
Abstract
Women in Victoria experience significantly higher rates of mental illness than men, particularly among culturally and racially marginalised women and those exposed to trauma, poverty, and family violence. Despite this, mental health services and research have historically relied on male-centred models, with mixed-gender inpatient settings often failing to provide safety or trauma-informed care for women. In response to the Royal Commission into Victoria’s Mental Health System, the Women’s Recovery Network (WReN) was established as a women-only, trauma-informed, and gender-affirming inpatient service. Delivered through a public–private partnership and co-designed with lived experience, WReN offers a recovery-oriented, dialogical model that prioritises safety, choice, and collaborative care.
Evidence and experience clearly indicate the need for an improved model of care in women’s mental health services. Traditional models in the mixed -gendered public health system are not able to meet women’s particular needs, including their gendered needs and need for physical and sexual safety.
In Victoria, 36% of women have been diagnosed with depression and anxiety by a doctor in their lifetime, compared with 23.7% of men. In 2019, 21% of women reported experiencing, psychological distress compared with 15.6% of men. 1
These gendered differences are more profoundly experienced by women who are culturally and racially marginalised. This includes women from non-English speaking backgrounds, and Aboriginal and Torres Strait Islander women all of whom experience mental illness differently to women from English speaking backgrounds and non-Indigenous backgrounds. 2
The complexities for women and mental health treatment are further compounded by the fact that women are more likely to live with poverty and family violence, compared with men: issues which have their own detrimental impacts on women’s mental illness. 3
In short, women are at higher risk of poor mental health and mental illness through their greater exposure and vulnerability to gendered social, economic, and environmental circumstances. Major woman-specific life transitions such as pregnancy, motherhood and menopause, alongside unequal economic and social conditions contribute to their risk and character of mental illness for women. 4
When considering the importance of gender as a basis for designing mental health care for women it is important to consider that compared with men, women are more likely to:
Women’s experiences have, until recently, been largely absent due to historical exclusion in medical research with strong evidence that traditional mental health approaches, including models of care and staff training principles, have been developed for men and generalised to be used with women patients. 8
The outcome for women requiring inpatient mental health care is that they are in mixed-gendered settings which, evidence demonstrates, result in negative experiences for those women. There is a high prevalence of sexual safety incidences against women in mixed-gender inpatient mental health units from other consumers and staff, with most incidents initiated by men. Mixed-gendered inpatient settings present an unacceptable risk of harm for women and effectively act as a barrier for women in accessing mental health services. 1
Effective treatment for women depends on offering them safe and respectful care based on their particular experiences and needs. It is evident that existing mixed-gender mental health services do not provide this.
Initiatives such as Kulkarni and colleagues 9 campaigning for women only areas within mixed-gender public mental health settings resulting in fewer violent incidents against women. However, due to bed shortages and other administrative reasons this gender segregation has resulted in breaches with ongoing dangers to women’s experience and feeling of safety which act as a barrier to women accessing treatment and the outcomes of care. Lack of gender-focused staff resourcing and training in the inpatient setting also contributes to increasing women’s vulnerability to gender based violence, and in particular to sexual safety violations.
The Royal Commission into Victoria’s Mental Health System 10 raised issues around the specificity of women’s experience – the Women’s Recovery Network (WReN), a statewide women’s mental health service was established in response to the Commission’s findings. The Royal Commission heard accounts of the sexual assault and harassment of women with vulnerable mental health during their stays in Victorian mental health inpatient services. These experiences echoed the findings of the ‘Right to be Safe’ report by the Victorian Mental Health Complaints Commissioner which found that around 80% of complaints about sexual safety breaches on inpatient mental health wards were made by women, and over 75% of alleged perpetrators were men. 11
The Royal Commission considered the issue of gender-based separation and discussed the need for women-only inpatient services which could be sensitive to the impact of women’s sex-specific bodily and life experiences and create a unique women’s experience of mental illness. This included examination of the need for better understanding how lived experiences of trauma may have affected a woman’s support needs before entering the service and the need to ensure that disclosures of violence are never trivialised, dismissed or met with disempowering responses from staff.
WReN was established to facilitate the Royal Commission`s Recommendations and works alongside other specialist mental health services for women based in metropolitan Melbourne, 12 however, there is limited access for women in regional areas. WReN is a partnership between Alfred Health, Goulburn Valley Health (GVH) and Ramsay. The women within the GVH catchment include a diverse population with a large Aboriginal and multicultural population who, as discussed above, are at greater risk of experiencing mental illness.
In responding to the identified needs around women’s services, WReN offers a model previously unavailable in Victoria, enabling public hospital mental health consumers to access gender-focused and trauma-informed voluntary treatment in a public health setting. WReN provides assessment, treatment and support for women over 18 years of age who require treatment for mental illness. This includes women who have experienced trauma and sexual abuse, women presenting with eating disorders, and women experiencing perinatal mental ill health. Crucially, the WReN model of care has been co-designed in consultation with women with lived experience of the mental health system. The design also depends on the delivery of a staff education program focused on gender safety, which includes the Safewards Model which commits to reduce the use of the Mental Health Act and restrictive interventions. WReN seeks to train and develop a specialist workforce that can deliver gender-specific and trauma-informed care (Figure 1). Hub and Spoke model of WReN.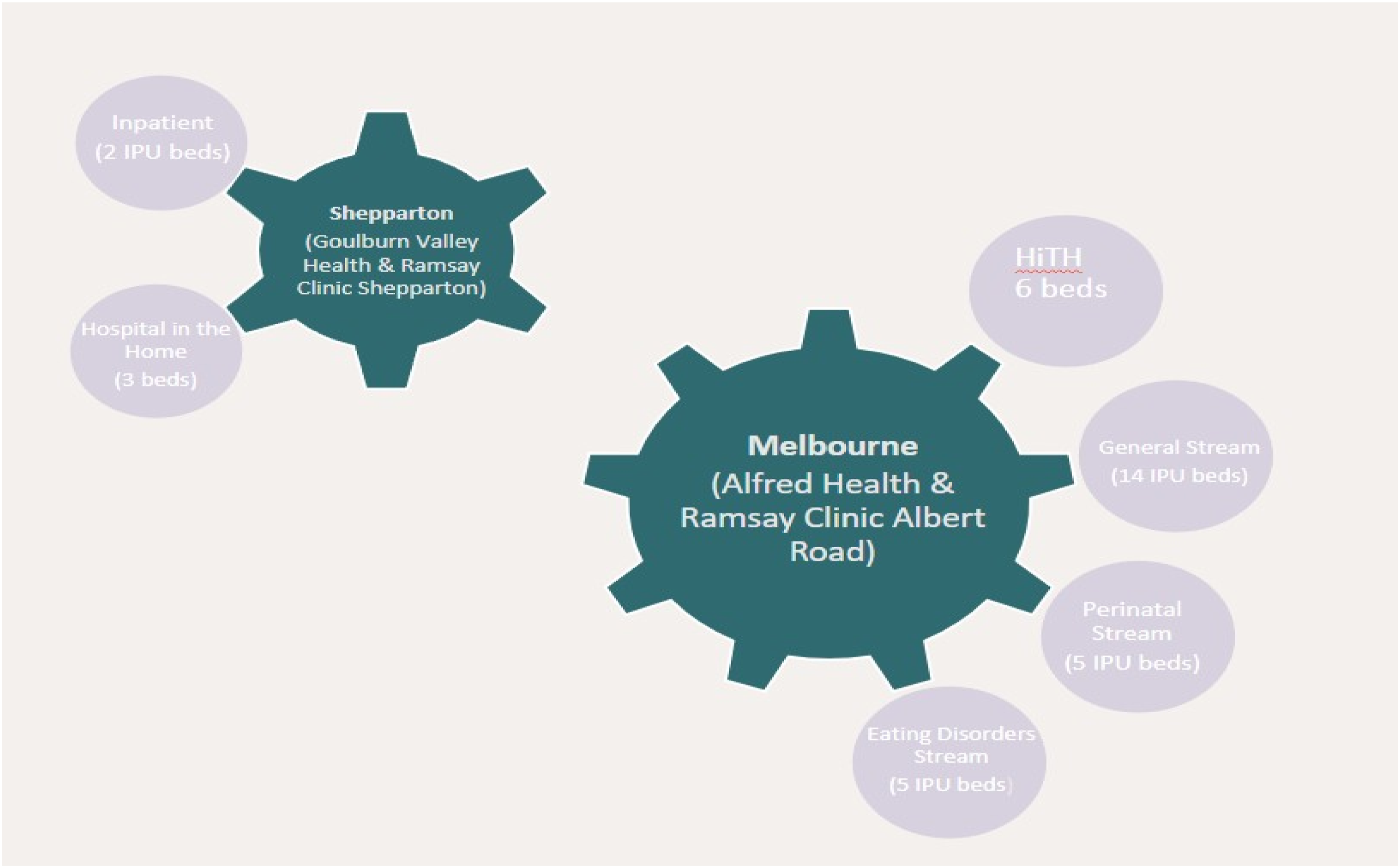
The objective of WReN is to provide both choice and flexibility in the way care is delivered to consumers that is safe, compassionate and responsive to their needs. It seeks to do so through a dialogically informed model – Open Dialogue – as a foundational component in care provision.
Open Dialogue is an innovative clinical and service organisation approach, developed within the mental health service setting of Western Lapland in Finland during 1980s. Initially developed as outpatient response to acute crises, Open Dialogue involves having network meetings with the health-affected individual, their family, other natural supports and any other professionals involved. 13 The model has expanded to inpatient treatment settings and inpatient units adopting this approach have found that the transparency of the model increases mentalising on the part of clinicians, transforms the culture of an inpatient unit, and reduces rounding times based on the impact of consumers being involved in decision-making processes. The model supports working with individuals and their families, in a system-focused approach such that participants in that system feel heard, respected and validated. This approach recognises the rights and roles that individuals have in making decisions about their care – ‘no decision about me without me’ – while grounding work in the reality of the affected person’s network of choice (e.g. family). It promotes human rights and recognises the importance of relationships and strong therapeutic alliance in mental health recovery. It instils hope for, and commitment to, individuals meeting their goals for health and wellbeing and being able to live fulfilling independent lives. Importantly, it also promotes care and compassion for the health care team, recognising their importance as part of the consumer’s care system, and the encouraging them to support one another and respect every team member. Within this model, clinical discussions within the inpatient setting are, as much as possible, conducted in the presence of the woman receiving care, and treatment decisions are made collaboratively with the consumer and the network of their choice.
This dialogical approach was adopted by WReN based on the recognition that it can be structured to effectively promote the specific experiences of women in that it promotes recovery-oriented care and aligns with trauma informed care 14 to improve women’s feeling of safety and empowerment.
The establishment of WReN relied on an extensive co-design process. The co-design consultation process included participation from 131 women with lived experience, as well as carers, family members and mental health clinicians.
Feedback was also received and incorporated from organisations including Perinatal Anxiety and Depression Australia (PANDA), Tandem, Victorian Mental Illness Awareness Council (VMIAC), Eating Disorders Victoria (EDV) and Women’s Health Victoria. The recommendations and process insights derived from the co-design process continue to inform and shape the service delivery model. A continuous incorporation of WReN consumers’ lived experience is achieved through an Engagement and Participation group, which comprises consumers and carers. The group creates an ongoing feedback loop which keeps WReN practices in a positive, directly consumer-informed, ongoing development trajectory.
We strongly believe – and there is early data to show – that the co-design process and the incorporation of feedback from consumers and carers improves the experience of care for participants and their family and all those involved in a consumer’s network of care. Further, it helps to improve, refine and create better strength and flexibility in treatment services.
Ultimately WReN’s aim is to offer mental health services that are tailored to women and that reach women in ways that resonate and respond to women in ways that have not, until now, been available in the public health system. The early indicators are promising. In the words of one consumer ‘I will definitely fail at adequately expressing my gratitude for the help and support I have received here, but I’ll try anyway. The staff and environment at Wren have provided the most meaningful support I have ever received for my mental health in my 42 years of life. Thank you all for everything, I am leaving feeling more equipped to be safe, and more empowered to begin to make changes to the lifelong harmful patterns I brought in with me. I hope you all understand the level of impact your work has on people’s lives.’
Footnotes
Acknowledgements
Dr Mal Hopwood & Dr Chloe Stella.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.