
Abstract
Objectives
Zuclopenthixol acetate (ZA) is commonly used in psychiatric intensive care units (PICUs) to manage acute behavioural disturbance (ABD). Despite its clinical utility, monitoring practices remain inconsistent, creating issues such as oversedation and cardiac risk. This study aimed to evaluate compliance with existing Queensland ABD guidelines, benchmark standards, and develop and pilot a proposed revision to the Queensland state guideline to strengthen monitoring and improve patient safety.
Methods
In this quality improvement project, a proposed ABD management guideline was synthesised from key guidelines identified by literature review. Baseline ZA practice was assessed in a regional PICU against the proposed ABD guideline. Following staff education and guideline implementation, pre/post outcomes were evaluated.
Results
Eighty-eight patients were included. Following ABD guideline implementation, compliance improved significantly for pre-ZA blood tests (49.3% to 84.2%, p < .01) and ECGs (43.5% to 83.3%, p < .01), and at discharge (ECG 33.3% to 83.3%, p < .01). Baseline documentation improved from 30.9% to 83.3% (p < .01). Improvements were consistent across patient demographics, except for higher discharge ECG completion in non-Indigenous patients (p = .04).
Conclusions
Implementation of the proposed ABDM guideline markedly improved monitoring and documentation of ZA use. These findings provide evidence for state-wide adoption to support safer and more consistent care.
The management of acute behavioural disturbances (ABD) in psychiatric intensive care units (PICUs), frequently involves the use of Zuclopenthixol Acetate (ZA), an injectable antipsychotic medication known for its rapid tranquilizing effects. 1 Despite its clinical utility, the use of ZA presents significant challenges, including marked variability in prescribing practices, 2 inconsistent physical health monitoring, and a lack of uniformity amongst established ABD guidelines. 3 These issues are compounded by the drug’s complex pharmacodynamic profile, 4 which includes a delayed peak effect (24-36 hours) and contraindications in neuroleptic-naive patients, heightening the risk of adverse outcomes such as prolonged sedation lasting up to 7 days, cardiovascular complications, and neuroleptic malignant syndrome (NMS).
The contentious nature of ZA’s use is underscored by documented gaps in pre-prescription assessments and post-administration monitoring, despite the usual requirement for consultant psychiatrist authorisation. 5 Variability in monitoring guidelines across healthcare services further exacerbates potential safety risks, particularly concerning oversedation, cardiac events, and prolonged QT intervals, which may precipitate Torsades de Pointes. Queensland Health guidelines recognise the potential for these cardiac adverse reactions; however, it is not required for an ECG to be performed prior to the initiation of psychotropic agents such as ZA, 3 unlike other state guidelines such as those from Western Australia. 6
As the Queensland Health ABD management guidelines are due for review, a quality improvement project was undertaken to evaluate and optimise the administration of ZA. The impetus for this initiative arose from pharmacy-led recommendations advocating for routine electrocardiograms (ECGs) prior to ZA administration, in recognition of the established risk of QT interval prolongation associated with antipsychotic medications.
The aims of this study were to: - Evaluate the compliance of ZA administration within the study site with existing Queensland Health guidelines for ABD management. - Evaluate documentation practices related to ZA administration and physical health monitoring. - Benchmark ZA administration and monitoring guidelines from other state and governing bodies. - Create a proposed update to the Queensland Health ABD management guideline (referred to forthwith as the ‘proposed ABDM guideline’. - Pilot education and implementation of the proposed ABDM guideline in our regional health service.
Methodology
This single-centre study was conducted in the PICU of a regional public teaching hospital. The study was approved by the Central Queensland Hospital and Health Service Human Research Ethics Committee (EX/2023/QCQ/91382). The SQUIRE guidelines for reporting quality improvement studies were used. 7
This study employed the plan-do-study-act (PDSA) cycle as its methodological framework, a widely recognised iterative model for quality improvement in healthcare. Utilising the PDSA cycle enabled the study team to systematically measure current practice, implement targeted changes, evaluate their effectiveness, and adapt strategies accordingly. This iterative process supports continuous quality enhancement and ensures that interventions remain responsive to evolving clinical needs and safety standards.
Comparison of existing and proposed ABDM guidelines
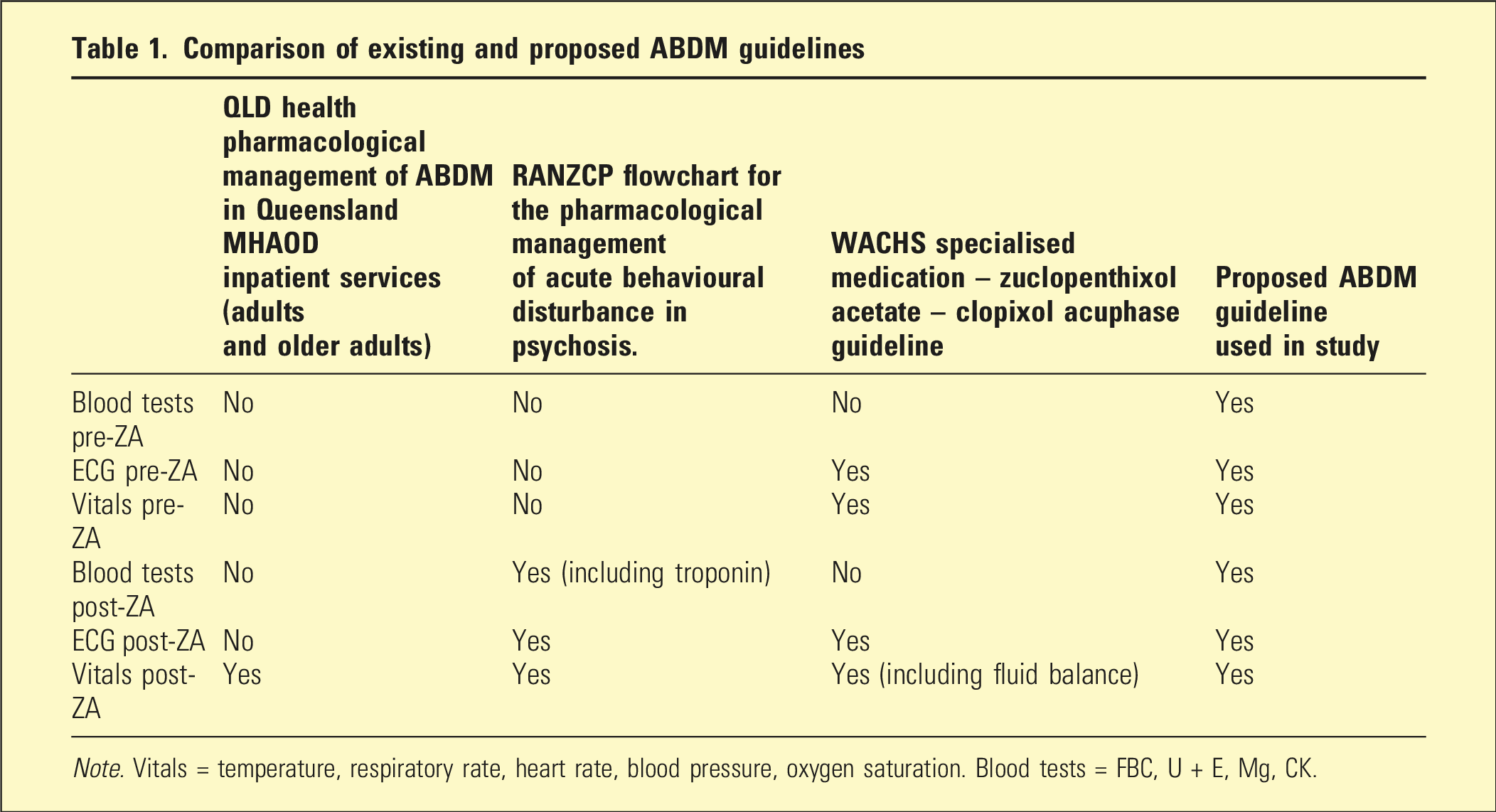
Note. Vitals = temperature, respiratory rate, heart rate, blood pressure, oxygen saturation. Blood tests = FBC, U + E, Mg, CK.
The WACHS ZA guideline 6 was selected as the primacy reference for the development of the proposed ABDM guideline, owing to its structured and systematic approach. However, it lacked recommendations regarding blood investigations, which are particularly important given the risk of NMS associated with ZA. Vital sign monitoring prescribed by the guideline recommended every 15 minutes for the first hour, then 1-hourly for 3 hours, then 2-hourly for 4 hours, then 4-hourly thereafter for 48 hours. However, this was considered impractical for implementation in patients with behavioural disturbances. In summary, the WACHS guideline was deemed overly stringent and not feasible in practice, whereas the Queensland Health guideline was insufficiently comprehensive, and the RANZCP guideline 9 did not address baseline assessments. This decision was reached following consultation with key hospital stakeholders including the Director of Pharmacy, the MHAOD Clinical Director, psychiatrists, psychiatry registrars, and senior mental health nursing staff keeping in mind the process of development of guidelines for the use of ZA. 10
Drawing on the WACHS guideline, the proposed ABDM guideline emphasised frequent and structured physical health monitoring, mandatory ECG documentation, and clear escalation pathways for clinical deterioration (see Figure 1). Proposed Acute Behavioural Disturbance Management guideline developed from synthesis of guidelines identified in literature review.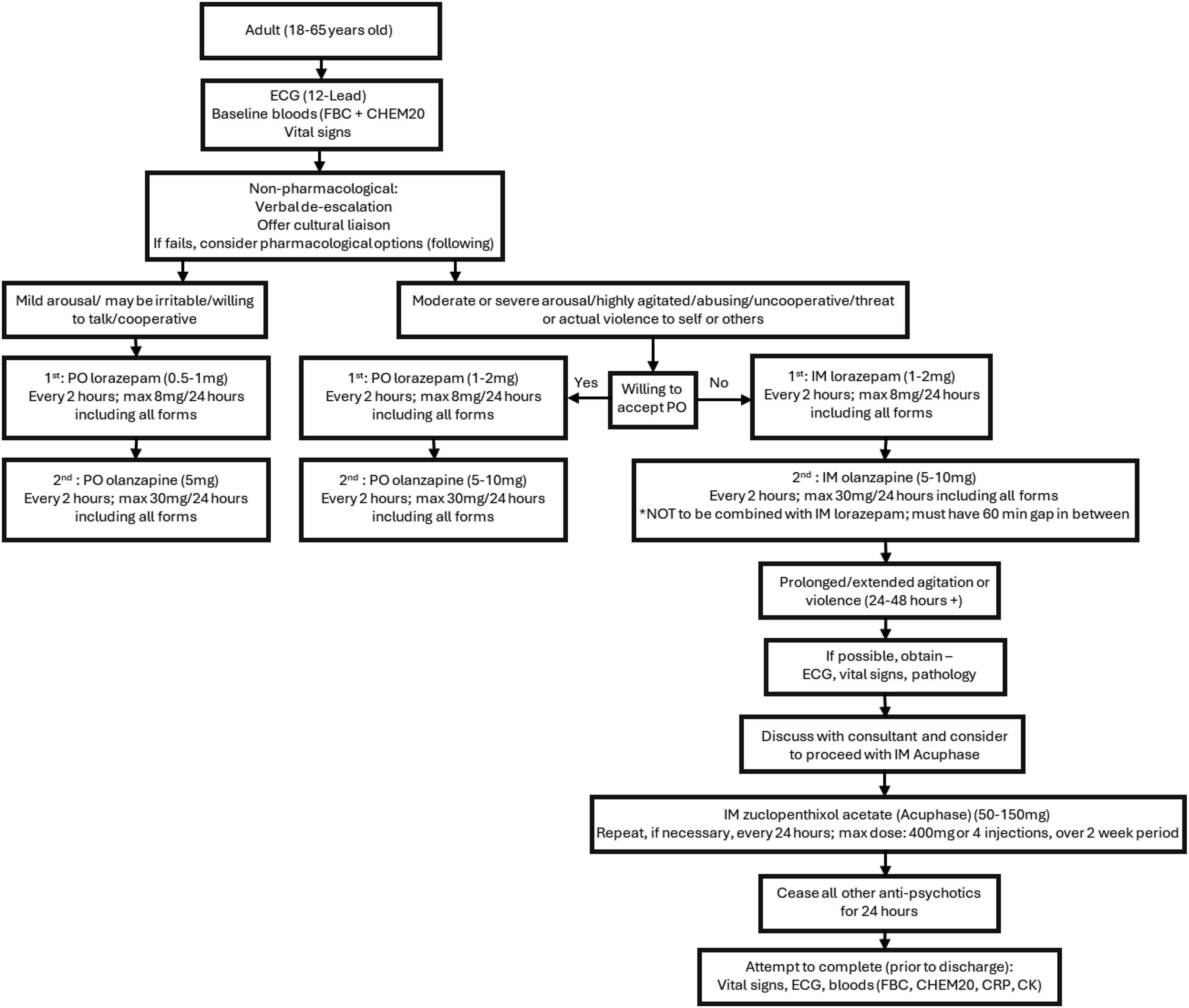
Next, a retrospective audit of medical records from January 2019 to December 2021 was undertaken, assessing compliance with the new guideline for the prescription, administration, and monitoring of ZA.
Finally, implementation of the proposed guideline was undertaken, and this involved comprehensive staff education, including the evidence-based rationale for frequent monitoring, case-based learning on the risks of inadequate observation, and practical training in the use of new audit tools.
The appropriateness of ZA administration and monitoring was evaluated against the proposed ABDM Guideline in both the pre- and post-intervention periods. An interrupted time series analysis compared baseline (pre-intervention) and post-intervention data for all patients prescribed ZA (n = 88). In this way, we assessed the implementation and introduction of the proposed ABDM guideline and targeted education. 5
Data collected included patient demographics, documentation of physical health monitoring (including ECGs), and compliance with the proposed ABDM guideline. Statistical analysis was performed using SPSS 26. Categorical variables were reported as frequencies and percentages, with comparisons between groups conducted using Chi-square or Fisher’s exact tests. Statistical significance was set at p < .05.
Results
Patient demographic overview
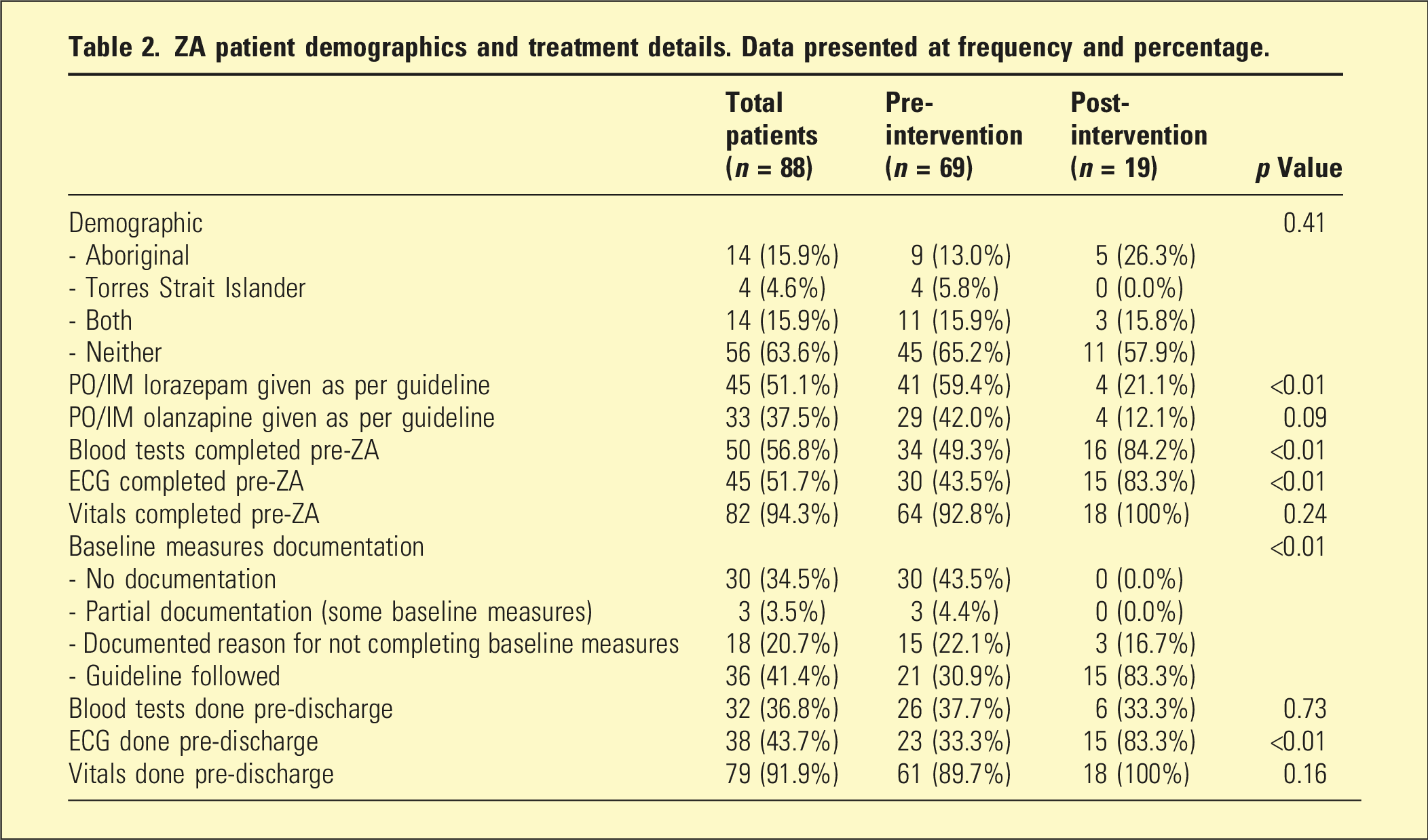
ZA patient demographics and treatment details. Data presented at frequency and percentage.
Pre-intervention audit results
Prior to the intervention, compliance varied depending on the ABDM guideline applied. Of the 69 patients in the pre-intervention group, 59.4% received PO/IM lorazepam as per the guideline, while 42.0% received olanzapine according to the guideline. In addition, pre-treatment assessments showed that 49.3% of patients had blood tests completed prior to ZA administration, and 43.5% had an ECG completed. Baseline vital signs were recorded for 92.8% of patients. However, documentation of baseline measures was inconsistent: only 30.9% had full protocol documentation, 22.1% had a documented reason for not completing baseline measures, and 43.5% had no documentation at all. At discharge, 37.7% had blood tests completed, 33.3% had an ECG, and 89.7% had vital signs recorded.
Post-intervention results
Following the intervention, several key process measures demonstrated significant improvement. Among the 19 patients in the post-intervention group, the proportion who had blood tests completed prior to ZA increased to 84.2% (p < .01), and those with a pre-ZA ECG rose to 83.3% (p < .01). Vitals were recorded for all patients prior to ZA administration. At discharge, 33.3% had blood tests completed, 83.3% had an ECG (p < .01), and 100% had vital signs recorded. However, guideline adherence for lorazepam and olanzapine administration declined post-intervention, with only 21.1% and 12.1% of patients, respectively, receiving these medications as per the guideline.
Treatment compared by patient demographics
No significant differences were observed in most key monitoring outcomes between Aboriginal and Torres Strait Islander and non-indigenous patients during the post-intervention period. Compliance with administration of PO/IM lorazepam and olanzapine as per protocol, completion of pre-ZA blood tests, documentation of baseline observations, and completion of discharge blood tests and vital signs were all similar across groups (p > .05). However, completion of ECG monitoring prior to discharge was modestly higher in the non-indigenous group (p = .04). Importantly, overall ECG monitoring rates remained higher in both groups than pre-intervention levels. Taken together, these findings indicate that the improvements achieved following implementation of the proposed ABD management guideline were broadly equitable.
Discussion
This quality improvement project identified substantial pre-intervention gaps in the monitoring and documentation of ZA for acute behavioural disturbance in a regional psychiatric intensive care setting. Inconsistency in clinical guidelines 2 across jurisdictions contributed to this irregularity, 12 as clinicians navigated conflicting standards from sources such as the Queensland Acute Behavioural Disturbance Guideline 3 and international bodies like the Cochrane Collaboration. 13 As such, clinical practice was largely influenced by the prescriber’s personal experience, organisational culture, and historical habits, rather than by robust evidence or standardised guidelines.
The improvement seen after implementation of the proposed acute behavioural disturbance management guideline is therefore best understood not simply as a documentation gain, but as evidence that clearer expectations, structured monitoring requirements and focused education can shift practice towards safer and more standardised care. The largest changes were seen in objective physical health monitoring, particularly blood testing, ECG completion, and vital sign recording. This is important because the safety of ZA cannot be separated from the systems used to assess patients before and after administration. The environment of inconsistent monitoring and documentation posed risks to patient safety and limited the ability to systemically evaluate outcomes or improve care. 14
These findings are consistent with the broader literature showing that monitoring after rapid tranquillisation is frequently suboptimal in routine mental health practice. In a national UK audit-based quality improvement programme, Paton et al. found that the minimum recommended level of post-rapid tranquillisation physical health monitoring was documented in only one in five episodes, despite clear guidance and the recognised risks associated with parenteral sedation. 15 Their findings suggested an important gap between guideline standards and real-world implementation, particularly when patients remain highly distressed or difficult to engage. Similarly, literature on antipsychotic-related physical health monitoring has shown that monitoring rates often remain inadequate despite longstanding recommendations, reinforcing that the challenge is not only whether guidance exists, but whether it is operationalised in a way that is feasible and sustained in everyday psychiatric practice.
An important finding in the current study is that improvement was not uniform across all domains of acute behavioural disturbance management. While compliance with monitoring and documentation requirements improved after implementation of the guideline, adherence to lorazepam and olanzapine recommendations was lower in the post-intervention period. This may indicate that implementation success was concentrated around the most visible and auditable components of the intervention, namely, ZA-related monitoring, rather than across the full pharmacological pathway for acute behavioural disturbance. 12 This does not diminish the safety gains observed, but it does suggest that future iterations of the guideline and associated education should more explicitly reinforce the place of first-line agents and the broader sequencing of care so that emphasis on ZA safety does not inadvertently narrow attention to other evidence-based management steps.
Our findings also align with prior Australian work by Vellar et al 16 in the prescribing and monitoring of ZA in regional mental Australian mental health services. This previous study systematically assessed ZA prescribing practices, identified critical safety concerns – particularly regarding high-dose use and lack of monitoring – and demonstrated that targeted interventions could lead to safer, more evidence-based clinical practice. Viewed alongside that study, the present project adds to the body of evidence highlighting the importance of embedding audit cycles and education to improve medication safety standards. This is particularly relevant in settings where prescribing practices may be shaped by local custom, workforce experience and service pressures as much as by formal evidence-based guidance. The study revealed a significant overrepresentation of Aboriginal and Torres Strait Islander patients among those receiving ZA for acute behavioural disturbance. While Aboriginal and Torres Strait Islander peoples comprise only 6% of the local population, 11 they accounted for 36.4% of the total patients in this study. This finding should be interpreted carefully, as we did not measure the proportion of Aboriginal and Torres Strait Islander peoples who were PICU inpatients during the study period. Even with that caution, the observed overrepresentation warrants attention. It is consistent with longstanding evidence that Aboriginal and Torres Strait Islander peoples experience a greater burden of mental illness, substance-related harms, involuntary treatment, and structural barriers to culturally safe care. For that reason, this finding is best understood not as an isolated prescribing issue, but as a signal of wider inequities in how acute mental health crises emerge, are responded to, and are managed within health systems. This finding highlights ongoing systemic inequities in mental health care access and delivery for Aboriginal and Torres Strait Islander Australians. 17
Importantly, the improvements in compliance, documentation, and monitoring following the intervention were consistent across all demographic groups, with only ECG monitoring showing statistically significant differences in treatment processes or outcomes between Aboriginal and Torres Strait Islander patients and other patients. This suggests that the intervention was effective and equitable in its implementation.
Nevertheless, the stark overrepresentation or Aboriginal and Torres Strait Islander peoples in acute psychiatric care underscores the need for culturally responsive care models, comprehensive psychosocial assessments, and strategies that foster cultural safety and patient-centred approaches. 18 Ongoing engagement with Indigenous health organisations and regular staff training in cultural competence are essential to address these disparities and ensure that care is both effective and culturally safe. 19
The literature also suggests that implementation of physical health monitoring in psychiatric settings is influenced by barriers that extend beyond the existence of a guideline. A systematic review by Ali et al. found that monitoring can be undermined by clinician knowledge gaps, uncertainty regarding responsibility for follow-up, time pressure, fragmented interfaces between mental health and general medical care, and difficulty engaging unwell patients in investigations. 20 Other quality improvement studies have shown that monitoring improves most when guidance is paired with practical workflow supports such as reminders, standardised documentation and multidisciplinary ownership, rather than dissemination of policy alone. 21 This helps explain why the present intervention, which combined a revised guideline with education and structured expectations, was associated with greater improvement than would be expected from passive guideline availability alone.
Several limitations should be considered when interpreting these findings. This project was conducted at a single PICU of a regional public teaching hospital, which may limit generalisability to other settings. The post-intervention sample size was relatively small, and data collection relied on retrospective medical record review, introducing potential documentation bias. An important comorbidity for people with acute behavioural disturbance is drug use, particularly methamphetamines, and this was not measured in the current study, but should be included in future work. Additionally, staff education and implementation fidelity were not formally audited. Despite these limitations, improvements were clinically meaningful and feasible.
Despite these limitations, the findings have practical implications. They support the use of audit-informed, locally adapted guideline revision as a feasible strategy to improve the safety of ZA use in psychiatric inpatient care. They also suggest that sustainability will likely depend on repeated audit cycles, feedback to prescribers and nursing staff, reinforcement of the full acute behavioural disturbance treatment pathway, and continued refinement of documentation and monitoring systems. As such, the project offers a pragmatic model for regional services seeking to strengthen psychotropic medication governance while aligning psychiatric care more closely with physical health safety standards. Based on the findings of this study, the following recommendations are proposed: (1) Balance efforts to improve monitoring and documentation for ZA with strategies to maintain guideline adherence for other medications, such as lorazepam and olanzapine, to ensure comprehensive and integrated care. (2) Address the persistent overrepresentation of Aboriginal and Torres Strait Islander patients in acute psychiatric care through ongoing collaboration with Indigenous health organisations, implementation of culturally responsive care models, and regular staff training in cultural competence. (3) Institute sustainability measures such as regular audits, real-time feedback, and continuous education to maintain improvements and address emerging gaps in practice. (4) Implement further auditing with a specific focus on addressing barriers to the implementation of the monitoring requirements. (5) Provide comprehensive training on the proposed ABDM guideline to medical and nursing staff, including the rationale for rigorous monitoring with ZA, and practical guidance on its administration and observation. (6) Promote a culture of empathy and reduce stigma through targeted education, reflective practice sessions, and support for staff well-being.
In summary, while the implementation of the proposed ABDM guideline has led to significant improvements in the safety and consistency of ZA prescription and monitoring, ongoing vigilance is required to ensure that all aspects of care, including cultural safety and comprehensive guideline adherence, are maintained and enhanced over time.
Conclusion
This study identified significant shortfalls in the clinical prescribing, administration and monitoring of ZA use within the pilot site PICU. Entrenching an evidence-based approach to clinical practice through an audit can affect clinically significant patterns of incremental change to improve safe prescribing and monitoring practice.
Footnotes
Ethical considerations
The study was approved by the Central Queensland Hospital and Health Service Human Research Ethics Committee (EX/2023/QCQ/91382).
Consent to participate
Informed consent was waivered within the ethics exemption and patient information deidentified.
Author contributions
S.R.: Study design, data collection, and writing the manuscript. V.K.S.: Study design, data collection, and writing the manuscript. M.H.: Data analysis and finalising the manuscript. A.R.: Study design, supervision, and finalising the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data is available from the corresponding author upon request.