
Abstract
Background
Despite a limited evidence base to inform clinicians, Australia has adopted a national approach in rescheduling psilocybin and MDMA as clinical therapies for treatment-resistant depression (TRD) and post-traumatic stress disorder (PTSD), respectively.
Purpose
This paper explores clinical research domains warranting further investigation through outlining the reflections of a clinical-academic psychiatrist involved in psychedelic trial work.
Results
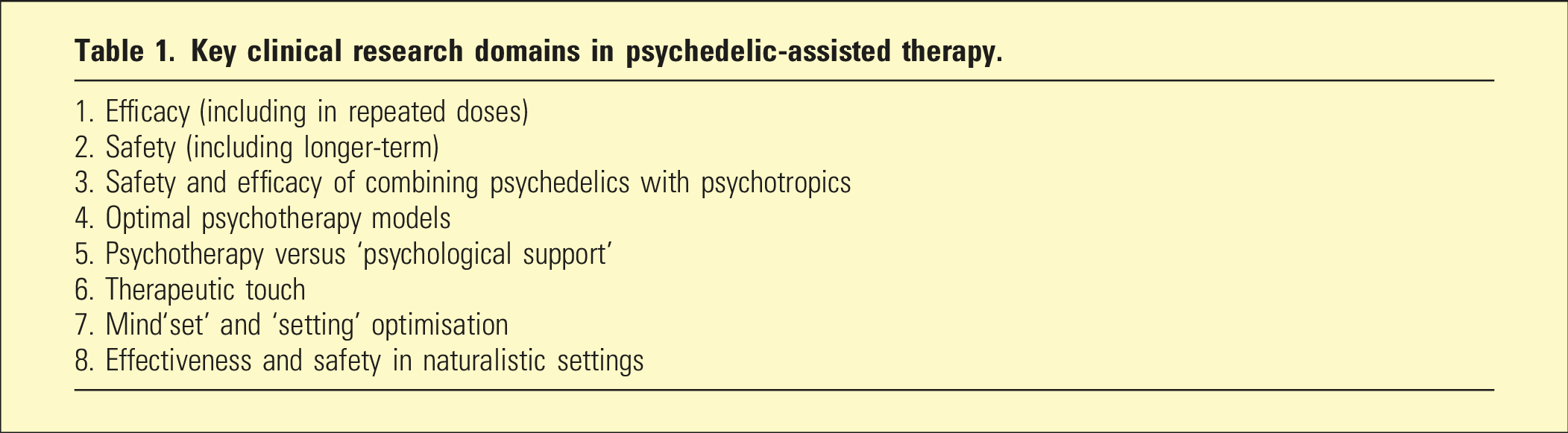
Eight domains were found to warrant further research investigation including: efficacy, safety (including combining with psychotropics), psychotherapy models, psychological support, therapeutic touch, set/setting and examination of naturalistic data.
Conclusions
The clinical availability of psychedelic-assisted therapy (PAT) gives greater impetus for careful research studies, informing treatment and improving patient outcomes.
Introduction
Over the past several years, I have worked as a clinical researcher on several psychedelic trials, including as half of a therapist dyad in a psilocybin-assisted therapy trial – a collaboration between Black Dog Institute and St Vincent’s Hospital, Sydney. I recall the surreal feeling when first writing ‘PSILOYCBIN’ on a medication chart, thinking it was not a medicine I ever expected to prescribe. Flashback to a decade ago, as a junior consultant I delivered a grand rounds presentation on: ‘Making a Medicine out of MDMA’ 1 and ‘Can psychedelic compounds play a part in drug dependence therapy?’ 2 Published in the British Journal of Psychiatry, the cover featured psychedelia-inspired images with chemist ‘Sasha’ Shulgin holding an MDMA molecule, which he ‘re-discovered’ and introduced to the psychotherapeutic community in the 1970s. The talk was met with more than a few raised eyebrows from colleagues. Fast-forward to 2023, the Therapeutic Good Administration (TGA) down-scheduled from Schedule 9 (prohibited) to Schedule 8 (controlled) substances – MDMA for posttraumatic stress disorder (PTSD) and psilocybin (the psychoactive ingredient found in ‘magic mushrooms’) for treatment-resistant depression (TRD), 3 Australia being the first country to adopt a national approach to medical regulation.
Preceding this decision, there was renewed popular interest in psychedelics globally (e.g. Michael Pollan’s 2008 bestseller ‘How to Change Your Mind’). 4 Locally, there was intense lobbying of the TGA from advocacy groups and a powerful message sent from people with lived experience, with over 13,000 public submissions describing personal mental health struggles despite existing treatments, demonstrating the ‘scope and gravity’ of the public health issue. 3
The TGA’s decision was surprising and groundbreaking, as psychedelics were largely banned substances worldwide for 50 years, considered harmful by society-at-large. As a psychiatry trainee, I developed an unquestioned assumption that psychedelics must necessarily be ‘bad’ for patients. Not surprising, given my training was weighted towards psychosis services, where young patients presented with drug-induced psychoses. It was an intellectual leap to consider these substances might – when used for non-psychotic conditions in controlled settings – be of benefit to select patients.
The TGA relied on evidence from phase III trials of MDMA-assisted therapy for PTSD,5,6 with a lower standard of evidence for psilocybin-assisted therapy in TRD (no published phase III trials to date). 3 Further, to become an authorised prescriber of an ‘unapproved’ medicine, the TGA requires a lower level of evidence if clinical need is high 7 – which raises ethical considerations relating to beneficence and non-malfeasance. In treating severe TRD or PTSD – clinical need is high – however, there is a risk that gaps in the evidence base or poorer quality evidence could result in unknown or unintended harms (e.g. is there a longer-term risk of substance misuse?). In an ecosystem where these drugs can now be prescribed clinically, it remains important that regulatory approval doesn’t forestall continued accumulation of an adequate evidence-base. 8 The following are my reflections on the need for further clinical research in this emerging field.
Research questions
Key clinical research domains in psychedelic-assisted therapy.
Many with TRD or PTSD cannot easily withdraw from existing treatments (prerequisite for most studies) without becoming destabilised and suicidal. There is limited data examining addition of psilocybin or MDMA to psychotropics, for example, selective serotonin reuptake inhibitors.10,11 Can they can be safely added to antidepressants or other psychotropics, and what is the impact on efficacy?
It’s argued that psychedelics have a positive safety versus risk profile including low risk of dependence. However, in the Goodwin et al. study, 9 77% of patients had side effects, with 9%–17% experiencing a worsening of suicidal ideation/behaviour or deliberate self-harm. The Food and Drug Administration rejected approval of MDMA-assisted therapy for PTSD partly due to underreporting of adverse events. Further safety data (including longer-term), with more stringent collection, and development of structured monitoring tools (akin to the Ketamine Side Effect Tool-Revised 12 ) are needed to inform clinicians and patients.
Psychedelic-assisted therapy (PAT) challenges standard psychotherapeutic practice, being akin to an ‘intervention’. Preparation and integration sessions bookend a dosing day, with potential for rapid psychological changes. Patients may have the equivalent of a year’s worth of therapy hours in a single month. But what type of therapy should be used? Should the psychedelic be administered using the PAT model or would combining it with a manualised therapy be superior? Could similar results be achieved with a ‘light touch’ approach, where therapists act like midwives – ensuring dosing day safety – while allowing the patient’s process to unfold and the drug to have its therapeutic effect? 13 Trials comparing differing forms of psychotherapies versus ‘psychological support’ would be enlightening.
PAT utilises two therapists in a dyad. An historical precedent to have both feminine/masculine presence in the room, it also reduces risks of boundary violations. Is the dyad model feasible in clinical practice given its burden on clinical resources? Could PAT be adapted to scalable group settings? A model with group integration, could be tested to examine if patients can be safely managed with comparable benefits.
Therapeutic touch (TT), a core element of PAT, challenges a tenet we learn as psychiatrists, which is ‘never touch the patient’. TT is used if patients are distressed or require grounding under acute effects of psychedelics. Formal consent forms are often used in trials. The risk of boundary violations increases once TT is an option, with an alleged serious sexual boundary violation occurring in a trial. Exploration of TT ethical and safety issues are needed to minimise breaches which could negatively impact patients and the field as a whole.
Aldous Huxley famously wrote, the brain operates as a ‘reducing valve’ whereas psychedelics act as ‘amplifiers’. 14 PAT emphasises mindset (‘set’) and ‘setting’ as important factors which affect the psychedelic experience. Many public psychiatric facilities are gloomy places – replete with plastic chairs, harsh lighting, and noise. In psychedelic trials, attention is given to creating a comfortable environment, for example, soft furnishings, artwork, indirect lighting, use of scent and music. How psychedelic services can be delivered with due consideration to these factors needs examination – with cost a significant barrier. Qualitative research on which aspects of set and setting are important to optimise would be another area of fruitful research.
Real-world patients are often more complex than trial participants – with comorbidities and higher risk. Trial results may not easily be generalised to clinic patients with potential for worse outcomes. The TGA decision means the field has little choice but to adopt a pragmatic approach and observe if requirements such as ethics committee approval of authorised prescriber protocols offer sufficient guardrails. Naturalistic data should be collected from clinics to understand the effectiveness and risk profiles outside of trials. This could be facilitated by centralised research registries, assisting with minimum data collection and benchmarking, for example, the Clinical Alliance and Research Excellence (CARE) in Electroconvulsive Therapy and Interventional Psychiatry Network. 15
Conclusion
Laypeople and colleagues often ask me: ‘now that MDMA and psilocybin can be prescribed, why the need for more research?’ The answer is there’s an even greater imperative for undertaking studies, to guide clinicians in safely treating real-world patients with PTSD and TRD. There are also more conditions that might be treated with psychedelics (e.g. anxiety, substance use and eating disorders), with studies underway. And there are other psychedelic substances to explore – both existing and in development. In the clinical realm, collection of naturalistic data will supplement results from formal trials. The TGA has undertaken a national experiment, and the world is watching. The method to conduct any experiment – is through research – with formal and naturalistic approaches providing a rich opportunity for Australia to lead the world in psychedelic science and clinical practice.
Footnotes
Acknowledgements
I thank Prof. Collen Loo for reviewing the manuscript.
Disclosure
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.