
Abstract
Objective
To descriptively analyse aeromedical retrievals of children and adolescents for mental health concerns to Royal Darwin Hospital from February 1, 2016, to February 1, 2024.
Method
A retrospective review of electronic medical records was conducted of children and adolescents under 18 years who were transported via aeromedical retrieval to Royal Darwin Hospital for mental health concerns. Data were collected on demographics, clinical characteristics, admission status, length of stay, discharge destination, and representation rates, which were analysed descriptively.
Results
A total of 226 retrievals involving 167 patients were identified. Most patients (89%) were Indigenous, with an average age of 15 years. Common reasons for referral included psychotic symptoms (41%) and suicidal behaviour (25%). Most referrals came from primary community health clinics (73%). The majority of admissions were involuntary (83%), with an average length of stay of 12 days. Approximately one-third of retrieval episodes resulted in discharge to the Darwin metropolitan area.
Conclusion
Aeromedical retrieval plays a central role in facilitating access to specialist child adolescent mental health care, particularly for Indigenous adolescents in remote communities.
Keywords
A nationwide survey of child adolescent mental health in Australia found that approximately one in seven Australian’s aged 4–17 years experienced mental illness in a 12-month period, with anxiety, depression, attention deficit hyperactivity disorder, and conduct disorder being the most frequent disorders. 1 However, less is known about mental health presentations of children and adolescents in the Northern Territory (NT) compared to the broader Australian context. NT-specific research has found that hospitalisation trends for suicidal behaviour, particularly among Indigenous youth are increasing in the NT. 2 Additionally, psychiatric emergency presentations among individuals aged 15–18 in the NT have increased over time. 3
Aeromedical retrieval is defined as the transport of patients via fixed-wing aircraft or helicopter for medical care and plays an important role in enabling access to tertiary hospital services, including for individuals with mental health concerns.4,5 In remote regions of the NT, vast distances and limited local healthcare resources mean that aeromedical retrieval often represents the only viable pathway to tertiary care. 6 Children and adolescents in these settings may be first assessed in primary community health clinics, which do not routinely have access to specialist child and adolescent psychiatric services.
Royal Darwin Hospital (RDH) is the NT’s tertiary referral hospital and the only hospital with a specialised child adolescent inpatient mental health unit. 7 RDH provides specialised inpatient and outpatient mental health care for children and adolescents living in the northern regions of the NT, including Darwin, Palmerston, East Arnhem and Katherine region. Specialist inpatient and outpatient services are delivered through the Top End Mental Health Service; however, there is no dedicated outreach child adolescent service. Consequently, children and adolescents requiring specialist psychiatric assessment or inpatient treatment are transferred to RDH via aeromedical retrieval.
While existing studies have explored aeromedical retrievals nationally,4,8–15 literature specifically examining aeromedical retrievals for mental health concerns in the NT, has for the most part, been limited to the Central Australia and Barkly districts of the NT – areas served by the Royal Flying Doctor Service (RFDS) – which contains only one fifth of the NT population.10,11,14 The RFDS coordinates only a small number of aeromedical retrievals to RDH, with the majority operated by CareFlight. As a result, existing studies on aeromedical retrievals for mental health concerns in Australia have not adequately represented the population served by TEMHS; even the sole study addressing youth 14 relied on RFDS data, which does not comprehensively cover this region.
This study addresses this gap by examining, for the first time, the characteristics of aeromedical retrievals for children and adolescents with mental health concerns to RDH. This research will provide valuable insights into the nature and extent of psychiatric emergencies affecting young people in the northern regions of the NT, which can inform the development of clinical services.
Aim
This retrospective descriptive study aimed to analyse clinical data from children and adolescents transported to Royal Darwin Hospital for mental health concerns via aeromedical retrieval over the period from February 1, 2016, to February 1, 2024. The objectives included quantifying the incidence and trends of aeromedical retrievals for mental health concerns, specifically the demographic characteristics of the patient population, and assessing clinical characteristics and short-term outcomes.
Methodology
Study design
A retrospective review of electronic medical records at RDH was conducted for children and adolescents under 18 who were transferred via aeromedical retrieval for mental health concerns between February 1, 2016, and February 1, 2024. Retrievals outside this period or from outside the Top End Mental Health Service catchment were excluded. Only retrievals that resulted in an admission to the child adolescent mental health inpatient unit were included. All identifying information was removed for confidentiality.
Data were collected on demographics, clinical characteristics, admission status, length of stay, discharge destination and representation rates, using primary sources such as the referral assessment, emergency triage documentation, and admission and discharge summaries. The primary presenting concern was defined as the reason for retrieval documented by the referring clinician. Arrival time analyses were limited to retrieval episodes that presented via the emergency department, where a recorded triage time was available.
Aeromedical retrieval notes were excluded from analysis due to inconsistent availability in the electronic records. Discharge diagnoses were not systematically analysed, as many were recorded using non-specific terms such as ‘situational crisis’, and therefore formal mental health diagnoses were not reliably available.
Analysis
Descriptive analyses of demographic, clinical variables, and episode characteristics were conducted using Microsoft Excel. For the demographic and clinical data analysis, only the first episode per individual was included, while for referral and outcome analysis all episodes were examined.
Ethics
Ethical approval was obtained from the Human Research Ethics Committee of NT Health and Menzies School of Health Research (reference number 2024-4862). This study used routinely collected clinical data and was reviewed in accordance with ethical guidelines for research involving Aboriginal and Torres Strait Islander peoples.
Results
Demographic characteristics
During the study period, 226 aeromedical retrievals involved 167 individual patients. Of these, 89 (53%) were female, and 149 (89%) were Indigenous. The mean age was 15 years (standard deviation = 1.4), with a range of 10–17 years.
Regarding living arrangements, 92 patients (55%) lived with parents, 60 (36%) lived with other family members, and 15 (9%) lived in a non-family residence (e.g. foster care, supported accommodation, or with a romantic partner). Additionally, 16 patients (10%) were under the care of child protection services. Educational status was recorded for 137 patients, with 63 (38%) attending school.
Demographic variables.
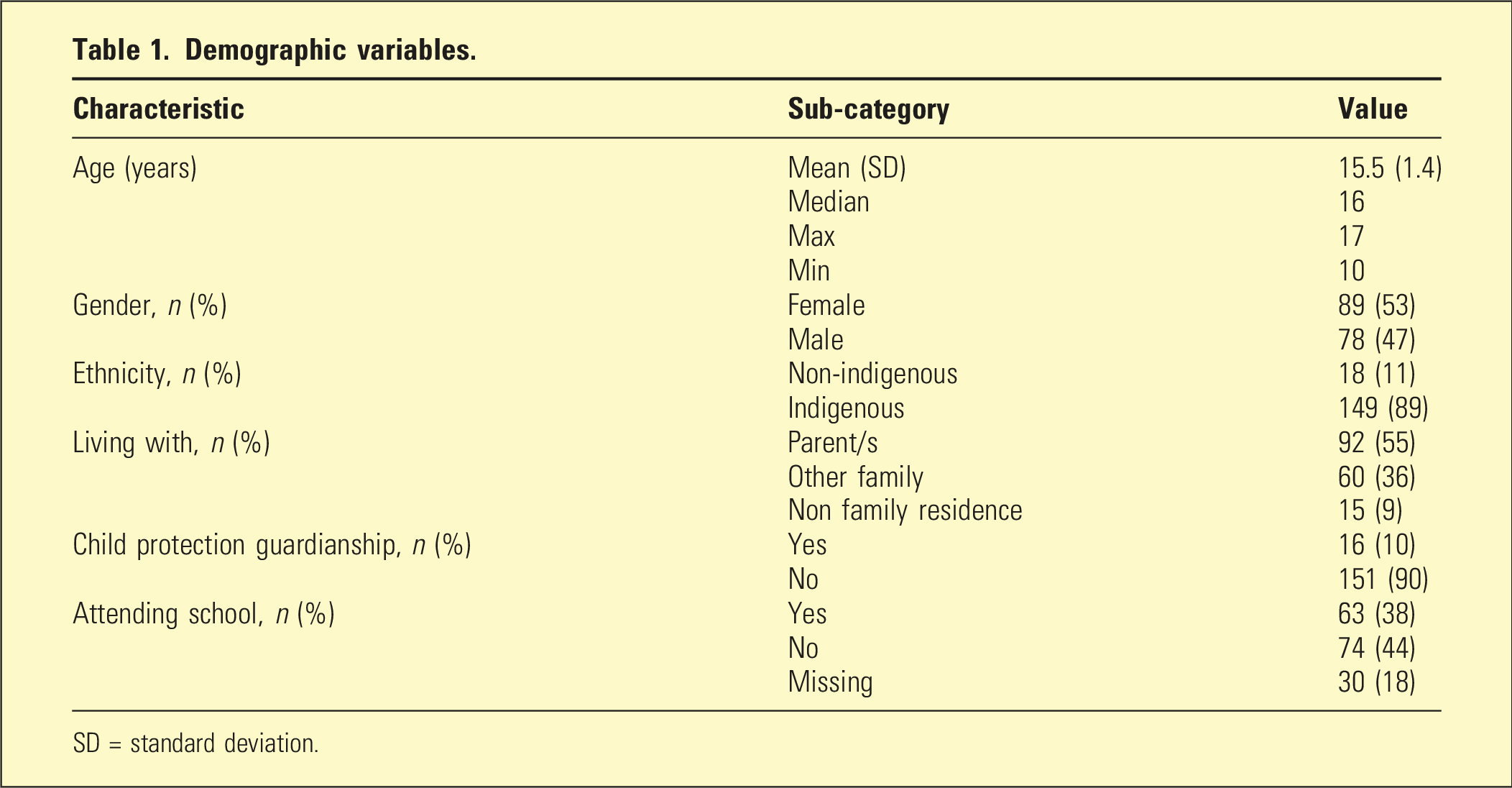
SD = standard deviation.
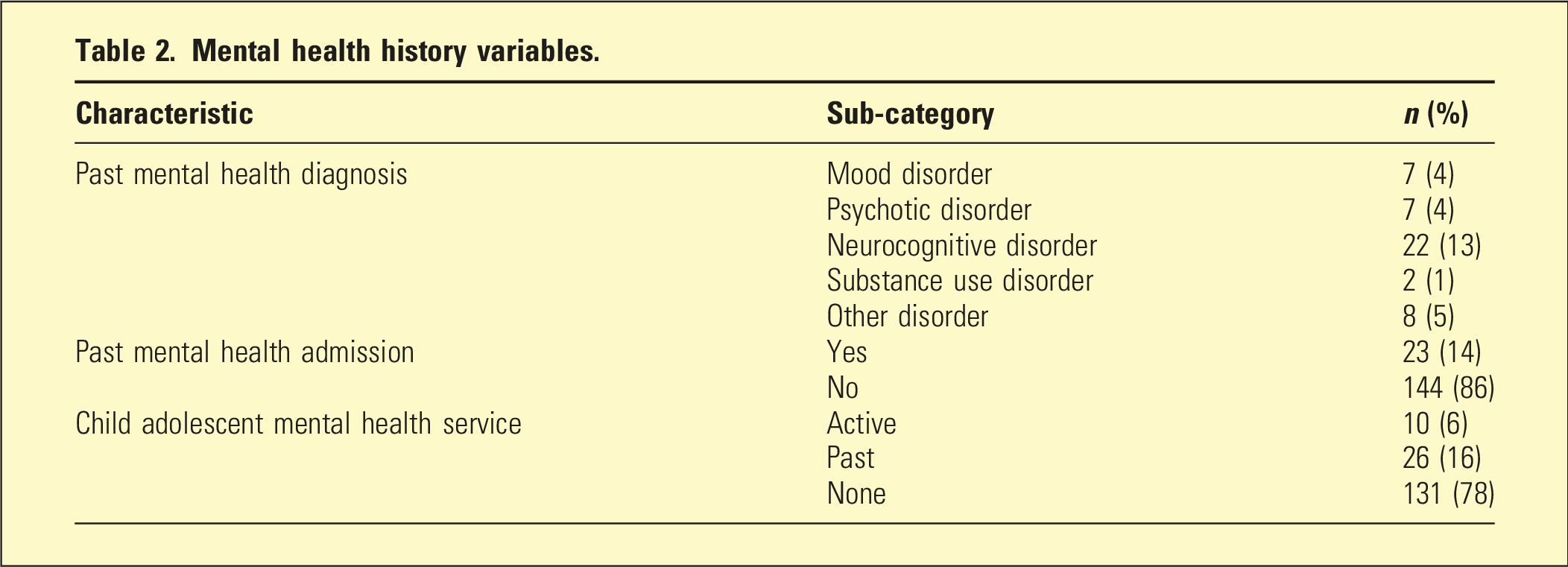
Mental health history variables.
Retrieval characteristics and discharge disposition
The following data were obtained from 226 retrieval episodes.
Referral characteristics
Most referrals for aeromedical retrieval request came from primary community health clinics (73%), with the remainder coming from district hospital sites. In terms of regionality, 76 referrals (34%) were from the Katherine region, 70 referrals (31%) from the East Arnhem region and 80 referrals (35%) from the Darwin region (excluding Darwin and Palmerston metropolitan areas).
Figure 1 summarises the primary presenting concerns leading to retrieval. These were suicidal behaviour (56 episodes, 25%), suicidal ideation (51 episodes, 23%), psychotic symptoms (93 episodes, 41%), deliberate self-harm (6 episodes, 3%), and behavioural reasons (20 episodes, 9%). No cases were documented as retrieved for mood symptoms or other mental health reasons as the primary concern. Characteristics of reasons for aeromedical retrieval.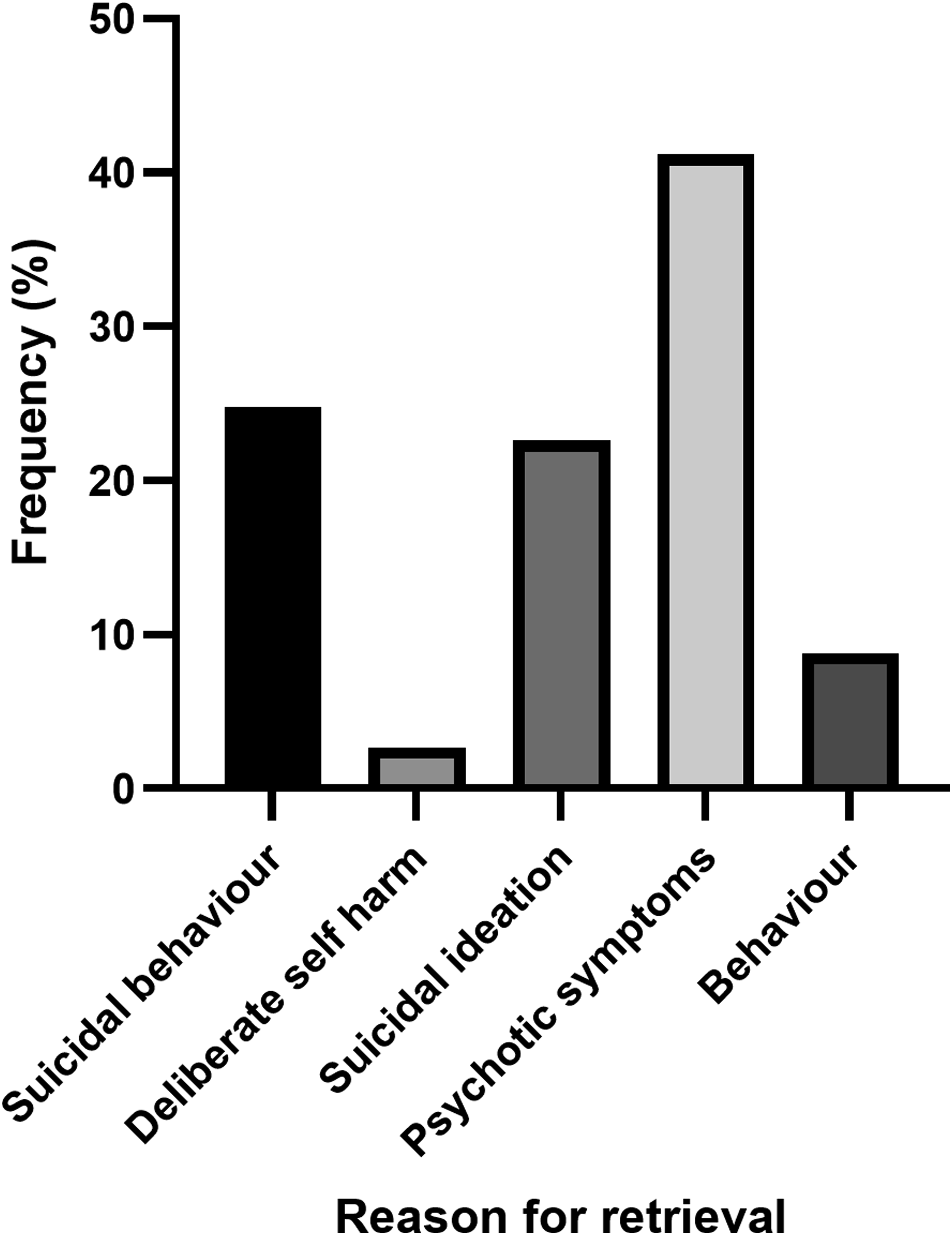
Aeromedical retrieval arrivals were most frequent on Friday (43 episodes, 19%), followed by Tuesday (39 episodes, 17%), Wednesday (39 episodes, 17%), Thursday (38 episodes, 17%), Monday (28 episodes, 12%), Saturday (25 episodes, 11%) and Sunday (14 episodes, 6%).
The most aeromedical retrievals occurred between February 1, 2022, and February 1, 2023, and the least occurred between February 1, 2016, and February 1, 2017. Trends in number of aeromedical retrievals by year of arrival is demonstrated in Figure 2. Number of aeromedical retrievals according to date of arrival.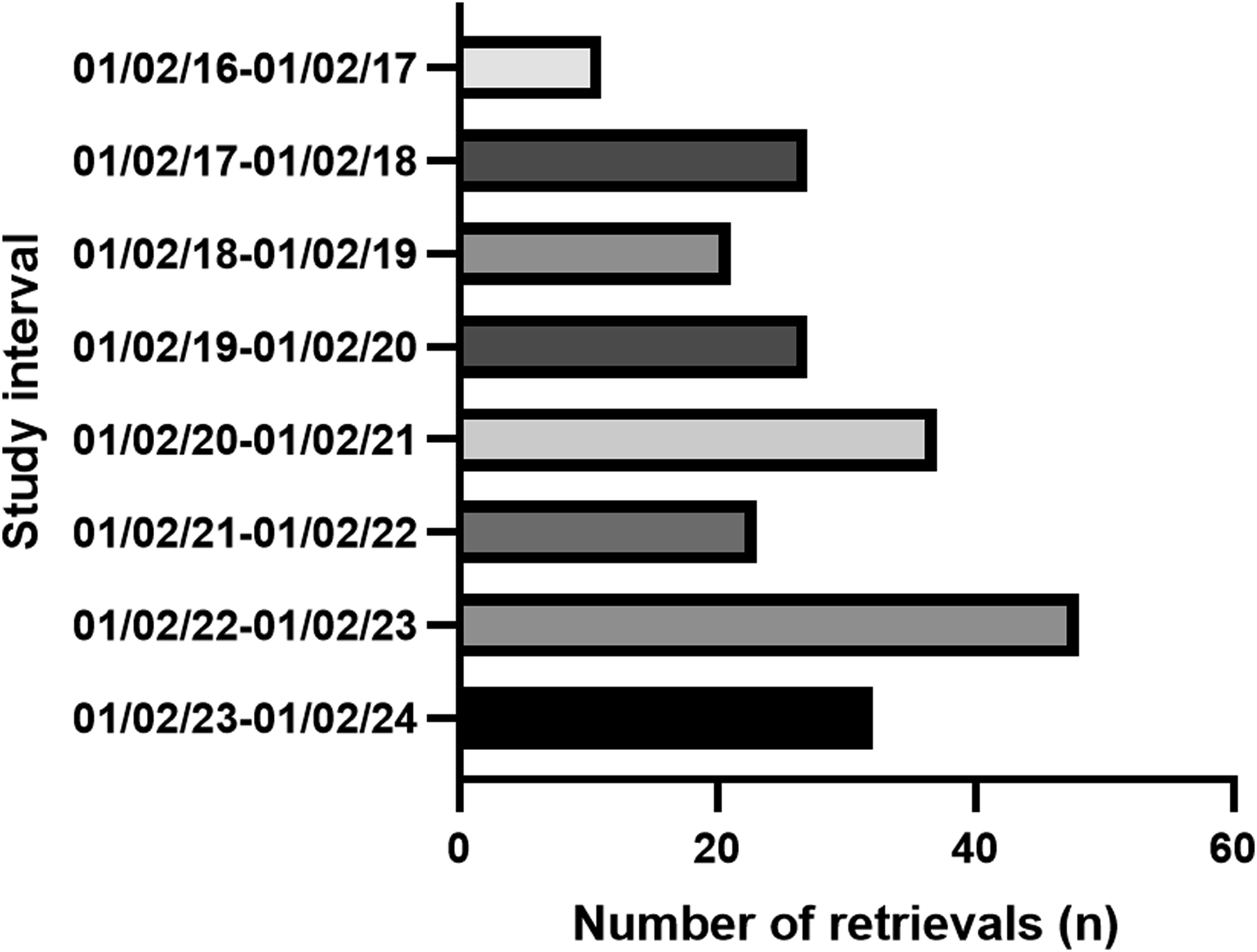
Most presentations were admitted to the hospital ward via the emergency department. However, eight were admitted directly to the inpatient psychiatry ward without triage through the emergency department and one episode did not have an accessible emergency triage document. These episodes were removed from analysis when determining arrival times, leaving a total of 217 episodes. Figure 3 shows that most episodes presented outside of business hours. 67 (31%) episodes occurred between 8:00 and 16:29 hours, 90 (41%) episodes occurred between 16:30 and 11:59 hours, and 60 (28%) presented to hospital between midnight and 7:59 hours. Aeromedical arrival according to time of day.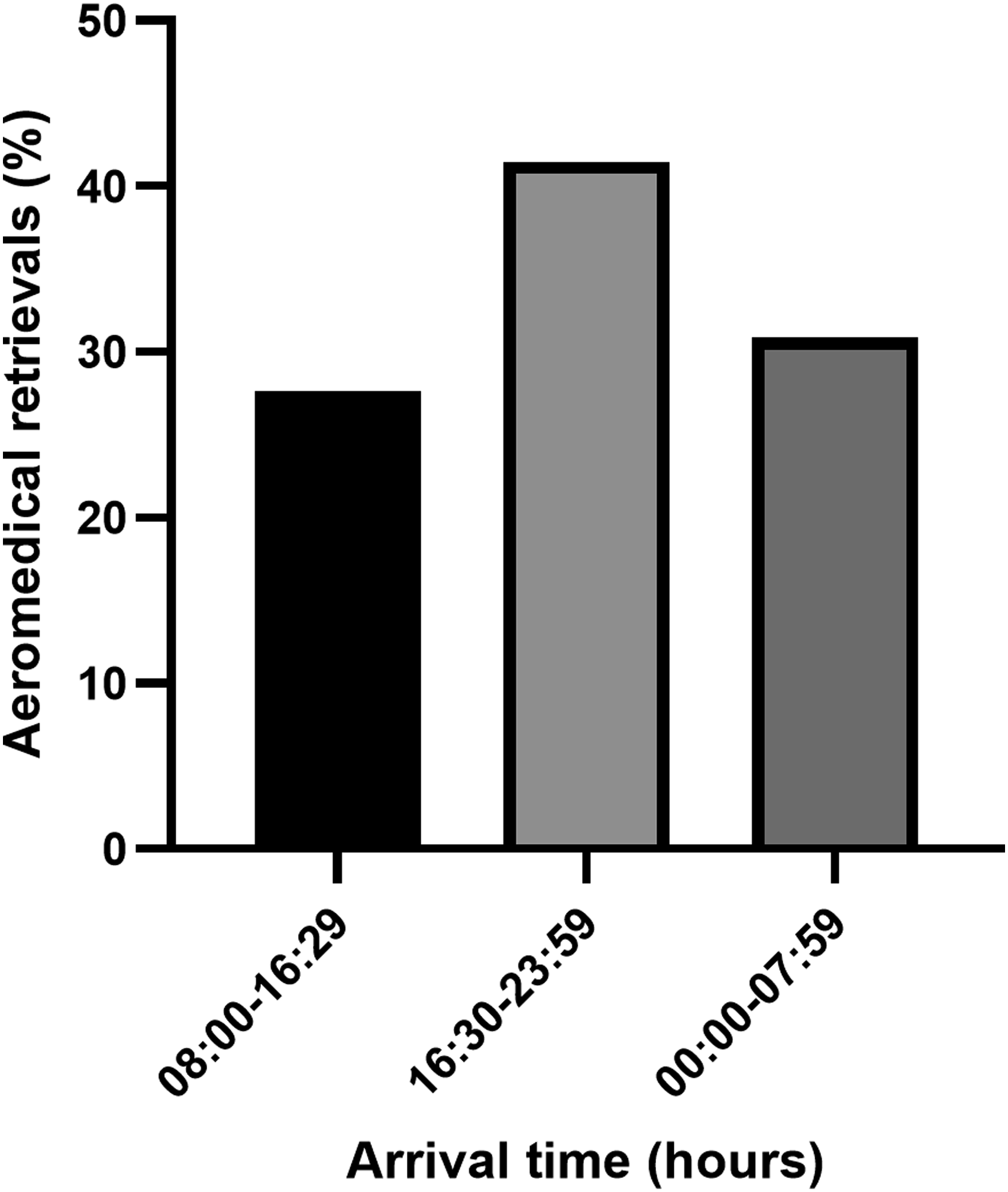
Admission characteristics
The average length of admission was 12 days, with a median length of stay of 8 days; the longest recorded stay was 84 days, while the shortest was 1 day. Of the admissions, 187 (83%) episodes were involuntary, whilst 39 (17%) were voluntary under the NT Mental Health Act.
220 (97%) episodes were admitted to the child adolescent mental health inpatient unit, while two were admitted to the intensive care unit, and four were admitted to another ward (extended emergency, paediatric or surgical wards) prior to admission to the mental health unit.
Discharge disposition
Forty (18%) episodes were discharged to the Darwin metropolitan area, 147 (65%) to remote regions, 33 (15%) to temporary accommodation in the Darwin metropolitan area. 6 (3%) episodes ended as the patient absconded, discharged against medical advice, or was discharged from psychiatry and transferred to another hospital team.
Representation rates
Throughout the study period, 33 patients represented via aeromedical retrieval and were admitted to psychiatry, with the maximum number of representations being 6, a median of 2, and an average of 2.8 representations per individual.
Discussion
This study is the first to examine aeromedical retrieval of children and adolescents with mental health concerns to RDH. The findings demonstrate that retrievals predominantly involved older adolescents, many of whom were Indigenous, with referrals commonly originating from primary community health clinics. The most frequent reasons for retrieval were psychotic symptoms and suicidal behaviour, and most admissions occurred as involuntary under the NT Mental Health Act.
A key finding was that for most patients, the aeromedical retrieval was their first recorded encounter with specialist mental health services. This likely reflects the limited availability of local child adolescent mental health care in remote regions of the NT, where specialist services are primarily based in Darwin and not routinely available within remote regions. The urgent nature of retrievals, and the associated separation from family and community, means that initial engagement with specialist care often occurs in conditions that differ substantially from those available within community settings.
In many cases, retrievals resulted in arrival outside standard business hours. In this context, specialist child and adolescent psychiatrists are not routinely available on site. As a result, some children and adolescents experienced delays before specialist psychiatry assessment, which were most pronounced when arrival occurred over the weekend.
This study also found that a high proportion of admissions were involuntary, likely reflecting the severity, and complexity of presentations necessitating aeromedical retrieval. While involuntary admission rates reported elsewhere in Australia appear lower,16,17 direct comparison is limited by such factors as differences in study design, population demographics, and mental health legislation. Future research could examine use of involuntary provisions under the mental health act among children and adolescents in the NT.
A subset of patients in this study experienced multiple aeromedical retrievals, suggesting they experienced persisting or recurrent mental health problems. While the reasons for repeated retrieval were not examined in this study, the data may imply challenges associated with continuity of care following discharge from hospital. Similarly, the finding that nearly a third of retrieval episodes resulted in discharge to the Darwin metropolitan area rather than return to the site where retrieval was initiated warrants further exploration. Although this may reflect individual preferences or logistical challenges, it could also be indicative of broader service-related barriers that contribute to extended stays in metropolitan areas.
While prior studies have reported an increase in aeromedical retrievals over time, 4 the COVID-19 pandemic may have influenced the trends observed in this study. The decrease in retrieval rates in this study observed from February 2021 to February 2022 may reflect pandemic-related isolation measures in the region. Further research is needed to clarify trends in retrievals over time.
The findings of this study point to the need for several system improvements. First, clinical staff in remote communities should receive additional training and resources to assess and manage mental health issues in children and adolescents. Additionally, clinics should have access to specialised child and adolescent mental health expertise through outreach visits or telehealth to ensure timely care. This would align with recovery-oriented principles and the NT Mental Health Strategic Plan.7,18
Several limitations must be acknowledged. First, the retrospective chart review design relied on the accuracy and completeness of existing medical records, which may introduce bias if critical information is missing or inconsistently documented. Additionally, aeromedical retrieval clinical notes were not consistently availability within the electronic medical records, limiting description of in-transit variables such as clinical risk and sedation use. Reasons for retrieval were based on referring clinicians’ assessment notes, reflecting the presenting concern at the time; discharge diagnoses from specialist services were not included, which may limit direct comparison with confirmed diagnostic outcomes. The study’s geographical and temporal focus limits the generalisability of the findings to other regions or populations. Finally, whilst it is standard practice at RDH that aeromedical retrievals with mental health concerns do get admitted to an inpatient psychiatric unit, the exclusion of cases that did not result in psychiatric admission may have skewed the data toward more severe presentations.
Conclusion
This study provides insight into the aeromedical retrieval process for children and adolescents with mental health concerns to RDH. The findings emphasise the need for improved access to mental health care in remote settings, alongside enhanced specialist support through outreach or telehealth models. Strengthening community-based services may reduce need for emergency mental health retrievals and improve continuity of care for children and adolescents in the region.
Footnotes
Author’s
The authors declare that they were employed by the psychiatry service at the tertiary hospital where the data for this retrospective audit was collected. While the authors’ employment at the institution does not constitute a conflict of interest in the retrospective nature of the study, the potential for bias in data analysis is acknowledged.
Acknowledgements
We would like to acknowledge the administrative staff at Royal Darwin Hospital for their support in facilitating this research, and to the Human Research Ethics Committee of NT Health and Menzies School of Health Research for their approval of the study.
Ethical considerations
Ethical approval was obtained from the Human Research Ethics Committee of Northern Territory Health and Menzies School of Health Research (reference number 2024-4862) on April 2024.
Consent to participate
The Human Research Ethics Committee of Northern Territory Health and Menzies School of Health Research (reference number 2024-4862) provided a waiver of patient consent for the collection, analysis and publication of the retrospectively obtained and anonymised data for this non-interventional study.
Author contributions
Dr Natalie Hunt conceived and designed the study, with the assistance of Professor Philip Hazell. Dr Hunt conducted data analysis and drafted the manuscript. Professor Hazell reviewed the paper prior to submission.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data from this study are available from the corresponding author upon reasonable request. Access to the data is limited to researchers conducting meta-analysis, to minimise the risk of patient identification and to protect the confidentiality of the participants. Due to privacy and confidentiality restrictions, the data are not publicly available.