
Abstract
Objective
The most common psychiatric disorders in adolescents are anxiety and mood disorders. Often, anxiety itself is a prelude to depression and irritability is an antecedent to both. Thus, irritability likely heralds the onset of mental illness in adolescents, especially those disorders with a bias in gender prevalence. Consequently, it is necessary to examine irritability to obtain a comprehensive understanding of this phenomenon. Further, factoring gender into these examinations may provide insights into its nature and the role it putatively plays in the development of anxiety, depression and suicide in adolescence. Presently, efforts for early intervention look to identifying established disorders early in their course; however, by detecting symptoms that are precursors it may be possible to shift the focus of health practice and policy.
Conclusions
Viewing irritability through a lens of gender during adolescence may yield key insights that inform our understanding of how disorders and outcomes that have a bias in gender prevalence emerge. By considering the divergent experiences of puberty, and factoring these into our mechanistic understanding of irritability, pathways for future systematic examinations become clearer.
To inform health policy we need to understand the antecedents of anxiety and depression which begins by studying the phenomenology of irritability.
Irritability: A phenomenological enigma
Irritability is a clinical and phenomenological enigma – manifesting across a range of psychiatric disorders and across all ages. 1 It is common in health, and like other normal phenomena such as anxiety, it is difficult to determine when irritability becomes clinically significant as a ‘symptom’ – a problem as it were – as opposed to a normative experience. 2 Irritability’s ubiquity across both health and illness has meant it lacks a conceptual home in psychiatry, and classificatory systems count it as a symptom of several different psychiatric disorders1,2 highlighting its lack of specificity. For example, in mood disorders, irritability is a symptom of both mania and depression 3 contingent on age – seemingly contradicting the conceptualisation of these poles of mood as being diametric opposites.
Irritability’s transdiagnostic existence has meant it has been examined from a variety of perspectives: its role in externalising disorders has prompted attention from those in the paediatric domain and its entanglement in emotion has piqued the interest of those in mood disorders’ research. Hence, different definitions of irritability have been informed by research in different populations and various conceptual frameworks have emerged. For example, studies in children link irritability to behavioural outcomes, such as temper outbursts and aggression, and purported underlying mechanisms, such as emotion and reward system dysregulation.1,4 Similarly, studies in mania attempt to group irritability with similar concepts such as agitation, without providing operational definitions that distinguish these constructs. 5 An overarching problem that has thwarted most analyses of irritability has been the focus on the behavioural consequences and external triggers or stimuli, instead of examining the internal experience of being irritable.6,7 Suffice to say, a conceptually accurate definition of irritability that also achieves consensus in psychiatry is yet to be determined.
A pragmatic compromise that is gaining validity, because of its simultaneous breadth and distinction from closely-related constructs such as anger and aggression,7,8 characterises the experience of irritability as one of partial physiological agitation - in other words, one of increased arousal and tension that is at lower level of intensity as anger, for example. This experience also entails an increased sensitivity to stimuli, combined with a non-cognitively mediated lowered threshold for responding with anger or aggression to stimuli that is typically less-vexing. 7 In addition, irritability may be caused by direct physiological factors such as hunger, sleep deprivation, pain or fatigue and as such manifests in response to frustration from unmet needs. 8 Notably, by this definition, irritability is not always accompanied by aggressive behaviours, and it is not necessarily pathological.
In addition, irritability is conceptually distinct from related phenomena such as anger and emotion dysregulation. With regard to anger, irritability can largely be distinguished due to its generally lesser intensity, and the fact that it often emerges without a cause that is obvious to the person who experiences it (for further detail, see 9 ). Moreover, in paediatric contexts, irritability is often characterised as a form of emotion dysregulation. 10 However, whilst irritability may manifest due to an underlying problem with managing one’s emotions, this characterisation implies that irritability manifests as behavioural outbursts of anger that are observable to others. But these behavioural manifestations are not reflective of the subjective experience of irritability that occurs in adolescence and adulthood which does not necessarily demonstrate in observable behaviours. 11 Thus, framing irritability as emotion dysregulation is not applicable to various clinical circumstances in adolescence and adulthood where irritability occurs. Therefore, there are gaps in our current understanding of the relationship between emotion regulation and irritability – particularly beyond childhood.
Where to look for irritability?
The recency of the aforementioned definition means that most research on irritability is yet to make use of this framework – in other words, the conceptualisation of irritability as a ‘subjective experience’ – and persists in examining external indicators such as temper outbursts and focuses on populations where it is most often presented. Indeed, the majority of research on the concept has focused on children, among whom irritability is a common ‘clinical complaint’, 12 with only few epidemiological studies examining the construct in adolescents 13 and adults. 14 This is problematic for two reasons.
First, children do not have the capacity to introspect in the same way as adolescents and adults; hence, their ability to report their symptoms is understandably limited. Therefore, measures of their irritability often rely on more tangible indicators, such as temper outbursts and behavioural disturbances, that are reported by an observer and from which inferences are made.4,7 As noted in the definition above, these behaviours are not necessarily present when irritable, and in children it may be difficult to link these behaviours to the subjective experience of irritability specifically, as opposed to impulsivity or agitation, for which there could be a number of potential explanations such as an attentional difficulty or cognitive impairment. Thus, trying to examine irritability in children and link it with an underlying disorder is difficult.
Second, psychiatric disorders are generally more difficult to define in children, and confidence in diagnosis is lower than that in adolescents or adults, especially as even disorders that are thought to have distinct aetiologies usually have overlapping manifestations in children. For example, behavioural outbursts may indicate different disorders such as depression, externalising disorders and neurodevelopmental disorders. Therefore, in practice, it is only as a child ages and symptoms become more delineated, that a diagnosis can be made with more confidence and to the exclusion of other causes.
Thus, by focusing on children, most research aiming to understand irritability has been studying the population in which disentangling underlying causes of symptoms is arguably the most challenging. In addition, and related to this, studies of irritability employ a wide variety of measures to capture it as a construct; however, they either do not consider all the subcomponents of irritability (proneness to anger or aggression and increased likelihood of externalisation of negative emotions) or lack validity.7,8 This is because they either, for example, rely on behavioural indices of irritability (rated by an external observer such as a parent), measure constructs that overlap with related concepts (e.g. anger), include specific external triggers (e.g. interpersonal conflict) or consequences (e.g. verbal arguments), or simply rely on a single item. 5 Thus, a combination of problems both with the populations that have been studied and the means used to capture the construct have meant that irritability research has been hamstrung.
Progress is being made to address the limitations of measuring irritability, and conceptual examinations of existing measures have determined that subjective measures that do not overlap with related but distinct concepts such as anger, aggression or behavioural consequences should be used where possible, such as, for example, the Brief Irritability Test (BITe).7,8 By utilising BITe in adolescents who have already developed the ability to introspect and report subjective experiences, it is hoped that the findings gained will inform more valid and reliable measurements of irritability that can be used in children. It is important to address these issues not only for theoretical clarity but because irritability’s presence within mood and anxiety disorders, self-harm and suicide suggests that a better understanding of its ontology is likely to yield deeper insights into these outcomes, which in turn would improve their detection, prevention and management. Thus, modelling the underlying mechanisms and outcomes of irritability will inform future healthcare research and policy.
Viewing adolescent changes through a gendered lens
Gender plays a key role when considering a macro view of the outcomes linked to irritability, namely, depression and anxiety disorders, self-harm and suicide. In mood disorders, for example, gender plays a significant role with regard to prevalence and separates depression, which is twice as prevalent in women than men, 15 from bipolar disorder, in which both genders are affected equally. Further, women are more likely to experience anxiety disorders 16 and self-harm behaviours, 17 whereas men are more likely to die by suicide. 18 Critically, these differences emerge during adolescence between the ages of 12 and 18 years, when girls and boys diverge both developmentally and in terms of their psychosocial experiences, and many psychiatric disorders, or their incipient symptoms, first appear. Adolescence is also a time when the brain undergoes maturation, and individuals gain the ability to introspect and provide a subjective account of their experiences. Thus, if we want to examine the emergence of anxiety and mood disorders, or other outcomes, such as suicide and self-harm, and the role that irritability may play, then examining irritability across adolescence using the lens of gender seems the most apt.
It is important to note that while the term ‘sex’ is typically used to refer exclusively to biological characteristics (i.e. female and male) and ‘gender’ is used to refer to psychosocial characteristics related to a person’s self-identity (i.e. women and men), for the purposes of this paper, we refer to these qualities collectively as ‘gender’ as we consider both the biological and psychosocial factors to be interrelated and as yet, indistinguishable.
Findings regarding age, gender and irritability
Research focusing on the relationship between gender and irritability during adolescence in particular is sparse, despite the interest in examining irritability and its behavioural outcomes. Indeed, recent large-scale longitudinal studies that have aimed to examine irritability over adolescence did not use gender as a framework to examine their findings.19,20 Whilst these studies report the distribution of girls and boys in their respective findings, critically, they neither utilised gender as a lens through which to view the role that irritability plays throughout adolescence, and in the development of mood symptoms and other negative outcomes.
In our own research, 21 for example, we found that there is an important interplay that occurs between irritability, age and gender. For instance, in adolescent girls, irritability is associated with both manic and depressive symptoms, and the pathways and factors that mediate the relationships between irritability, anxiety, emotion regulation and mood symptoms differ according to age. Furthermore, irritability is associated with depressive symptoms and mediated through trait anxiety in both early and late adolescents, but it is not significantly associated with depressive symptoms in middle adolescents.
In contrast, in our separate study in boys, 22 irritability had no significant interaction with age across adolescence, but it was associated with difficulties in emotion regulation. Irritability appears to bridge the gap between these difficulties and behavioural outcomes, such as emotional reactivity, social difficulties, hyperactivity and conduct problems. We therefore hypothesised that correlations between irritability, emotion regulation and behavioural difficulties point to a mechanistic link between difficulties in accepting negative emotions leading to irritability, which in turn causes behavioural disturbances, anxiety and eventually depressive symptoms. Importantly, these findings would not have been uncovered had irritability not been examined through the lens of gender.
Our insights have been extended by others. In recent cross-sectional irritability research, it was found that, in contrast to our own findings, irritability did seem to interact with age in boys but not in girls.
23
In girls, internalising reactions to negative emotions were found to be positively associated with age. In boys, on the other hand, irritability, and its subcomponents of proneness to anger, externalisation of negative emotion reactions and reactive aggression were all negatively associated with age (see Figure 1). However, there are two key methodological differences between this study
23
and our research.21,22 First, in this study the cohort spanned ages 4–19 years, thereby encompassing early childhood, and second the analysis combined both parent- and self-report measures, while our studies mentioned above implemented only the latter. This is problematic, as the concordance between parent and child ratings of outcomes such as internalising symptoms tends to be weak.
24
In addition, parents are more likely to rate boys as having higher irritability than girls during childhood and rate boys and girls as having similar levels of irritability during adolescence, despite adolescent girls reporting significantly higher irritability than boys
25
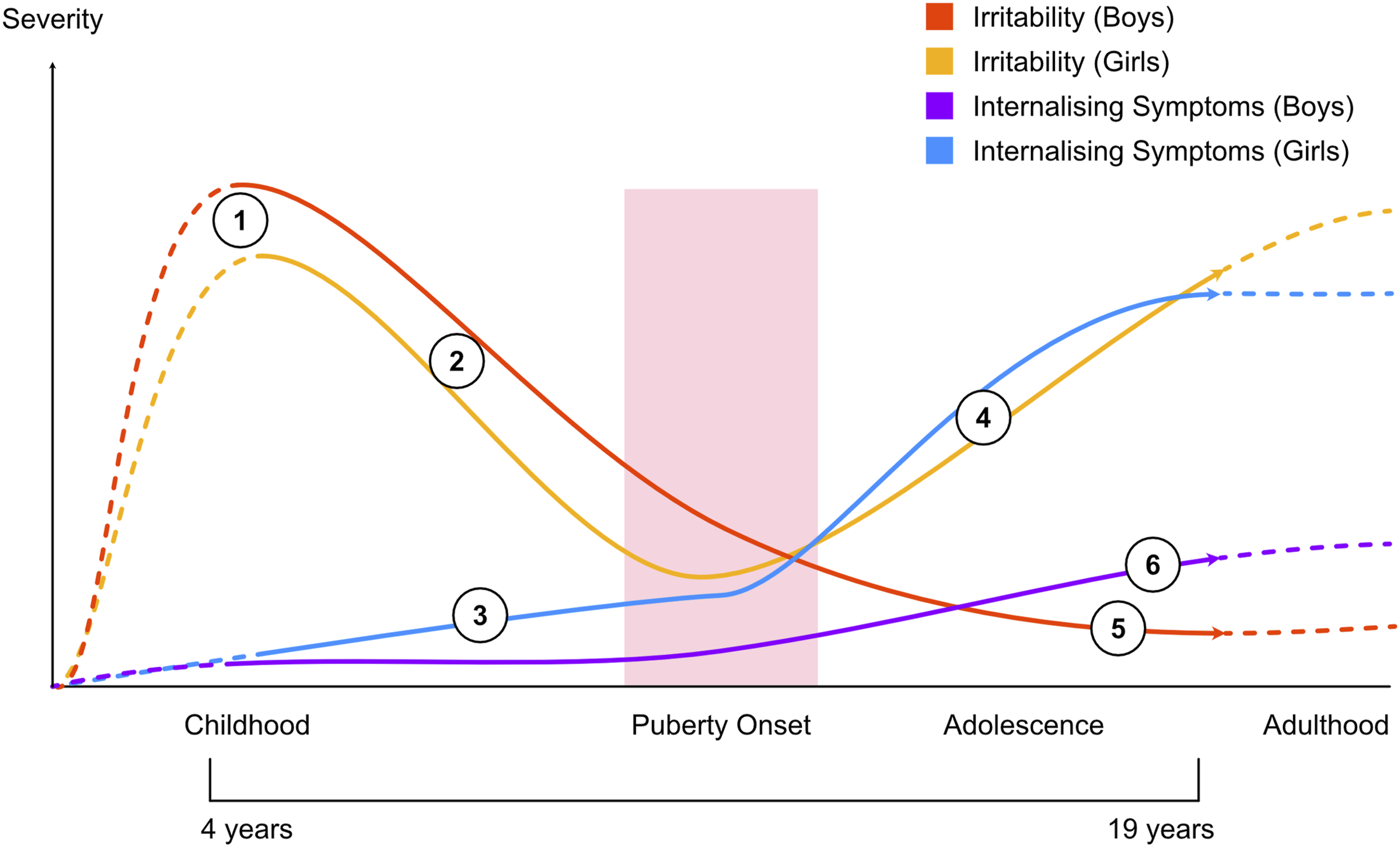
in self-report measures. Thus, the effects of age over the broad sampling period of 4–19 years may be difficult to ascertain, especially if this relationship is not linear. Schematic of interactions between age, severity of irritability and internalising symptoms in boys and girls. This schematic attempts to capture the summative trends over time in levels of irritability and internalising symptoms, and how these differ between boys and girls, extrapolated from key studies. Dotted lines indicate approximations in ages for which data is limited, and solid lines indicate trends from the ages of 4–19 years.
20
In both genders, irritability is high in early childhood
23
(1), and decreases steadily with age (2) as the brain develops throughout childhood. In girls, internalising symptoms increase over time (3) and this is coupled with an increase in irritability (4) following the onset of puberty (pink shading),
24
as girls manage monthly menstruation cycles which is associated with frustration. The non-linear relation of irritability with maturation (time) explains in part why studies that try to find an age-by-irritability interaction in a population that spans both childhood and adolescence, have found it difficult to establish a clear relationship in girls. With a significant event like menarche occurring in the middle of this sampling window, and with menstruation causing ongoing monthly difficulties, it is likely that levels of irritability in girls change as a function of this recurrent, disruptive event. The coupling of an increase in irritability post-puberty with an increase in internalising symptoms
20
(4) poses an additional risk of developing anxiety and depressive disorders in girls. In contrast, in boys, irritability continues to decrease steadily from childhood to adulthood
20
(5) and though, similar to this, internalising symptoms may increase following puberty (6), the increment is much smaller than that seen in girls.
20
Studies that employ a broad sampling methodology that straddles both childhood and adolescence, may not be able to detect overall interactions between age and irritability, if they are not linear. However, they can indicate linear trends in some variables such as internalising and externalising symptoms that persist over this time period. The finding that internalising symptoms show a positive relationship with age in girls indicates that this trend persists from childhood through to adolescence despite other, potential non-linear trajectories of factors such as irritability and its subcomponents. At the same time, boys experience a decrease in behavioural outcomes such as externalising behaviours and aggression as they mature from childhood to adulthood, especially after puberty.
A key event that occurs during the time period from childhood to late adolescence is the onset of puberty which causes a significant biological and psychosocial divergence in the experiences of girls and boys. Specifically, once menarche commences, girls experience emotional vicissitudes that can lead to ongoing psychological difficulties as they grapple with their now monthly hormonal cycle. Whilst boys too experience difficulties in coming to terms with their physical, emotional and cognitive changes that are not to be understated, the key difference is that these changes occur gradually over time and do not entail the same regular fluctuations in hormones and consequent emotional and physical upheaval that girls experience. Indeed, early menarche in girls is strongly linked with elevated and earlier onset of depressive symptoms. 26 Further, this effect is specific to depressive symptoms and not mental health outcomes more generally, and therefore a causal link between these two events has been posited. 26
Thus, approximately halfway between childhood and adulthood there is a key event that begins to distinguish girls and boys not only physically, but psychologically, which can have significant consequences when trying to assess the temporality of psychiatric phenomena during this time period. Importantly, this period may lead to non-linear trends in symptoms such as irritability in girls, wherein after puberty, girls experience an increase in internalising symptoms, as well as monthly fluctuations in their emotions according to their cycle, which can further increase irritability. This increased irritability in girls could provide a link between changes in their internalising emotional states, and poorer outcomes.
Previous research has established a clear link between increased irritability and a greater risk of poorer emotion regulation in both girls and boys.
27
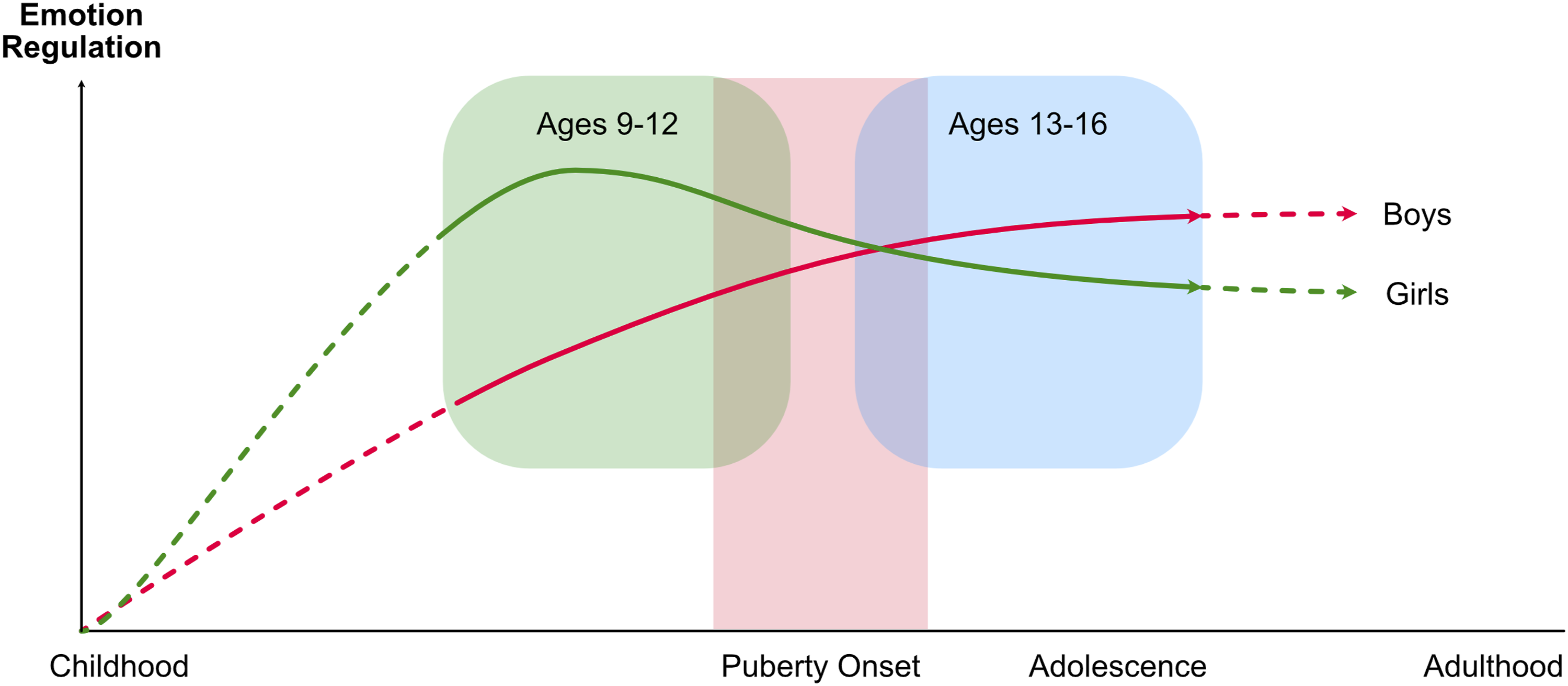
However, recent findings have shown that there is an interaction between gender and age, wherein younger girls show better emotion regulation strategies than younger boys; however, this relationship is reversed in older adolescents, wherein older boys show greater scores than older girls
28
(see Figure 2). Arguably, this may be because of the ongoing difficulties faced by girls following puberty, and whilst the developmental transition from childhood through to sexual and psychological maturity is universally difficult, girls experience monthly pain, hormonal fluctuations and stress, which potentially adds to their frustration and psychological burden, and decreases their ability for emotional regulation. Schematic illustrating changes in emotion regulation between girls and boys from early childhood to adulthood. This schematic extrapolates from research examining changes in emotion regulation between boys and girls at ages 9–12 years and at ages 13–16 years.
24
Younger girls show greater emotion regulation skills than boys (green shading), however this relationship is flipped in older adolescents (blue shading). As seen in Figure 1, girls show a positive association between internalising reactions to negative emotions and age. Thus, with this additional burden of significantly increased internalising symptoms and irritability, girls may experience diminished capacity for emotion regulation,
25
and potentially an increase in maladaptive strategies such as withdrawal and self-devaluation.
24
The divergence between girls and boys with regard to irritability and its relationship with age, alongside other factors such as emotion regulation skills and internalising symptoms is important, because while both adolescent girls and boys are prone to depression and suicide, girls are at greater risk of developing internalising disorders such as depression and boys are at greater risk of externalising problems such as aggression and dying via suicide. This gender-specific separation is evident in childhood, where irritability has been more strongly linked with later self-harm in boys than in girls.29,30 Thus, if a mechanistic understanding of how these factors interact to produce these outcomes is to be envisaged, then a pathway for future research into each of these factors is needed – one that could yield critical insights into the development of mental health problems in adolescence.
A mechanistic model for gender, age and irritability
In order to make sense of the relationships between the various components discussed, namely, irritability, age, gender, internalising symptoms, emotion regulation, negative behavioural outcomes and anxiety and mood symptoms, we propose a mechanistic model that is informed by our own research as well as the recent developments made by others (Figure 3). This model builds on the model originally developed in adolescent boys
22
and expands this to accommodate differences between boys and girls and the effect of the interplay between gender and age. Schematic positing a mechanistic model for the relationships between gender, irritability and known risk factors for the later development of psychiatric problems in adolescents.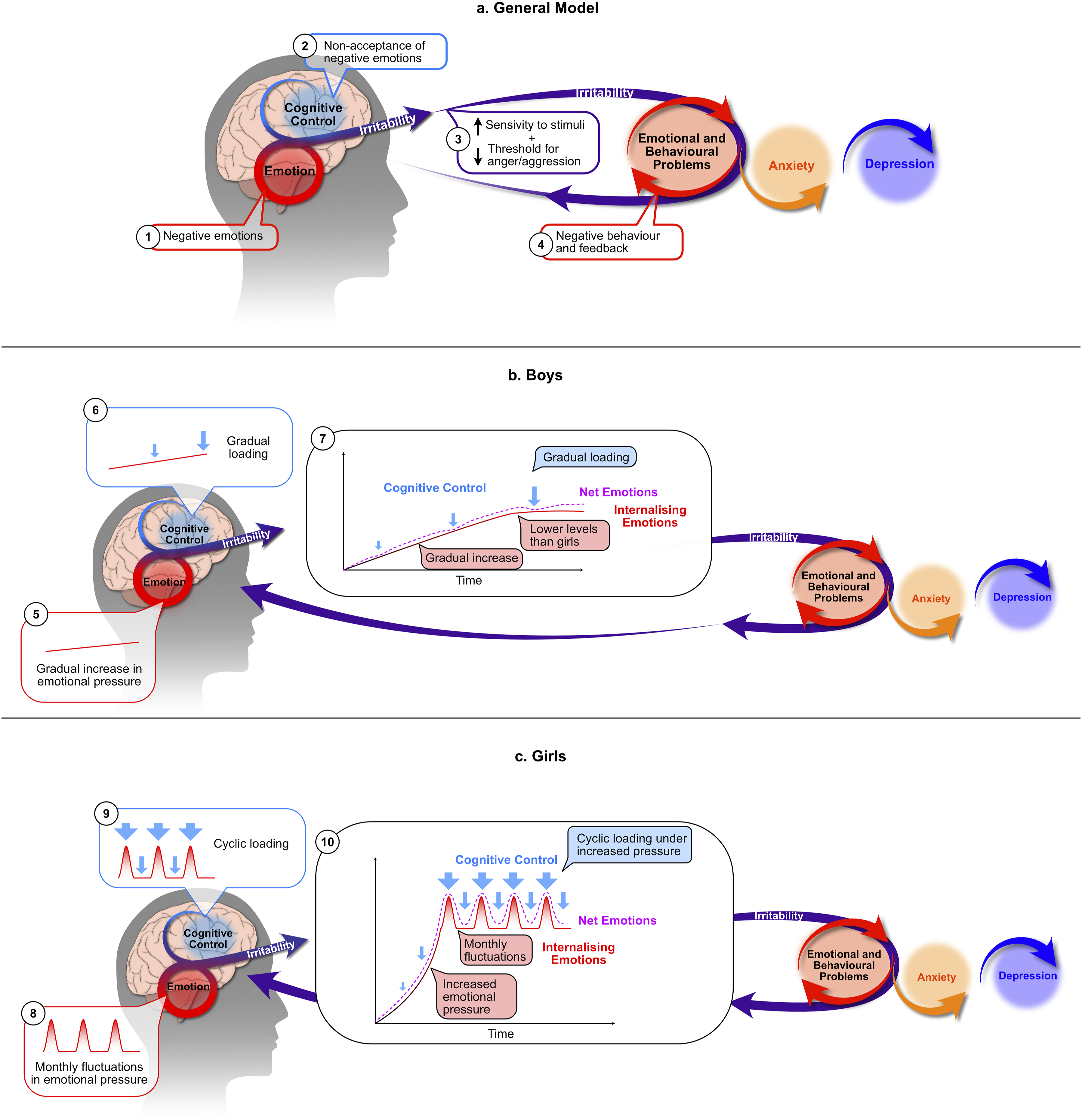
For both girls and boys (Figure 3(a)), the key elements of the model remain the same – that is, both begin with the interplay between emotions and their cognitive control. Irritability emerges from non-acceptance of negative emotions, leading to emotional and behavioural problems.21,22 These problems lead to external feedback from those around the adolescent that perpetuates and exacerbates the cycle of negative emotions, poor cognitive control and increased irritability. Eventually, this culminates in increasing anxiety and depressive symptoms. The main differences between boys and girls lie in the early components of the model, namely, the interplay between emotions and cognitive control.
In boys, internalising emotions increase gradually or remain relatively stable over adolescence, and, because this change is gradual, cognitive adaptation is easier, and the degree of control required is relatively consistent and at a level that can be sustained and acclimatised to over adolescence. In girls, monthly fluctuations in emotions occur following menarche and this places cyclic loading on their cognitive control resources. In addition, girls experience an overall increased level of internalising emotions from childhood through to adolescence 23 (see Figure 1). The summative effect of these components means that girls experience increasing negative emotions, conceptualised schematically (in Figure 3(c)) as emotional ‘pressure’, and this is coupled with additional cyclic loading throughout their menstrual cycle. The overall greater pressure as well as its fluctuating nature make it far more difficult to control and regulate. However, it is important to note that this model does not suggest that girls have a diminished capacity for emotion regulation but rather that despite the fact that girls develop cognitive control and regulation of their emotions earlier than boys (see Figure 2), the emotional pressure they experience is both unsustainable and difficult to habituate to.
Future directions
The proposed model is helpful as it incorporates irritability, which is often overlooked as an antecedent to anxiety and depression and gender, which allows for a more sophisticated formulation of the model. The model clearly needs to be tested but it is envisaged that it will allow key questions to be explored. For instance, currently, the impact of gender on the longitudinal trajectories of irritability remains unclear. Specifically, the relationship between irritability and internalising symptoms in adolescent girls and outcomes such as suicide in boys.4,29 This is critical because whilst adolescent boys more likely die via suicide than adolescent girls, 18 adolescent girls are more likely to develop depression than boys. 15 Therefore, the potential role of irritability in this gender divergence of symptoms and outcomes may provide insights that allow us to more effectively identify who is at risk of suicide or developing mood disorders.
An obvious limitation of the current model is that it currently only encompasses a binary model for gender, and does not yet account for those with other gender identities or those that are transgender. This is important as these individuals are not only at greater risk of psychiatric disorders, but would likely also include a more complex interplay between biological and psychosocial factors that impact wellbeing.
Therefore, this model should be further tested with a view to incorporating the gender diverse population to not only gain insights as regards the wellbeing of this under-researched population, but also these findings may further inform our understanding of the relationship between biological and psychosocial factors that are relevant to all adolescents. Thus, future examinations that are structured according to the proposed model are likely to provide a more sophisticated pathway for influencing healthcare research and policy by enabling the earlier detection and management of irritability and facilitating the prevention of its consequences in adolescence and early adulthood.
Footnotes
Acknowledgements
The authors would like to acknowledge the Greek Young Matrons' Association (GYMA) for their ongoing support.
Author contributions
E.B. conducted the literature review, generated the original draft and developed the figures. All authors contributed to the editing of this manuscript. All authors have read and approve of the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: E.B. has received joint grant funding from the University of Sydney and National Taiwan University (Ignition Grant), The North Foundation and the Greek Young Matrons’ Association (GYMA). P.B. has received speaker fees from Servier and Janssen, educational support from Servier and Lundbeck, is on an advisory board for Incite Health, has been a consultant for Servier, inhaleRx and Greenhorn industries and has served as DSMC Chair for Douglas Pharmaceuticals. K.S. has received grant funding from the Greek Young Matrons’ Association (GYMA). G.S.M. was Editor-in-Chief of ANZJP 2010–2021 and is presently College Editor and Editor-in-Chief of the British Journal of Psychiatry and advisor to the Editor of Australasian Psychiatry. He has received grant or research support from National Health and Medical Research Council, Australian Rotary Health, NSW Health, American Foundation for Suicide Prevention, Ramsay Research and Teaching Fund, Elsevier, AstraZeneca, Janssen-Cilag, Lundbeck, Otsuka and Servier and has been a consultant for AstraZeneca, Janssen-Cilag, Lundbeck, Otsuka and Servier. He is the recipient of an investigator-initiated grant from Janssen-Cilag (PoET Study), joint grant funding from the University of Sydney and National Taiwan University (Ignition Grant) and grant funding from The North Foundation.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.