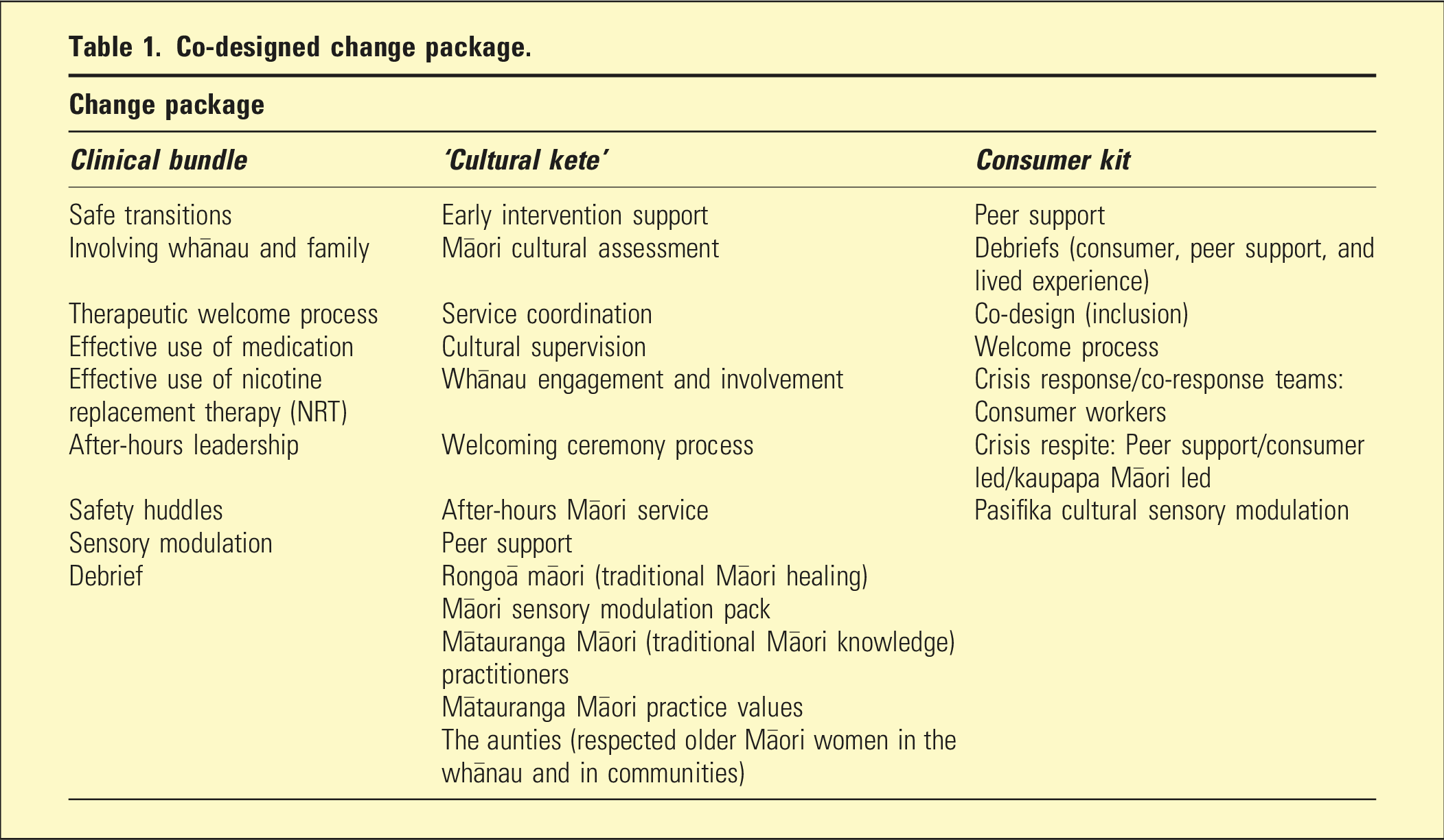
Through this process, a change package was developed, which included a clinical bundle, a ‘cultural kete’ (Māori for ‘basket’) and a ‘consumer kit’. 35 Each was informed by what limited evidence was available in the literature, and by change ideas demonstrated to be effective in the quality improvement testing phase of the work by project teams – thus known as a ‘formative’ collaborative. They were then reviewed and critiqued by relevant expert clinical, cultural, and lived experience advisory groups identified from across the national mental health and addiction sector. A comprehensive description of the change package is available, 35 but key elements developed and shown to be effective are listed briefly in Table 1.
Co-designed change package.
Measurement
Three outcome measures were selected to assess baselines for improvement in rates of seclusion in the 22 adult acute units (no rehabilitation units) in 19 of Aotearoa New Zealand’s 20 health districts. These measures were derived from data collected in Aotearoa New Zealand’s national mental health and addiction service data set, PRIMHD (Programme for the Integration of Mental Health Data),
36
which covers all publicly funded, inpatient-delivered mental health services including for people aged between 18 and 64 (those consumers in adult inpatient units). PRIMHD is an administrative data source not designed for our purposes, which is a limitation, but provides national data with demographic information. Outcome measures derived were as follows: • Rate of seclusion (percentage of inpatient mental health consumers who experienced any seclusion episode). • Average duration of seclusion experienced (per consumer). • Average number of episodes of seclusion (per consumer).
Each measure was analysed by ethnicity (Māori and non-Māori/non-Pacific). Baselines were derived from data for the period September 2018 to August 2019, when the project was in the set-up and co-design phase prior to testing of change ideas. In each measure, statistical process control techniques37,38 were used to assess for special-cause variation over time that was not attributable to chance.
Results
Mean monthly seclusion rates of both Māori and non-Māori/non-Pacific ethnicities, expressed as the percentage of all inpatient mental health consumers by month who are secluded, show significant shifts downward from baseline. From a baseline of 6.4% of all mental health service consumers secluded monthly in the 12 months to September 2019 the rate reduced to 4.3% sustained to June 2024 (see Figure 1).
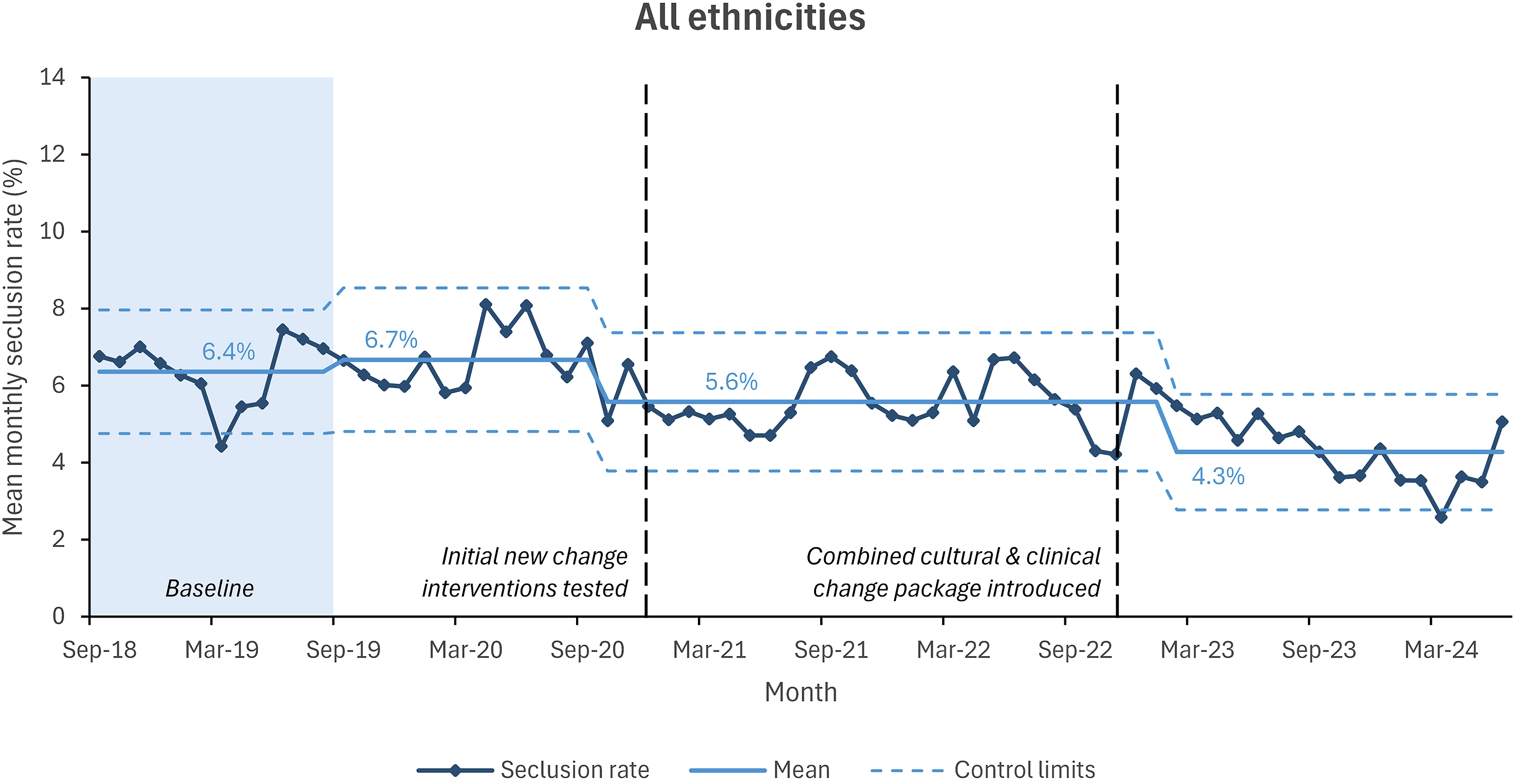
Seclusion rates for all consumers in adult, non-forensic inpatient mental health units, Aotearoa New Zealand, Sept 2018–June 2024. Note: graphs exclude Nelson-Marlborough and Southern districts due to changes in their IT systems and data collection during the project.
Step changes in the data are associated with significant events in the project’s evolution, such as when the refined cultural and clinical change package was introduced across mental health adult inpatient units in November 2022.
For Māori mental health service consumers, most inequitably affected by seclusion, the mean monthly rate of seclusion fell from 9.9% at baseline to 6.0% sustained to June 2024 (see Figure 2).
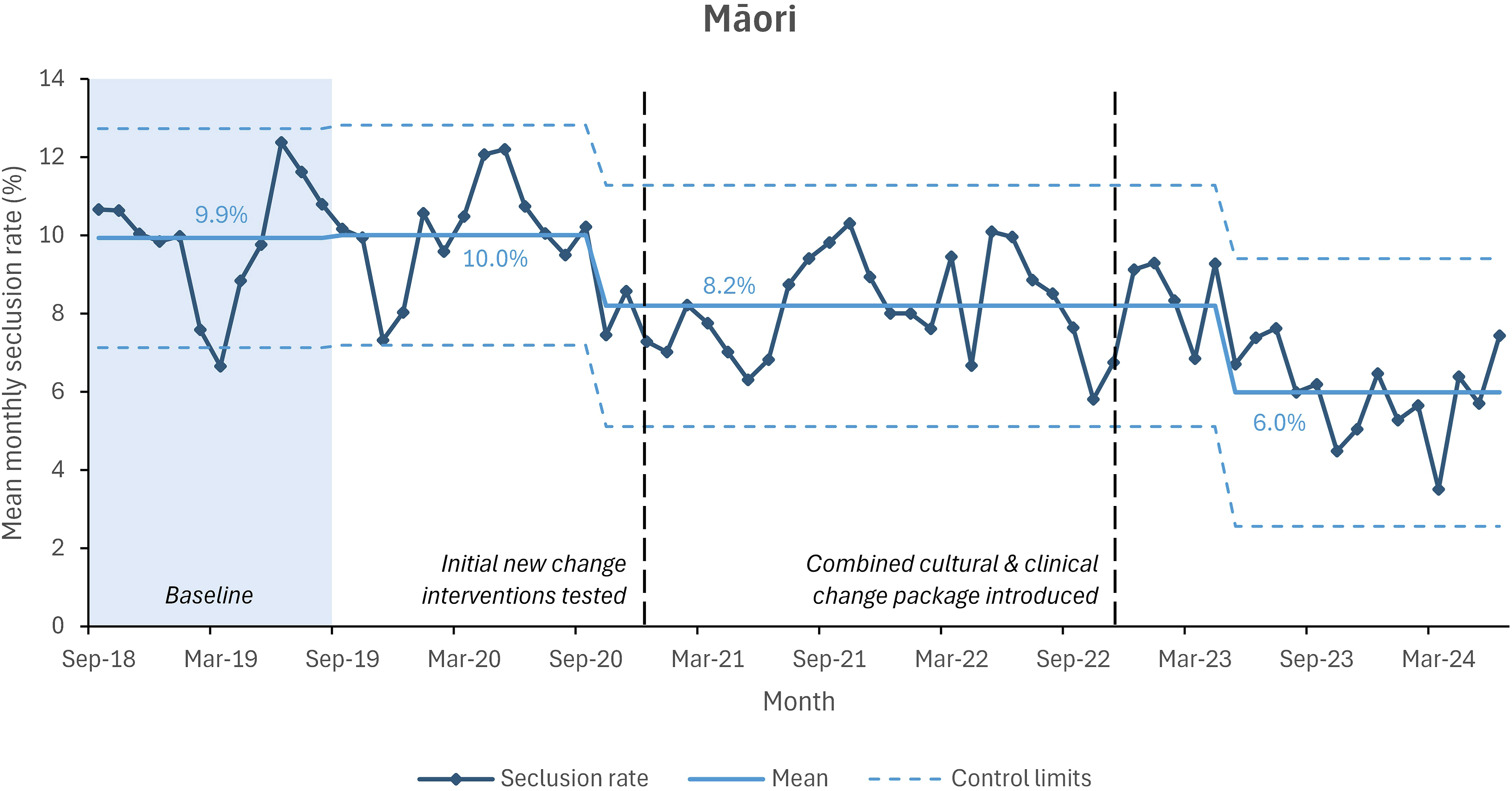
Seclusion rates for Māori consumers in adult, non-forensic mental health inpatient units, Aotearoa New Zealand, Sept 2018–June 2024. Note: graphs exclude Nelson-Marlborough and Southern districts due to changes in their IT systems and data collection during the project
For mental health service consumers of non-Māori/non-Pacific ethnicity, after a brief rise from baseline of 4.0% to 4.4%, the mean monthly rate of consumers secluded fell to 2.3% sustained to June 2024 (see Figure 3).
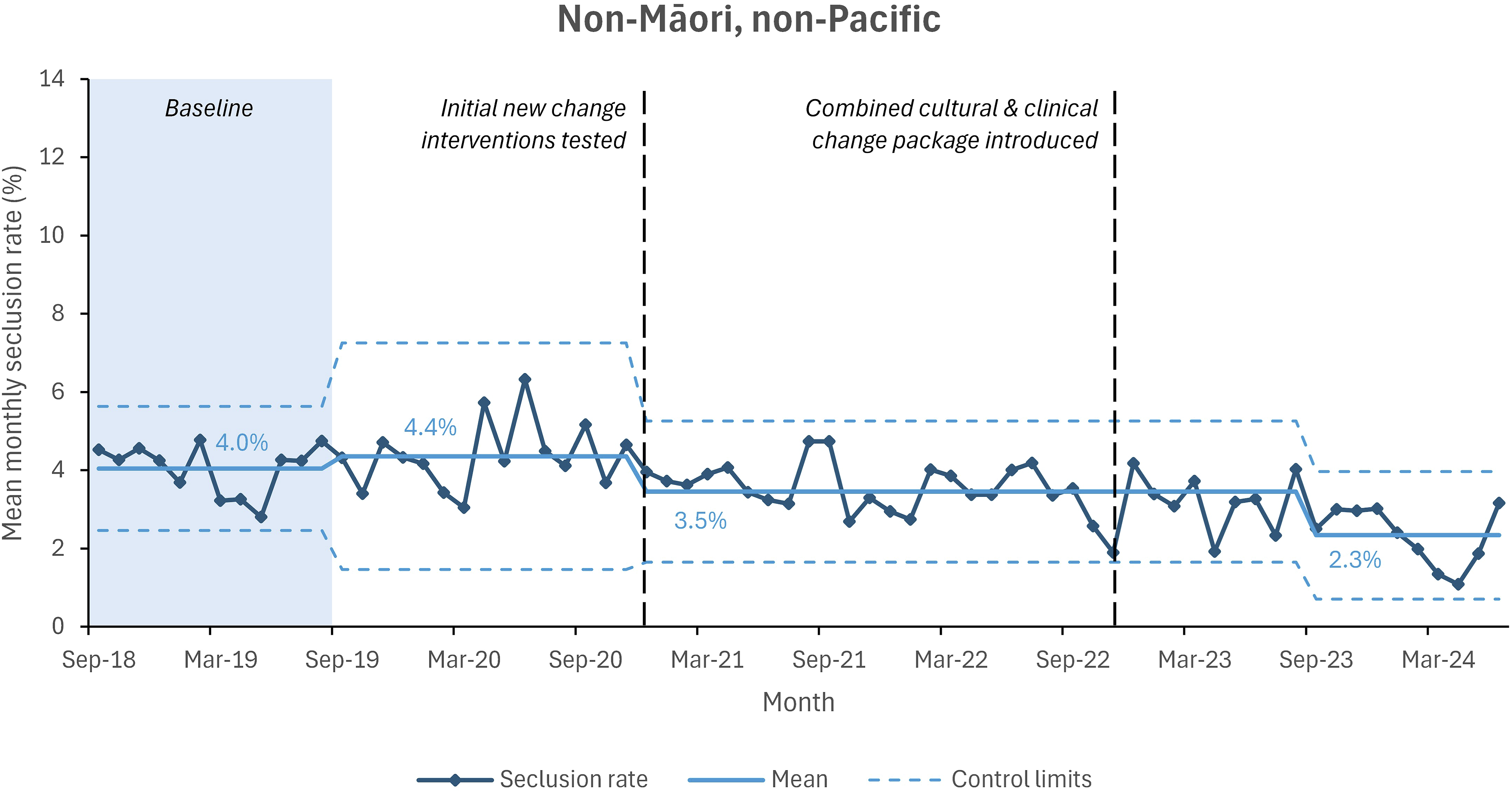
Seclusion rates for non-Māori/non-Pacific consumers in adult, non-forensic mental health inpatient units, Aotearoa New Zealand, Sept 2018–June 2024. Note: graphs exclude Nelson-Marlborough and Southern districts due to changes in their IT systems and data collection during the project
See the web supplement for further detail on additional results summarised below.
Monthly average duration of seclusion experienced fell from 2.5 hours for all ethnicities during baseline to 1.3 hours in April 2023, sustained to June 2024. For Māori, duration fell from 4.1 hours at baseline to 2.1 hours in the same period, and for non-Māori/non-Pacific, from 1.5 hours to 0.6 hours in September 2023.
The rate of monthly average number of episodes of seclusion (seclusion event rate, which counts seclusion events rather than people who were secluded) fell from 0.09 at baseline to 0.06 in April 2023, sustained to June 2024. For Māori, the seclusion event rate fell from 0.15 at baseline to 0.08 in September 2023, and for non-Māori/non-Pacific, from 0.06 to 0.03 in September 2023.
All of these results were statistically significant using the same statistical process control test as for the principal indicator.
Variation by district was visible in the data, but improvement was seen in two-thirds of districts (13 of 19), which include both large and small districts.
Conclusion
The reductions in seclusion rates shown in the data above are the results of diligent, creative, collaborative work under strong leadership, including strong Māori leadership, with attention paid equally to matters of culture, data, and consumer input. This work required services to be open-minded to changing an embedded, harmful practice that had been part of the norm for managing challenging or aggressive behaviour in mental health inpatient settings for decades, and trust and belief that there were alternatives. These results are also a result of sustained focus and effort over years, with the support of a national body for measurement and quality improvement, Te Tāhū Hauora.
Two aspects of strong Māori leadership were important: dynamic, cultural leadership within the team itself, but also access to resources and knowledge in the communities the units serve.
Leaders’ attitudes towards measurement were important. ‘What’s measured is what matters’ and where data (particularly data of inequity) were seen by leaders as a valuable tool for improvement, teams followed suit. Staff pay attention to what leaders pay attention to.
Fundamentally, improvement followed leaders’ belief that reducing seclusion was, in fact, possible. From there arose engagement with the data, creativity from leadership, and a culture of creativity enabled in teams to work on ideas that developed into those in the change package.
True co-design and partnership with those with lived experience was also critical to success. 31 This means the ‘frontloading’ of co-design: those most affected by the issue must be brought into the process as early as possible, including problem definition and project design.
Tracking potential substitutionary increases in use of restraint were intended to be a balancing measure in the design of the programme. However, in Aotearoa New Zealand’s PRIMHD mental health database use of restraint data are not collected. This is a limitation.
It is notable that the improvement shown above continued through substantial and challenging disruption. The Aotearoa New Zealand COVID-19 pandemic response was characterised by stringent early lockdowns and border closures for 2 years, including much pressure on mental health services. Once the so-called ‘keep it out’ strategy was overrun in early 2022, these disruptions morphed into staff illness, isolation requirements and burnout. 39 Simultaneously, the health system underwent significant restructuring. 40 Despite these conditions, reduction in seclusion, and reduction in the inequities associated with it, was possible.
Supplemental Material
Supplemental Material - Closing the equity gap as we approach zero seclusion: Successes of the quality improvement project some doubted could be done
Supplemental Material for Closing the equity gap as we approach zero seclusion: Successes of the quality improvement project some doubted could be done by Clive Bensemann, Jess Drummond, Karen O'Keeffe, Arana Pearson, Jacqueline Ryan, Carl Shuker, Karl Wairama, and Wi Keelan in Australasian Psychiatry
Footnotes
Acknowledgements
The authors wish to acknowledge Te Hiringa Kounga Māori, the group who provided Māori advice and cultural expertise to the programme.
Disclosure
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: the authors are paid employees of Te Tāhū Hauora Health Quality & Safety Commission (Te Tāhū Hauora) Mental Health and Addiction Quality Improvement programme, and worked on the project from which this research was derived. Te Tāhū Hauora is funded by the New Zealand Government.
Ethical statement
Supplemental Material
Supplemental material for this article is available online
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.