
Abstract
Objectives
To summarise service models, facilitators and barriers relevant to recognising and treating attention deficit/hyperactivity disorder (ADHD) within adult public mental health services.
Methods
A scoping review following PRISMA-ScR guidelines examined international literature describing adult ADHD care delivered within public mental health systems. Data were charted on models of care, implementation facilitators and barriers, and evidence gaps were identified.
Results
Thirteen sources met inclusion criteria. The literature was limited and largely conceptual, consisting predominantly of editorials, commentaries and clinical guidance, with minimal empirical evaluation of implementation or outcomes. Three broad approaches to service delivery were described: embedding ADHD assessment and treatment within existing adult mental health teams; establishing specialist adult ADHD or neurodevelopmental services; and shared-care and primary-care–led models supported by specialist input. Facilitators included targeted workforce training and collaboration with primary care services. Barriers related to diagnostic complexity, clinician confidence, service capacity and concerns regarding prioritisation within public systems.
Conclusions
The literature consistently supports embedding ADHD care within routine adult public mental health teams, supported by targeted registrar and psychiatrist training and structured collaboration with general practitioners. Empirical evaluation of service models is needed to inform sustainable and equitable implementation within publicly funded mental health services.
Attention deficit/hyperactivity disorder (ADHD) is a neurodevelopmental condition characterised by persistent patterns of inattention and/or hyperactivity–impulsivity that frequently continue across the lifespan and are associated with substantial functional impairment. 1 Findings from the Multimodal Treatment Study of ADHD (MTA) longitudinal study highlight the variable course of ADHD from childhood to young adulthood. Approximately one-third of participants experienced periods of full remission; however, these were often temporary. Only 9.1% demonstrated sustained remission by the study endpoint (mean age 25 years). 2 Consistent with this, an umbrella review of global evidence reported that approximately 30–60% of individuals with ADHD in childhood continue to meet diagnostic criteria in adulthood and that predominantly inattentive presentations are the most common form of ADHD observed in adults. 3
ADHD frequently co-occurs with other psychiatric disorders, and a substantial proportion of adults receiving care in public mental health services are estimated to have underlying ADHD with prevalence estimates between 15% and 21%. 4 Despite this, routine identification and treatment within Australian public adult mental health services remain uncommon. Failure to recognise ADHD in these settings may contribute to misdiagnosis, suboptimal treatment and poorer outcomes. 5
In Australia, adult ADHD assessment and treatment have largely developed within the private sector. Australia’s mental health system is characterised by a division between public and private care. The public system provides essential acute, in-patient, and community-based services and is chronically stretched. The private sector, subsidised by the federal government, offers faster and more specialised treatment in areas such as ADHD, but primarily to those who can afford insurance or out-of-pocket fees, raising concerns about equitable access to care. 6 Consequently, private psychiatric care absorbs a substantial proportion of ADHD-related demand and plays a critical role in community care. Both the Royal Australian and New Zealand College of Psychiatrists and the 2023 Australian Government Senate Inquiry into services for people with ADHD have called for improved access to ADHD care within public mental health services, alongside enhanced workforce training.7,8 For most adult public mental health services, introducing ADHD care presents a substantial workforce and service redesign challenge.
This review aims to map available literature relevant to clinicians, clinical leaders and service planners seeking to integrate ADHD care into adult public mental health services, and to identify gaps in the literature.
Methods
This review followed Joanna Briggs Institute methodology and PRISMA-ScR reporting standards and the review protocol was registered on the Open Science Framework (OSF).9,10 The review was guided by the following research questions (RQ):
What models of care or service reforms are described to support the introduction of ADHD care into adult public mental health services?
What facilitators are reported to support implementation of ADHD care in adult public mental health settings?
What barriers are identified that may hinder implementation of ADHD care in these services?
Information sources and search strategy
A systematic literature search was undertaken in March 2025 in MEDLINE, PsycINFO, Embase, CINAHL and ProQuest Central. Search terms related to adult attention deficit/hyperactivity disorder (ADHD), public or government-funded mental health services, and models of care were used. No date limits were applied. A full breakdown of the search strategy and results is provided in Supplemental Material, Appendix 1.
Eligibility criteria
Sources were eligible for inclusion if they addressed identification, assessment, treatment or service models for adult ADHD within public mental health services. Given the emerging nature of the evidence base, editorials, commentaries, guidelines, descriptive studies and reviews were included to capture service-level and policy-relevant evidence. Records were excluded if they focused solely on children or adolescents, addressed only the clinical diagnosis or treatment of adult ADHD without reference to service models or public mental health systems, were not available in English, or were books or conference abstracts.
Selection of sources and data charting
Titles and abstracts of search results were independently screened by two reviewers. Full texts of potentially relevant sources were retrieved and independently assessed against the inclusion and exclusion criteria. Data were charted using a standardised extraction form and findings were synthesised narratively to inform service planning.
Results
Selection of sources of evidence
The database search identified a total of 1,616 records. After removal of duplicates and screening of titles and abstracts, 105 full-text records were assessed for eligibility, of which 13 were selected for inclusion. Characteristics of included records are provided in Supplemental Material, Appendix 2.
The study selection process is summarised in Figure 1. Included records mapped to the review questions as follows: six addressed models of care or service reform (RQ1), four described facilitators (RQ2) and three discussed barriers (RQ3). PRISMA flow diagram.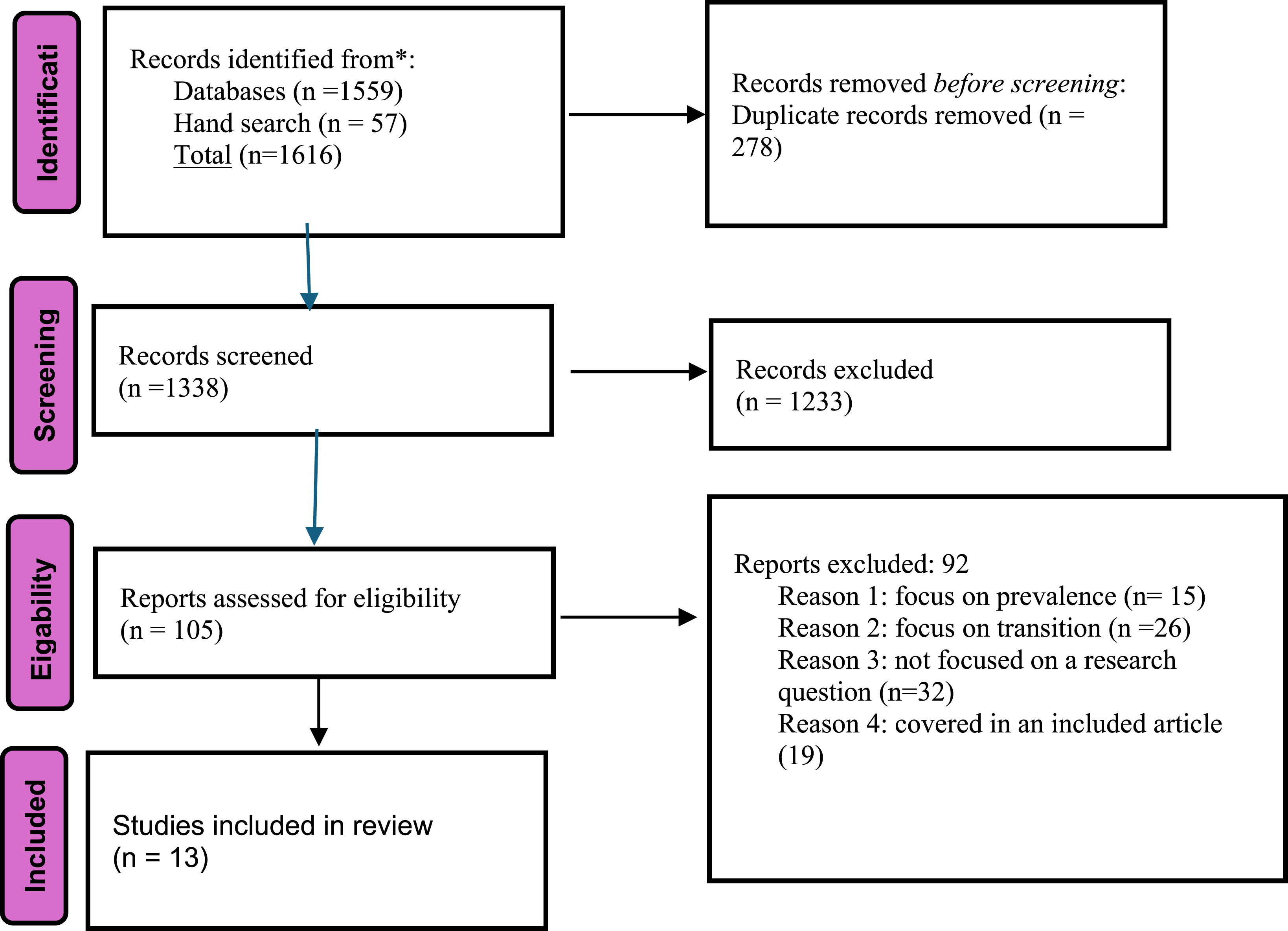
Models of care and service reform (RQ1)
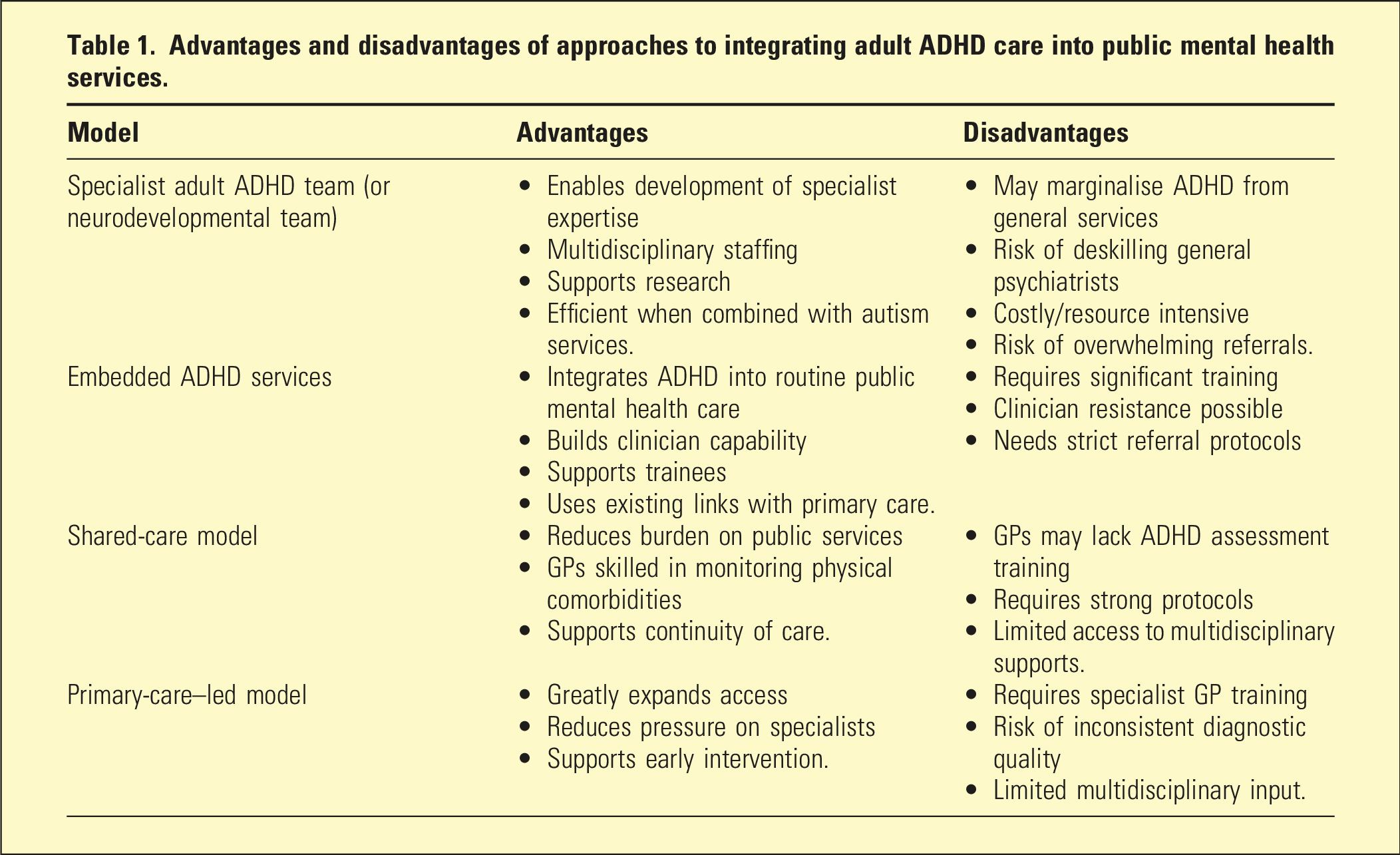
Three broad models of care were identified: embedding ADHD assessment and treatment within existing adult mental health teams, establishing specialist adult ADHD services and developing multidisciplinary neurodevelopmental teams that assess ADHD alongside autism spectrum disorder.11–14
Only one publication described ADHD care embedded within routine adult mental health practice with the remaining literature largely advocating for integration without reporting implementation processes or outcomes. 12
Establishing specialist adult ADHD teams was recommended in guidelines from the United Kingdom and Ireland.15,16 Importantly, in both countries these specialist ADHD teams are expected to accept direct referrals from general practitioners (GPs) and, in parallel, general adult teams are expected to embed ADHD assessment and treatment into routine care.
Advantages and disadvantages of approaches to integrating adult ADHD care into public mental health services.
Facilitators to implementation (RQ2)
Two key facilitators were identified: collaboration with primary care and the use of emerging technologies.
A spectrum of approaches to GP involvement in ADHD care and shared-care arrangements with GPs is described, ranging from GP-led follow-up following diagnosis by a psychiatrist to GP-led diagnosis and medication management following targeted training.12,17 Some evidence in Australian literature suggests that many GPs are willing and able to expand their role in ADHD management. 18 Emerging technologies, including digital assessment tools and remote monitoring, were discussed as potential supports for service expansion, although evidence for routine use in ADHD assessment and care remains limited.19,20
Barriers to implementation (RQ3)
Two recurring themes were identified: limited clinician training, including mixed clinician attitudes towards adult ADHD and diagnostic complexity, particularly related to comorbidity.
Several sources noted that adult ADHD assessment has not historically been a focus of psychiatric training, contributing to low clinician confidence. 21 Diagnostic complexity was highlighted across multiple records, particularly in distinguishing ADHD symptoms from comorbid mood, anxiety, substance use and personality disorders. 22 Attitudinal barriers included concerns regarding stimulant prescribing, workload implications and prioritisation within public services. 23
Discussion
This scoping review synthesises international guidance and emerging literature relevant to clinicians and service leaders considering how adult ADHD care might be incorporated into public mental health services rather than relying on the gradual diffusion of ADHD care through individual clinician initiative. The findings are directly relevant to clinical leaders responding to growing demand for adult ADHD care within public service systems. Experiences from the United Kingdom and Ireland are instructive for Australian service planning. In the UK, the Independent ADHD Taskforce concluded that public models reliant solely on specialist, single-diagnosis services, where diagnosis is restricted to psychiatrists or paediatricians, are unlikely to be sustainable. 24
Significant structural differences in service design between the United Kingdom, Ireland and Australia mean that the overseas models described cannot be directly transplanted into the Australian context.
Irrespective of the approach taken to introducing ADHD recognition and care into adult services, service leaders must consider established change management issues including risks, costs and stakeholder consultation. Given that clinical, educational and administrative resources are limited, implementation is likely to draw resource from other clinical programs unless there is parallel investment in workforce and infrastructure. 25
Implications for policy and service planning
Recent legislative reforms across multiple Australian jurisdictions, as well as in New Zealand, enable specially trained GPs to play an expanded role in ADHD diagnosis and treatment. These reforms signal a major shift in how ADHD care is likely to be delivered to the community.26,27 While New Zealand faces similar workforce and access challenges and recognises adult ADHD in public health pathways, differences in service organisation may require different implementation approaches.
Public mental health teams in Australia generally only accept individuals for treatment who present with acute symptoms or significant risk, including referrals from GPs. As a result, access is largely limited to patients with ADHD who have acute comorbid psychiatric illness or are in crisis, whether previously diagnosed or not. Currently, public services are only likely to prescribe ADHD psychopharmacological treatment for acutely ill patients following a confirmed diagnosis. In contrast, private psychiatric practitioners facilitate assessment in less acute contexts, including for individuals with subthreshold but functionally impairing symptoms, and may prescribe psychostimulant treatment. Reforms expanding the roles of GPs are likely to increase the number of adults with diagnosed ADHD presenting to public services. As GPs play an expanding role in ADHD diagnosis and management, there will be an increasing expectation that public services recognise ADHD and establish effective partnerships with primary care and private practitioners to support patients presenting with acute, complex comorbidity. 28
Workforce capability
Workforce capability emerges as a central theme in the literature. Diagnostic complexity and clinician attitudes towards adult ADHD require targeted training. Responsibility for building this capability rests with professional colleges, training bodies and public services themselves. Delays in embedding adult ADHD competencies within training curricula are inconsistent with professional position statements and emerging service demands. 7 Furthermore, where adult public services do not recognise or treat ADHD, trainees have little opportunity to gain clinical experience with this population.
Many psychiatrists working in public settings currently have had little or no training in identifying, diagnosing or treating ADHD. It is therefore understandable that some will be apprehensive about the prospect of upskilling. Resistance to service change is likely and should be recognised and addressed respectfully and with appropriate support. High-quality educational resources are increasingly available, including the Australian Evidence-based Clinical Practice Guidelines for ADHD and the ADHD Prescribing Guide produced by the Australian ADHD Professionals Association (AADPA).29,30 Engagement of experienced private-sector psychiatrists as external contractors to provide teaching and supervision may also support workforce development.
A possible model for Australian public services
Within the context described above, an internal-referral model, where specialist adult ADHD or neurodevelopmental teams accept referrals from within their parent service and co-manage care with general teams, may be both feasible and protect against the service pressures observed internationally. Such an approach mirrors the integration of specialist alcohol and other drug services within public mental health systems in Victoria, as recommended by the Royal Commission into Victoria’s Mental Health System. 31 This model could support the challenging task of embedding ADHD care within routine public service practice, provide essential training opportunities for psychiatry registrars and other clinicians and facilitate research, which is currently constrained by Australia’s reliance on private ADHD services.
Limitations
The relevant literature found in this review was limited in volume, with little empirical implementation or outcomes research, particularly within public-sector systems, and was largely drawn from the United Kingdom, Ireland and Australia. Consequently, conclusions regarding feasibility and impact must be interpreted cautiously.
Conclusion
This scoping review suggests that, despite increasing clinical and policy interest, the evidence base guiding the integration of adult ADHD care into public mental health services is limited. Nevertheless, the available literature offers practical direction for service leaders, professional colleges and educators responding to rising demand and is consistent with embedding ADHD care within routine adult public mental health teams.
Future research must move beyond descriptive accounts to evaluate the implementation, safety and outcomes of adult ADHD service models within public mental health systems. In particular, studies examining workforce capability, models of shared care with primary care and private practitioners and outcomes for individuals with complex comorbidity are needed to inform sustainable service development and support equitable access to care for adults with ADHD.
Supplemental material
Supplemental material - Recognising and treating ADHD in adults in public mental health services: key concepts: A scoping review
Supplemental material for Recognising and treating ADHD in adults in public mental health services: key concepts: A scoping review by Tom Callaly, Hatem Elshazly, Robert Lundin, Melissa Mulraney, Merryl Whyte and Scott Hall in Australasian Psychiatry
Footnotes
Ethical considerations
Ethics review was not sought or required for this study as it involved analysis of published literature and did not include human participants, identifiable data or unpublished patient information.
Author contributions
TC: conceptualisation; formal analysis; investigation; Methodology; writing – original draft; and project administration.
HE: conceptualisation, investigation; methodology; and writing – review and editing.
RL: supervision, investigation; methodology; and writing – review and editing.
MM: supervision, investigation; methodology; and writing – review and editing.
MW: Writing – methodology and review and editing.
SH: Writing – methodology and review and editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analysed during this study are included in this published article and its supplementary materials.
Supplemental material
Supplemental material is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.