
Abstract
Objective
The Australian Primary Health Networks’ Initial Assessment and Referral Decision Support Tool (IAR-DST) aims to help clinicians recommend an appropriate Level of Care (LOC) for adults with mental health difficulties. This study evaluated whether the IAR-DST has utility assessing ongoing care needs for young adults attending a tertiary community mental health service.
Method
Cross-sectional IAR-DST ratings for young adults (aged 18–24 years) attending a tertiary community mental health service in Adelaide in May 2019 were based on retrospective file review by senior clinicians. Health service use indices during patients’ current episode of care were collected using electronic record systems. Incidence Rate Ratios (IRRs) were generated to compare service intensity.
Results
104 young adults were included. Psychotic Spectrum Disorders and Borderline Personality Disorder were the most common diagnoses. 63% received IAR-DST ratings recommending for high-intensity care (i.e. LOC 4 or 5), whereas for 37% lower-intensity services were recommended. IRRs showed higher service use with increasing LOC.
Conclusion
The IAR-DST may be useful for reassessing service needs in young adults attending specialist mental health services, to support transitions within a tiered mental health system. More research is needed to evaluate the tool’s utility in different help-seeking populations.
The Lancet Commission on Youth Mental Health (2024) 1 recently reported a decline in mental health of young adults over the past two decades, labelled a “youth mental health crisis” by the US Surgeon General. Mental illness often begins early, with about two-thirds of cases emerging before the age of 25 years. 2 Among people aged 10–24 years, poor mental health contributes to 45% of disease burden. 3 In Australia, suicide is the leading cause of death for those aged 19–44 years. 4
Early, targeted support is crucial to mitigating the immediate and long-term impacts of mental illness, which include educational disruption, social isolation, and functional decline. 1 However, with limited and fragmented mental health resources for young adults,5,6 targeting services to those most in need is a significant challenge.
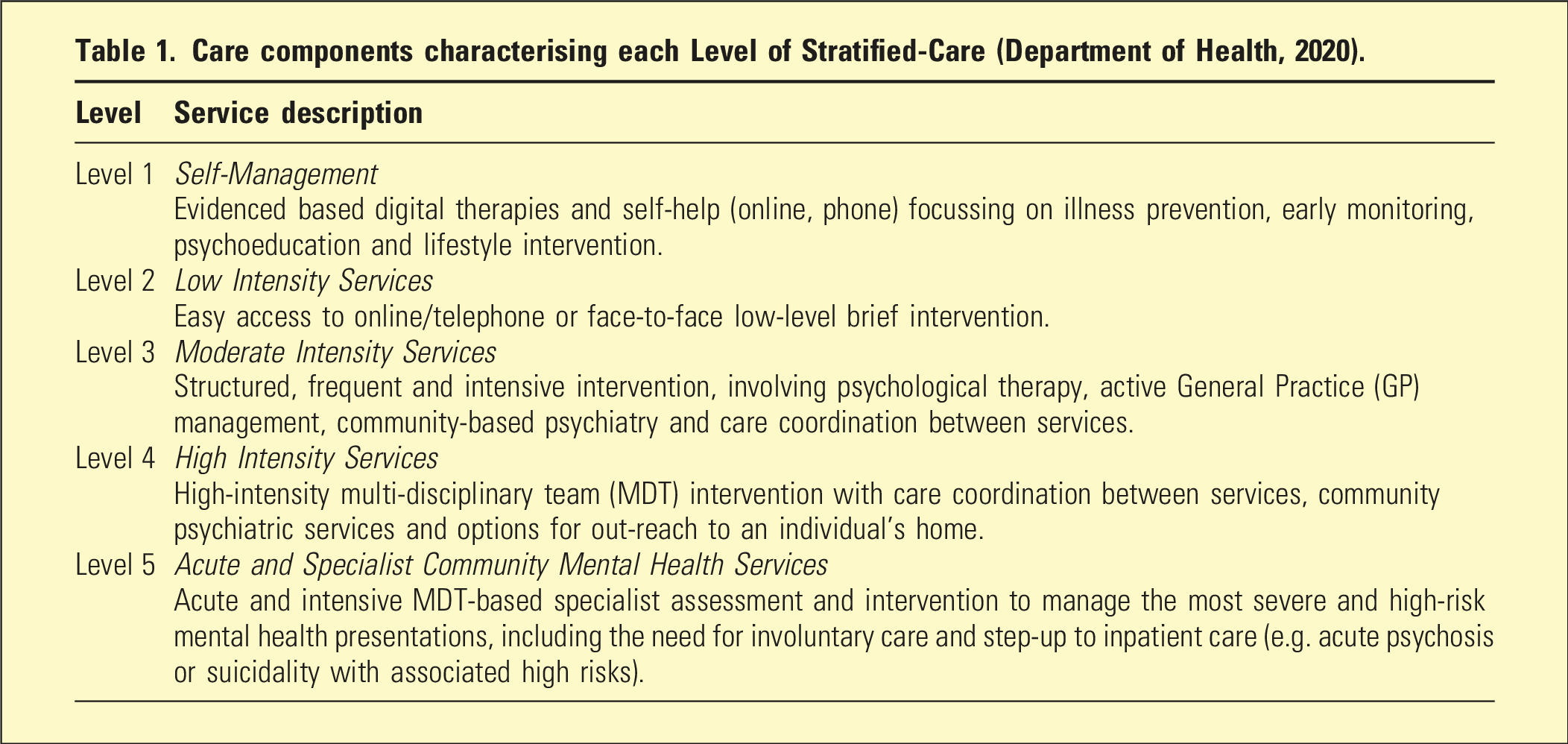
The stratified-care model in mental health
Care components characterising each Level of Stratified-Care (Department of Health, 2020).
The Australian Department of Health developed the Initial Assessment and Referral Decision Support Tool (IAR-DST) for Mental Health Care to help primary health clinicians evaluate mental health treatment needs and recommend appropriate stratified-care referral pathways. 8 In the 2021/2022 Federal Budget, $34.2 million was allocated to expand and implement the tool in primary care settings. 9
The eight initial assessment domains (department of health, 2020).
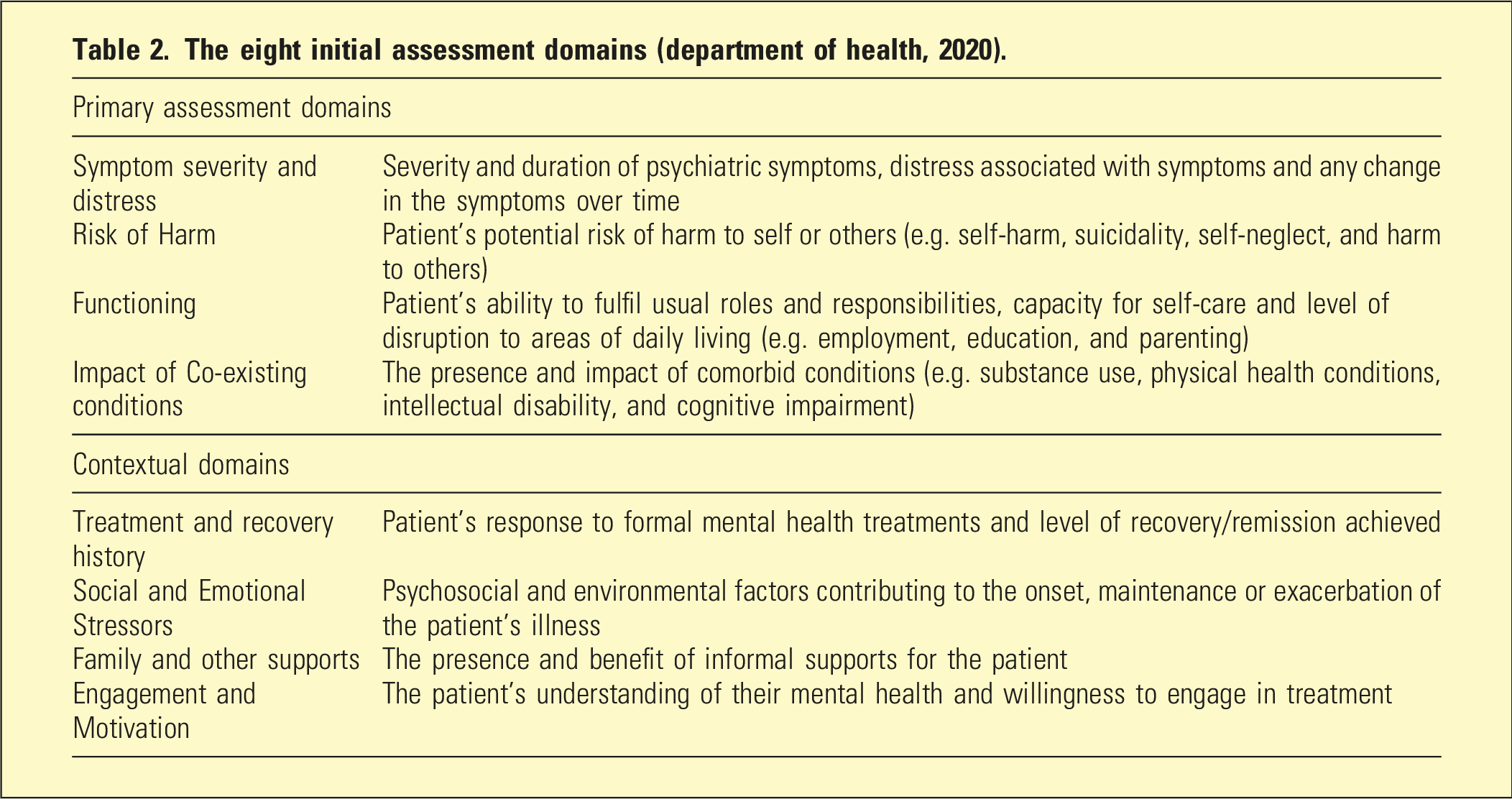
Once rated, each domain is mapped onto the Decision Support Tool (DST), which uses an established logic to recommend the most appropriate Level of Care (LOC) for the individual (Department of Health, 2020). The LOCs range from Level 1 to Level 5, corresponding to increasing service intensity, aligned with the stratified-care model (see Table 1). The IAR-DST is accessible online (https://iar-dst.online).
The IAR-DST was initially designed for an adult primary care population and has not been evaluated in adolescents, young adults, or specialist mental health settings. Whilst the IAR-DST was initially targeted to primary care settings, there has also been substantial consultation and education of tertiary services about this tool, as part of the rollout. This study aimed to assess its utility and applicability in a cohort of young adults receiving treatment at a tertiary mental health service. The primary goal was to determine whether these individuals were receiving the appropriate Level of Care (LOC) as recommended by the IAR-DST. If effective, the tool could be used more widely to allocate young adults with mental illness to the most suitable treatments and to ensure patients continue to receive the appropriate LOC as their treatment progresses.
Methods
Human research ethics
Ethics approval was granted for the study by the appropriate institutional ethics committee. A waiver of consent was granted by the Data Custodian to review the retrospective clinical information.
Study design
This retrospective, cross-sectional observational study was conducted across a state-funded tertiary adult community mental health service (CMHS) operated by an Australian Local Health Network (LHN) which serves patients aged 18–65 years. The study included all patients aged 18–24 years who were receiving mental health care on 30 May 2019, the cross-sectional time-point for data collection through case file review. This time point was deliberately chosen to fall well before the beginning of the COVID-19 pandemic.
Data
Data was extracted from each patient’s paper-based case notes and electronic records in the Community Based Information System (CBIS). Collected data included participant demographics (age and gender), primary mental health diagnosis, and comorbid conditions.
IAR rating
Two investigators (D.F. and P.L.) – senior mental health clinicians who were not involved in patient care – reviewed all eligible patients’ files and used information recorded in the most recent (prior to 30 May 2019) multidisciplinary-team-generated clinical case summary, to each IAR Domain from 0 to 4 based on the IAR Guidance. 7 The IAR total ratings and each IAR Domain ratings were tested for inter-rater reliability in 10 randomly selected consecutive cases and achieved kappa>0.8. Investigators then generated an IAR Level of Care (LOC) for each patient by mapping the Domain scores onto the IAR-DST logic. A rating of 4 (“Very Severe”) in Symptom Severity and Distress, Risk of Harm, or Functioning automatically generated LOC 5, while ratings of 0 or 1 in all Domains resulted in LOC 1. Other Domain variations were mapped to determine the appropriate LOC. IAR raters were blinded to service-use data, such as inpatient admissions, ED attendances, and face-to-face contacts.
Service use data
Retrospective service-use data was independently gathered for each patient’s current episode of care with the CMHT. Measures included the total duration of the current care episode (in months), as well as the number of Emergency Department (ED) presentations, inpatient admissions, and face-to-face contacts in the 24 months prior to the cross-sectional observation point. The investigator collecting service-use data (J.L.) was blinded to clinical data and designated IAR scores.
To adjust for each participant having varying durations of care at the cross-sectional data collection point, individual patient service data (ED presentations, Inpatient Admissions, and Face-to-Face Contacts) were converted to reflect a rate of event occurrence. Infrequent data points (ED Presentations and Inpatient Admissions) were converted to an event-per-year, while the high frequency data point of Face-to-Face contacts was converted to an occurrence per 3-month period (quarter).
Data analysis
Demographic, diagnostic, and LOC data were analysed to determine the prevalence of diagnostic clusters, comorbidity burden, and LOC distribution within the cohort. Patient data was stratified by LOC, and descriptive statistics were used to evaluate service-use rates across different LOCs. Incidence Rate Ratios (IRRs) were used to compare service usage per person-month of care for each LOC. LOC 5 was selected as the reference group and assumed to be representative of a severe and complex tertiary mental health patient. Microsoft Excel was used for data management and analyses.
Results
Clinical characterization of young adult patients by LOC
The study included 104 young adults, 56 men [54%] and 48 women [46%]. The mean [SD] age was 21.7 [1.7] (men 21.6 [1.7] and women 21.8 [1.7]). The mean length of young adult's episode of care with the CMHS, at the time of cross-sectional time point (30 May 2019) was 20.27 months [20.69 months], with a median of 11.5 months and a wide range from 1 to 106 months. The most prevalent diagnoses within the cohort were schizophrenia spectrum disorders (n = 38; 36%, of whom 76.3% were males) and Borderline Personality Disorder (BPD) (n = 27; 26%, of whom 70.4% were females) (Supplemental Figure 1).
Clinical characterisation according to IAR levels of care in 104 patients aged 18–24 years, attending a tertiary mental health service
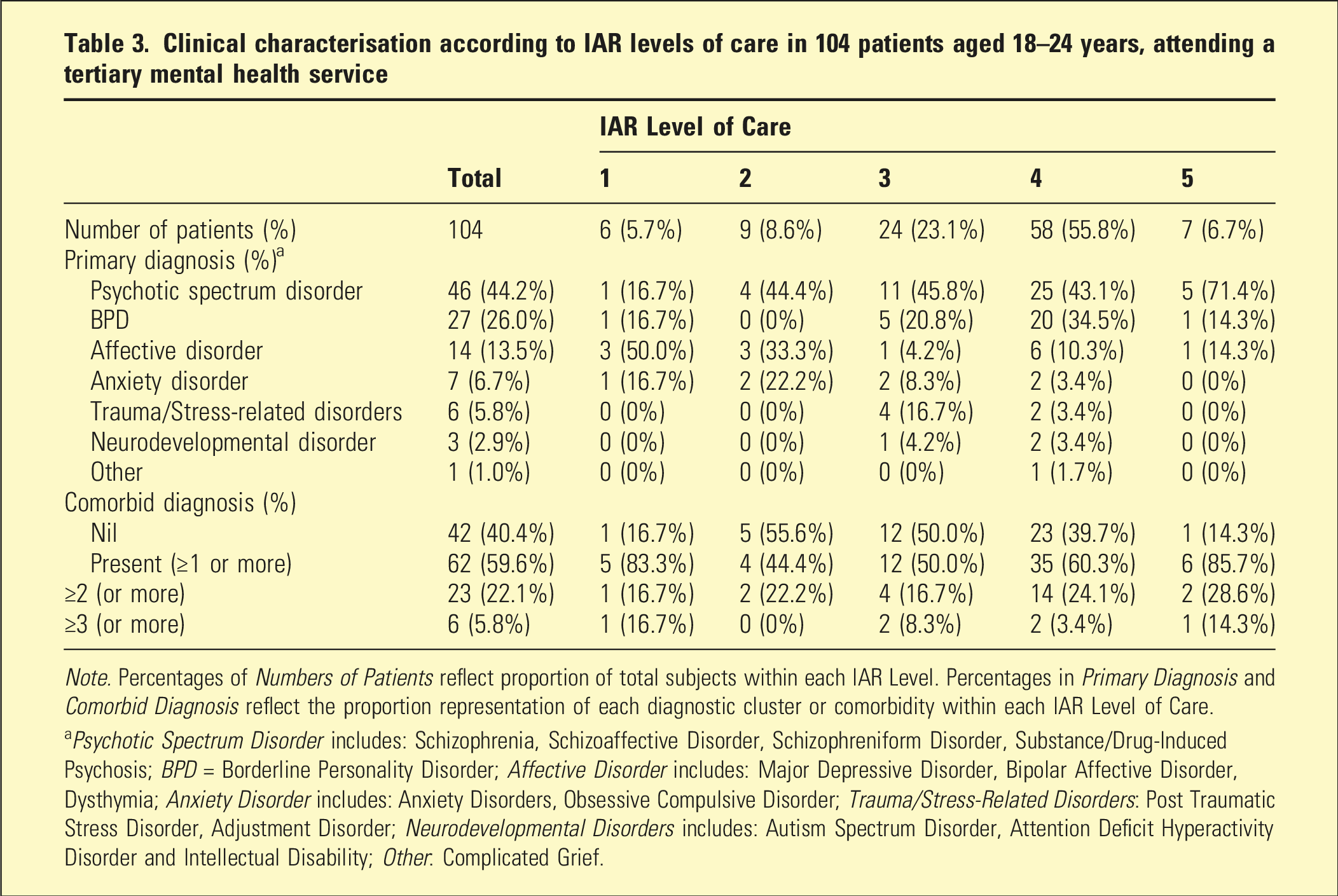
Note. Percentages of Numbers of Patients reflect proportion of total subjects within each IAR Level. Percentages in Primary Diagnosis and Comorbid Diagnosis reflect the proportion representation of each diagnostic cluster or comorbidity within each IAR Level of Care.
aPsychotic Spectrum Disorder includes: Schizophrenia, Schizoaffective Disorder, Schizophreniform Disorder, Substance/Drug-Induced Psychosis; BPD = Borderline Personality Disorder; Affective Disorder includes: Major Depressive Disorder, Bipolar Affective Disorder, Dysthymia; Anxiety Disorder includes: Anxiety Disorders, Obsessive Compulsive Disorder; Trauma/Stress-Related Disorders: Post Traumatic Stress Disorder, Adjustment Disorder; Neurodevelopmental Disorders includes: Autism Spectrum Disorder, Attention Deficit Hyperactivity Disorder and Intellectual Disability; Other: Complicated Grief.
Service usage according to the IAR LOC
Incidence rate ratios of service use per person-months of care
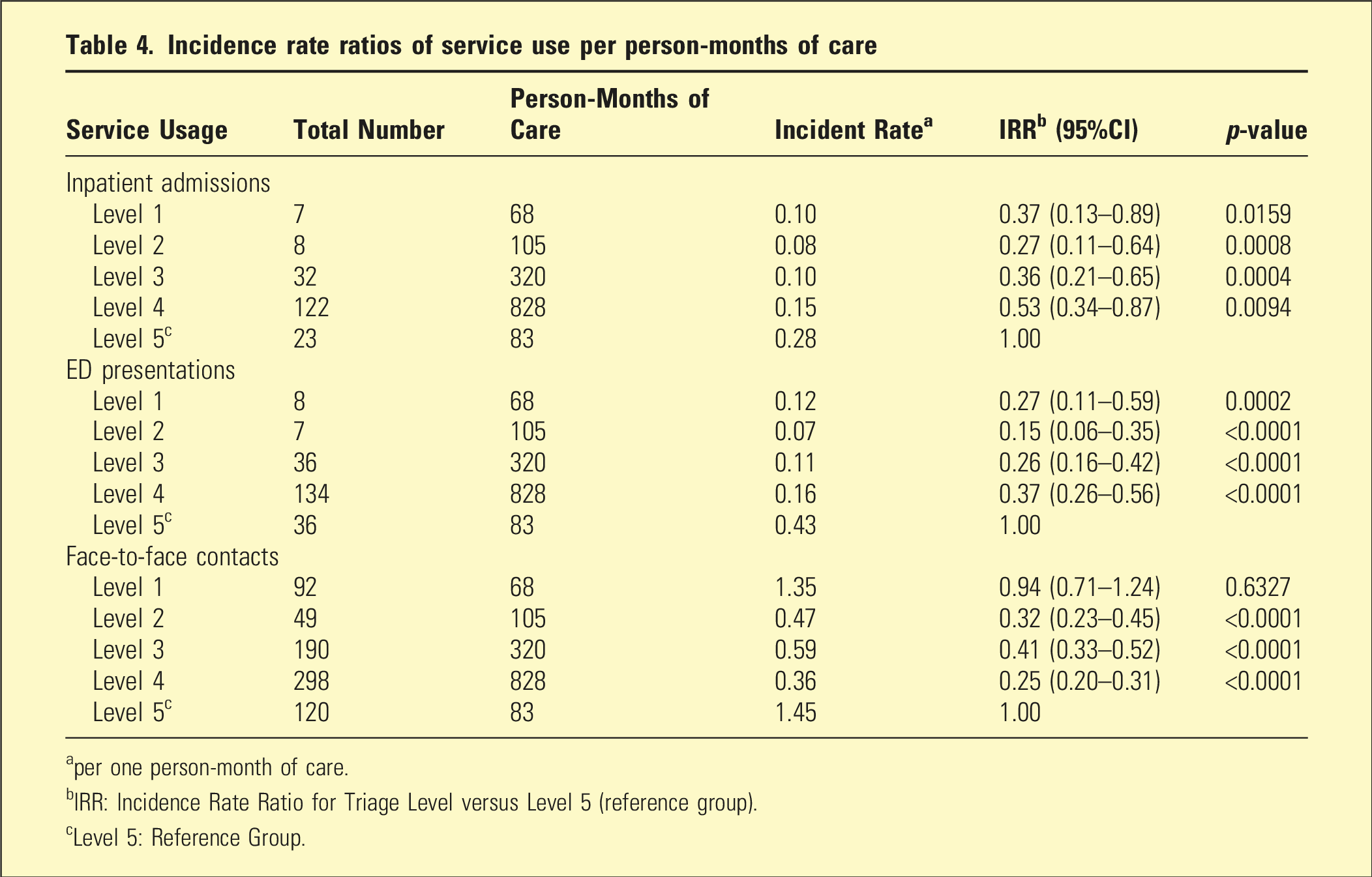
aper one person-month of care.
bIRR: Incidence Rate Ratio for Triage Level versus Level 5 (reference group).
cLevel 5: Reference Group.
With Level 5 as the reference group, all LOCs except Level 1 exhibited statistically significant lower IRRs compared to Level 5 (p < .05). For admissions and ED presentations, there was a progressive increase from Level 2 through Level 5; however, the differences between Levels 2, 3, and 4 were not statistically significant. In contrast, face-to-face contacts did not demonstrate a stepwise increase with rising IAR LOCs but were significantly higher in LOC 5 (see Table 4).
IAR domain ratings according to IAR LOC
Mean ratings for each IAR Domain were stratified by IAR LOC. Figures 1(a) and (b) illustrate that mean Domain ratings incrementally increase with higher IAR LOCs. In the Primary Assessment Domains, mean “Risk” ratings showed a relative increase in importance, particularly in LOC 5, compared to other Domains that increased more linearly across the five LOCs. In the Contextual Domains, “Engagement” and “Stressors” also gained relative importance at higher IAR LOCs. Mean domain scores according to Initial Assessment and Referral (IAR Level).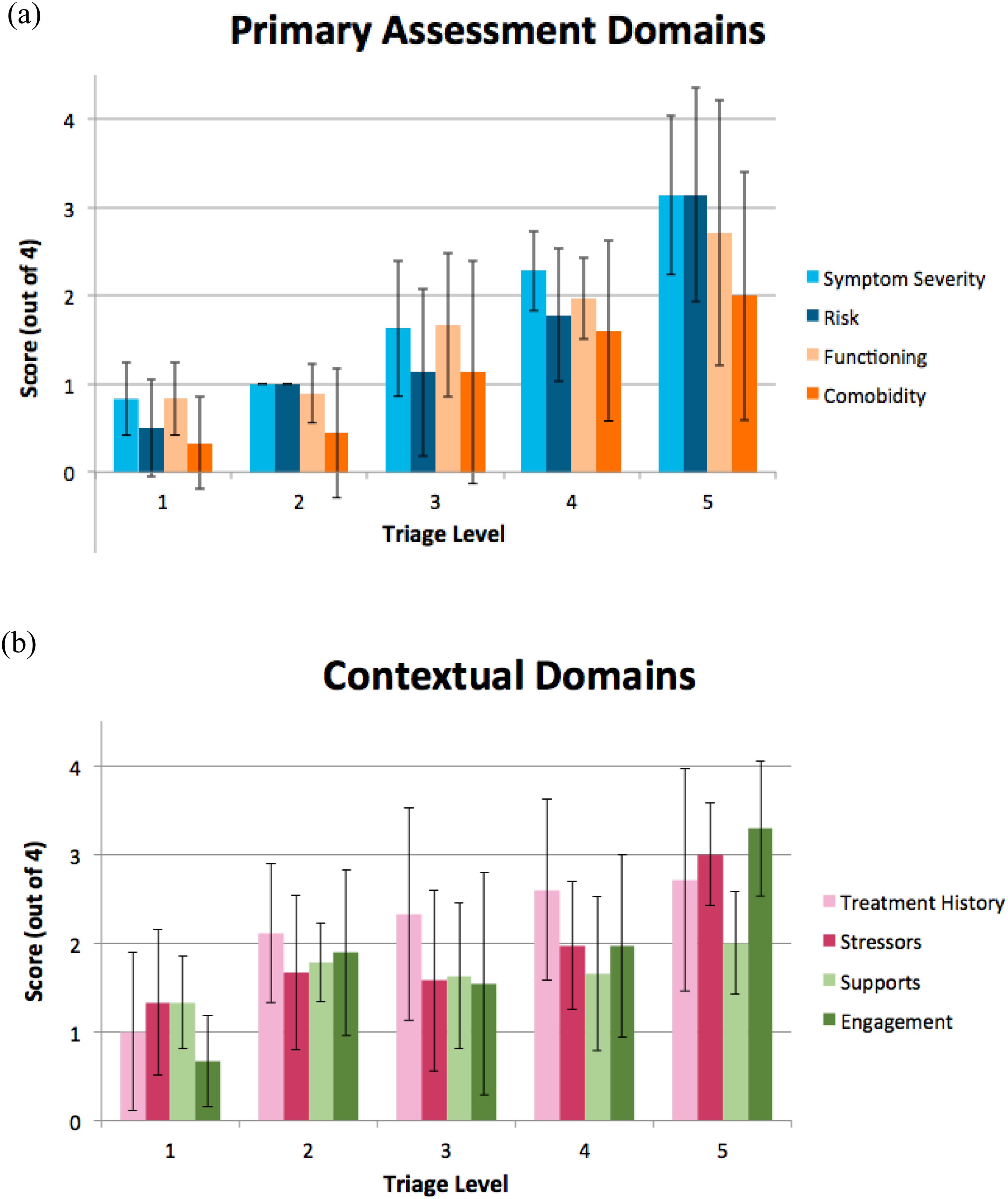
Discussion
To our knowledge, this study is the first to report the application of the IAR-DST for young adults with significant mental illness attending publicly funded, tertiary community mental health teams (CMHTs). We aimed to explore the applicability and utility of the IAR for assessing ongoing service need in specialist services by stratifying and describing a retrospective cross-sectional sample of tertiary community mental health patients currently receiving treatment. Nearly 63% of young adults attending these services fell into the IAR LOC that would trigger a recommendation for specialist or high-intensity care (i.e. LOC 4 or 5). However, only a small proportion of participants were classified in Level 5 (7%), indicating an acute mental health crisis, debilitating multi-morbidity, or chronicity. The low numbers in this IAR category are perhaps not surprising, given our assessment occurred during ongoing treatment rather than the acute point of service entry.
Over 37% of patients did not meet the recommended level of care for a tertiary mental health service (i.e. LOC 3 or below), suggesting that some young adults may be over-serviced or retained too long within specialist CMHT. It is also possible that the IAR-DST is failing to detect aspects of the patient situation that do indicate a need for ongoing specialist care. Thus, the IAR tool may be underestimating the LOC required for this tertiary cohort, which is already enriched for higher complexity. Future studies should further investigate this issue and explore whether similar patterns of lower-than-expected IAR Levels are observed in patients receiving treatment across the full range of stepped care services and age groups. If so, then the IAR may need recalibration for use in assessing patients in ongoing treatment.
Considering the primary diagnoses associated with LOCs 4 and 5, it is not surprising that Psychotic Spectrum Disorders and Borderline Personality Disorder (BPD) were the most common. This aligns with the well-recognized complex needs and high service utilization of individuals with psychotic illnesses and severe personality disorders. 10 In LOCs 2 and 3, psychotic illnesses were also the most prevalent primary diagnoses (44.4% and 45.8%, respectively). It is crucial to remember that psychotic illnesses are often complex, lifelong, and disabling disorders characterized by a chronic pattern of relapse. 11
The high proportion of patients with BPD in LOC 4 likely reflects individuals with severe personality pathology (e.g. dissociative episodes or chronic suicidality) and/or those in crisis situations that may involve suicidal or self-harming behaviours, often necessitating intensive specialist service intervention. Although most patients with BPD were triaged to a high-intensity LOC, 22% were classified as LOC 3 or lower. This less complex cohort likely represents patients with stable BPD or those primarily accessing specific psychological therapies (e.g. Dialectical Behavior Therapy) within public mental health services.
The higher prevalence of Affective, Anxiety, and Trauma and Stress-Response Disorders at lower LOCs may be attributed to two factors: the resolution of an acute crisis presentation that subsequently revealed a mild to moderate underlying disorder, or the added complexity of comorbid conditions impacting on the recovery journey. The latter hypothesis is supported by high rates of comorbidity observed across all IAR LOCs, which aligns with the recognized cumulative burden and treatment resistance associated with comorbid difficulties in young adults. 12
The IAR LOCs were associated with independently assessed metrics of service use. Higher service use (duration of care, ED presentations, inpatient admissions) was strongly linked to IAR LOC 5 compared to lower IAR LOCs, indicating that the tool is well-suited for identifying young adults with the highest acuity, complexity, and service needs. For LOCs 2–4, service use increased incrementally, although differences between levels were not statistically significant.
The lack of a stepwise increase in IRRs with Face-to-Face contacts may be attributed to crisis presentations that, while initially requiring intensive clinician involvement, later revealed low to moderate complexity. Additionally, this pattern may reflect illnesses that have decreased in severity but still necessitate specialist mental health support to maintain wellness.
Mean individual IAR Domain ratings demonstrated incremental increases with each rise in IAR LOC. Notably, the importance of “Risk” and “Engagement” increased significantly, particularly at LOC 5. This finding supports the common clinical observation that a young adult’s level of risk, insight, and engagement with treatment are critical factors influencing retention in a tertiary community mental health setting.
Our study demonstrated that the IAR-DST can stratify young adults into stepped levels of clinical severity that reflect their service usage. A key strength of the tool is its multidimensional evaluation of a young adult’s clinical presentation, aiding in case formulation and treatment planning. Our results suggest the IAR-DST may be useful for periodically re-evaluating a young adult’s illness severity and complexity, facilitating appropriate transitions of care. However, for practical implementation, services for young adults must be structured in an integrated manner, ensuring smooth transitions between services that do not jeopardize patient engagement.
Limitations
The most notable limitation of this study was the reliance on retrospective case note information to rate IAR-DST Domains, rather than conducting clinical interviews as intended by the IAR Guidance. Further, this study utilised the IAR-DST to assess service needs in patients engaged in ongoing treatment, rather than at the point of referral.
We were unable to assess the full age range that would encompass “youth” within CMHS (12–24 years), limiting our ability to comment on age-related differences that may have emerged if a younger cohort of adolescents had been included. Therefore, these results cannot be generalised to broader youth mental health services. Moreover, the cross-sectional nature of the study resulted in a heterogeneous cohort of patients at different stages of care, preventing analyses of potential changes in IAR LOC ratings over time. The lack of prospective or longitudinal data is a limitation of this study. Further research is needed to apply the tool prospectively to accurately evaluate its effectiveness across various time points, including transitions between levels of care.
Conclusion
This study represents the first application of the Initial Assessment and Referral Decision Support Tool (IAR-DST) to young adults receiving treatment in a tertiary CMHS. Our results suggest that one-third of patients whose case notes were included in this study would qualify for lower levels of service intensity. However, it is also possible that the IAR-DST requires recalibration for patients receiving ongoing specialist mental health care.
The diagnoses qualifying for involvement in the service (i.e. IAR LOC 4 or 5) were predominantly Psychotic Spectrum Disorders and Borderline Personality Disorder (BPD), complicated by high comorbidity. This aligns with existing literature highlighting the significant burden and complexity associated with comorbid illnesses in achieving recovery from mental illness. The IAR-DST appeared to capture increasing service use with each increasing LOC, particularly heightened service needs of individuals triaged into Level 5 (high intensity, specialist service).
There has been substantial investment in the IAR-DST. Overall, the tool demonstrated clinical utility in characterizing and triaging young adults with severe mental illness within a stratified model of mental health care. It has potential to benefit both primary and tertiary health providers, assisting in the assignment of young adults to the most appropriate services. Further prospective evaluation as a mechanism for facilitating reviews and transitions within services would be helpful in determining its utility beyond primary care.
Supplemental material
Supplemental Material - The utility of the Australian primary health networks’ initial assessment and referral decision support tool (IAR-DST) for cross-sectional assessment of care needs in young adults attending a tertiary community mental health service
Supplemental Material for The utility of the Australian primary health networks’ initial assessment and referral decision support tool (IAR-DST) for cross-sectional assessment of care needs in young adults attending a tertiary community mental health service by Jessica Lowe, Damon Fenech, Paula Larsen, Alexander Phillips-Hughes, Cherrie Galletly, and K Oliver Schubert in Australasian Psychiatry
Footnotes
Acknowledgements
The study was conducted as part of The Royal Australian and New Zealand College of Psychiatrists fellowship training Scholarly Project.
Ethical considerations
This study received ethical approved by the Central Adelaide Local Health Network Ethics Committee (ref 13997) with a waiver of consent to review the retrospective clinical information.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.