
Abstract
Objective
The Hirsch-index (H-index) is a bibliometric measure of research productivity and citation impact. In this systematic review and meta-analysis we aimed to derive pooled H-index benchmarks across professorial academic ranks in psychiatry, and to determine whether H-index differs significantly between successive academic ranks.
Methods
PRISMA guidelines were followed in conducting a comprehensive search using the databases Ovid MEDLINE, PubMed, EMBASE, and Google Scholar. Key search terms included: “Bibliometrics”, H index”, “H-index”, “Career Mobility”, “academic rank”, “Faculty, Medical”, “psychiatry”, “academic psychiatry”, “psychiatric”, and “Psychiatry in Literature”. Papers reporting data on mean H-index stratified by professorial academic rank were included. The DerSimonian and Laird random effects model was used to conduct the meta-analysis.
Results
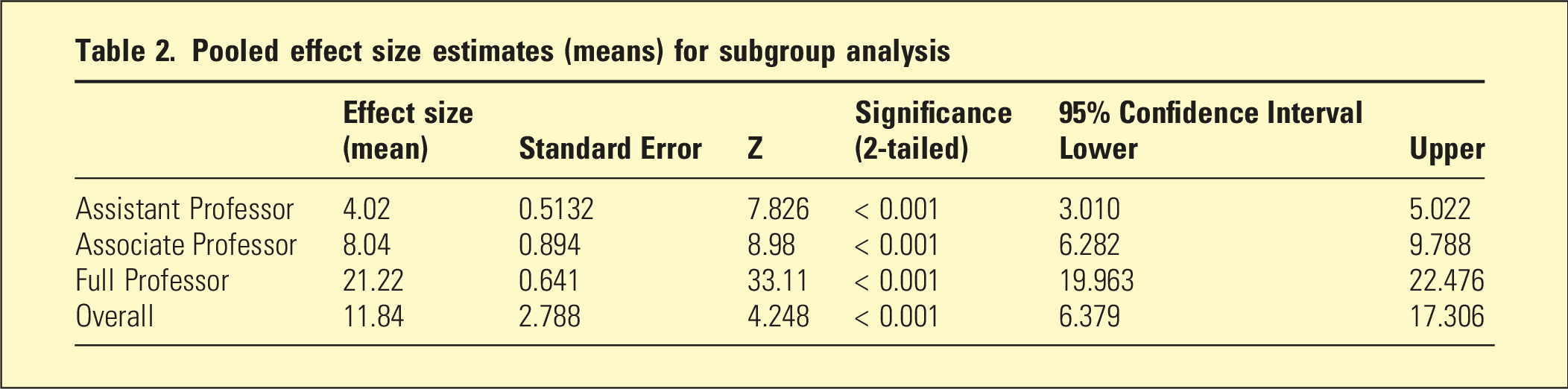
Four studies (all North American) were included in the systematic review and three in the meta-analysis. Mean H-index increased across successive academic rank. Pooled random effects estimates for mean H-index were: 4.02 (95% CI: 3.01–5.02) for Assistant Professor, 8.04 (95% CI: 6.28–9.79) for Associate Professor, and 21.22 (95% CI: 19.96–22.48) for Full Professor.
Conclusion
H-index increases with successive academic rank in psychiatry, with pooled benchmarks identified for each professorial level. Available data are limited to North American institutions, underscoring the need for Australasian studies.
“It does not matter how slowly you go as long as you do not stop.” ― Confucius
In academic medicine, including psychiatry, faculty members are assessed on their research productivity for the purposes of employment, promotion, grant allocation, recognition, and award decisions. 1 A variety of bibliometric indicators have been developed to quantify scholarly productivity. 2 Traditional metrics, such as total publication counts or total citation numbers, capture certain dimensions of output but fail to balance productivity, quality, and long-term impact. In 2005, J.E. Hirsch proposed the “H-index”, which has since become one of the most widely adopted bibliometrics across academic disciplines. 3 The H-index represents both productivity and influence by identifying the number of papers (H) an author has published that have each been cited at least H times. A researcher with an H-index of 25 has at least 25 publications that have each received 25 or more citations. This measure is therefore more reflective of sustained scholarly contribution than publication counts or journal impact factor alone.
Bibliometrics have become increasingly important in academic medicine, where promotion and tenure committees often include reviewers outside a candidate’s specific field. 4 Evidence-based measures such as the H-index provide committees with a relatively objective benchmark when comparing productivity across individuals and institutions. 1 Numerous medical and surgical specialties, including paediatrics, anaesthetics, orthopaedic surgery, general surgery, plastic surgery, dermatology, otolaryngology, ophthalmology, sports medicine, psychiatry, radiology, urology, radiation oncology, and surgical oncology, have consistently demonstrated a positive association between H-index and academic rank in prior studies. 1
In psychiatry, as in other specialties, scholarly productivity is only one component of faculty evaluation, which may also consider excellence in clinical care, education, mentorship, leadership, and professional and community service. Some academic appointments may even be oriented towards teaching activities. Nevertheless, because research output often carries significant weight in promotion and tenure decisions, bibliometrics such as the H-index have assumed a central role. Establishing discipline-specific benchmarks may therefore assist in promoting greater transparency and equity in academic career progression within psychiatry. In many institutions, success in competitive research funding is also a key criterion for academic promotion, further underscoring the multidimensional nature of academic evaluation.
A systematic review and meta-analysis of productivity (focussing on H-index) and academic rank in multiple medical and surgical disciplines was published by Zaorsky et al. in 2020.
1
However, this review included only one paper relating to psychiatry, published in 2017 and focussing on Canadian data.
5
Therefore, an update for academic psychiatry is warranted. Our systematic review and meta-analysis sought to address the following questions: (1) What are the pooled mean H-index benchmarks for each professorial academic rank (Assistant Professor, Associate Professor, and Full Professor) within the discipline of psychiatry, based on all currently available data? (2) Are there statistically significant differences in H-index between successive professorial academic ranks in the faculty of psychiatry?
Methods
Protocol and registration
We registered our systematic review and meta-analysis with PROSPERO (https://www.crd.york.ac.uk/prospero/) on 21 August 2025 (CRD42023488235).
Databases and search strategy
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines were followed in performing our systematic review (Figure 1). A comprehensive search was conducted using the databases Ovid MEDLINE, PubMed, EMBASE, and Google Scholar. PRISMA flow diagram.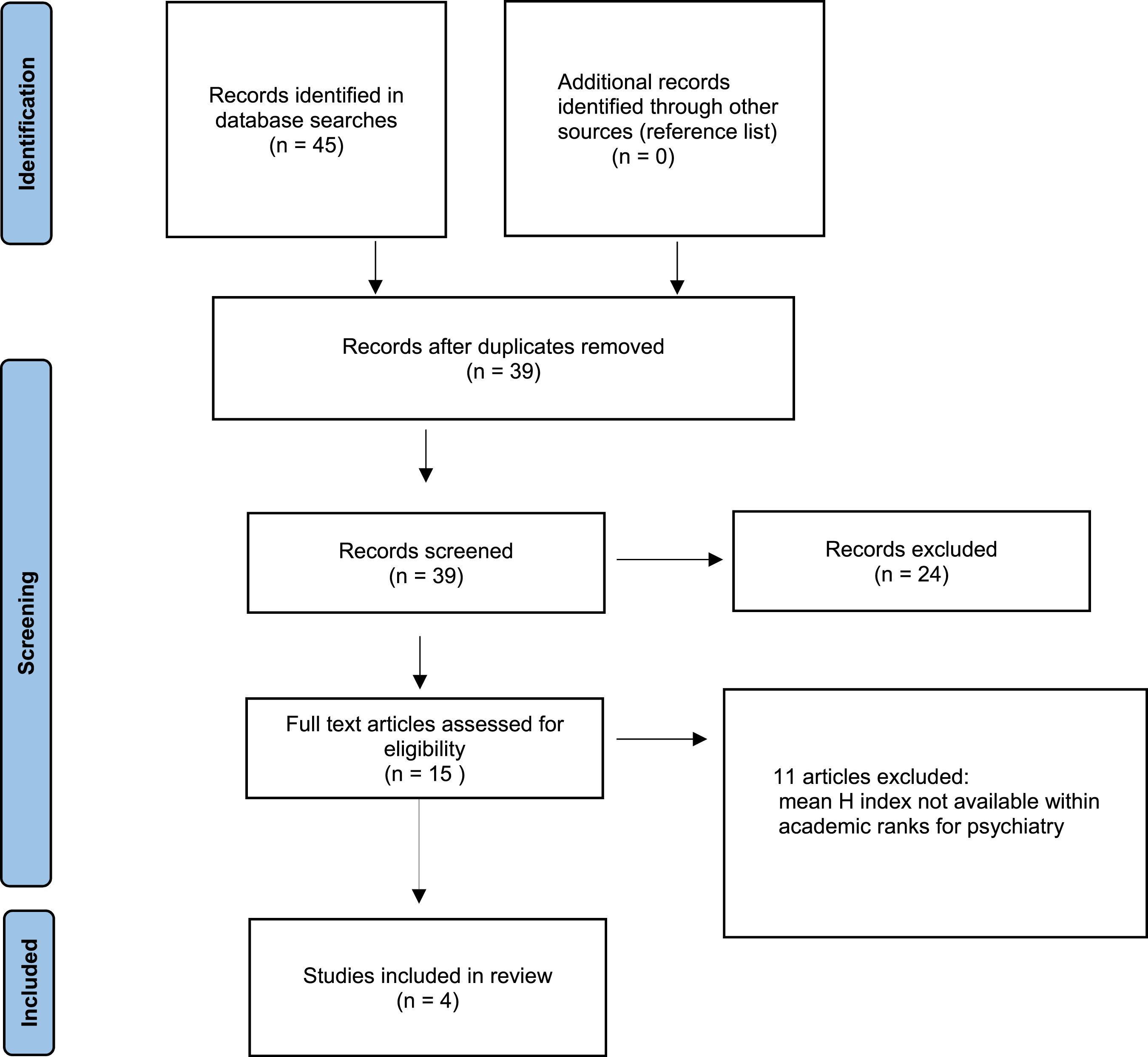
For Ovid MEDLINE and EMBASE the search strategy consisted of: (1) exp *Bibliometrics/or h index. mp, (2) exp Career Mobility/or exp *Faculty, Medical/or academic rank. mp, (3) Psychiatry. mp or exp *Psychiatry/or exp *Psychiatry in Literature/, (4) 1 and 2 and 3. For PubMed search terms included: (h index OR h-index) AND (academic rank) AND (psychiatry OR academic psychiatry OR psychiatric). For Google Scholar search terms were: allintitle: h index OR h-index psychiatry OR psychiatric.
We limited our search to English language papers published over the past twenty years.
Eligibility criteria
We included papers which provided data on mean H-index for the academic ranks of Assistant Professor, Associate Professor, and Full Professor within the discipline of psychiatry.
Study selection
The titles and abstracts, and when required, the body, of the papers from the search were reviewed independently by two authors to determine whether or not they met the eligibility criteria. Disagreements were resolved by consensus, including, if necessary, a third author.
Data extraction
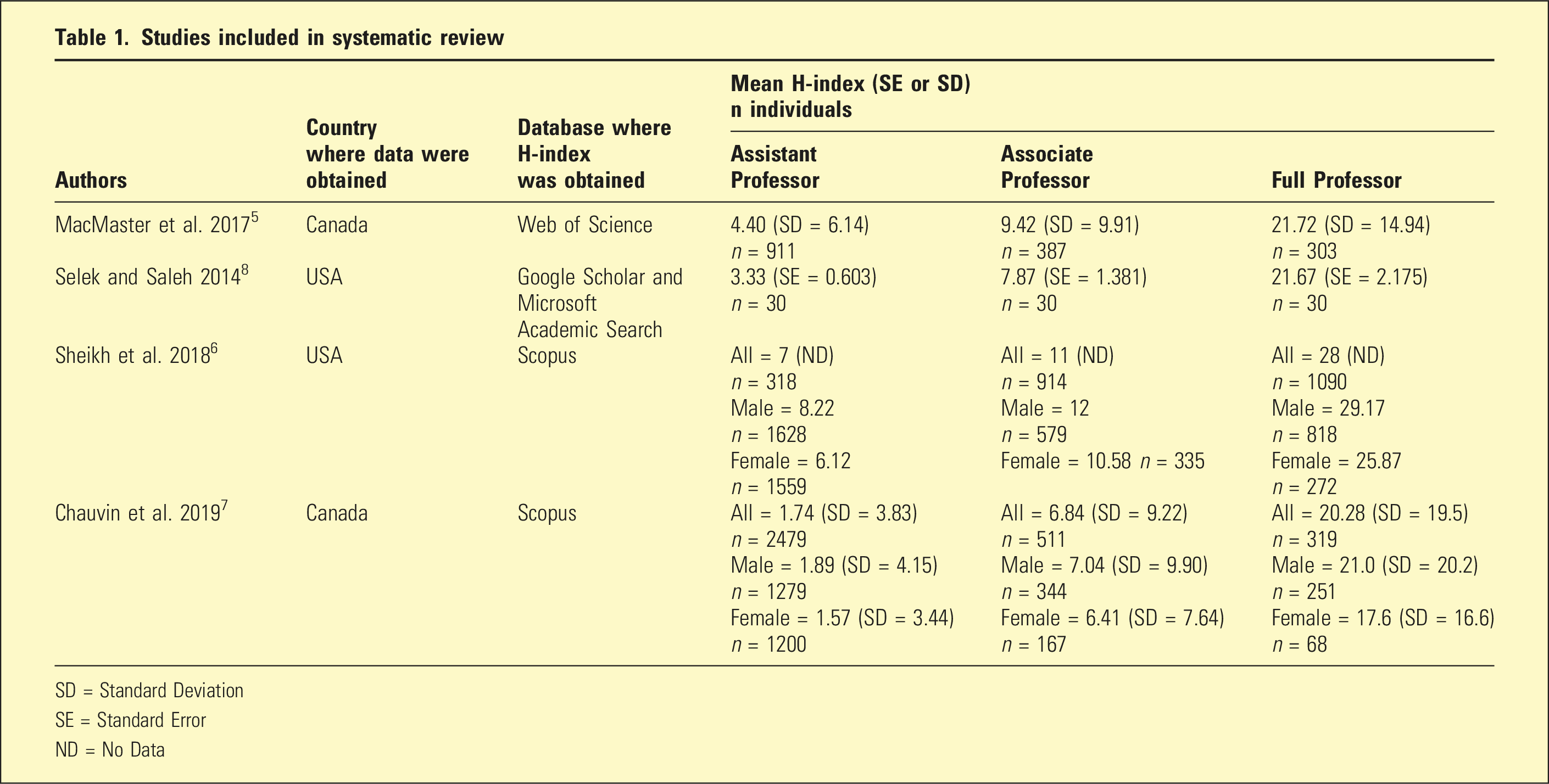
Relevant study data were extracted from identified papers by one author and confirmed by a second author. This information included: author(s), year, country where data were obtained, database used to obtain H-index, sample size (including stratified sample sizes), and mean H-index within each professorial academic rank with standard deviations or standard errors. One study 6 did not report standard deviations and/or standard errors for the mean H-indices. Attempts to contact the authors to obtain the missing data were unsuccessful. Therefore, this study was included in the systematic review but not in the meta-analysis, as these data are required to ensure appropriate weighting of the pooled effect size estimates.
Statistical analysis
Data were analysed using IBM SPSS Statistics version 30.0.0.0 (172) and JASP (version 0.95). Meta-analyses were conducted on the differences in the mean H-index between successive professorial academic ranks. The DerSimonian and Laird method (random effects model) was used to perform meta-analyses. Heterogeneity, overall and for each rank, was assessed using I2. Homogeneity, overall and between ranks, was assessed using the Q statistic. A Forest plot was generated for the pooled effect sizes (means) with academic rank subgroup analysis.
Results
As demonstrated in the PRISMA flowchart (Figure 1) six duplicates were removed, and 24 articles were excluded following title/abstract screening, as they did not meet the eligibility criteria. This resulted in four studies which were included in our systematic review.5–8
Study characteristics
Studies included in systematic review
SD = Standard Deviation
SE = Standard Error
ND = No Data
Collectively, the four studies comprised a total of 10,191 academics. In one study the academic rank of Assistant Professor also included Lecturers, whose academic roles are typically weighted towards teaching and tend to be less research-intensive than professorial appointments. 7 Accordingly, the mean H-index reported for this academic stratum was not included in the meta-analysis as its inclusion was considered likely to spuriously lower the pooled effect size estimates for Assistant Professors.
Across all included studies, there was a consistent increase in mean H-index with successive academic rank. Two studies reported H-index data stratified by gender, with higher mean H-index values observed for male academics at each academic rank, even after adjustment for career duration.6,7 For these studies, overall mean H-index values and corresponding standard errors were calculated for each academic rank by combining male and female data.
Meta-analysis findings
Pooled effect size estimates (means) for subgroup analysis
Consistent with these findings, the I2 statistic indicated substantial overall heterogeneity (I2 = 99%). Subgroup analyses demonstrated moderate heterogeneity among Assistant Professor studies (I2 = 64.75%), high heterogeneity among Associate Professor studies (I2 = 86.13%), and low heterogeneity among Full Professor studies (I2 = 0%).
The Forest Plot (Figure 2) depicts the effect sizes for each academic rank, together with their 95% confidence intervals, relative study weightings, subgroup pooled estimates, and the overall pooled effect size. Forest plot.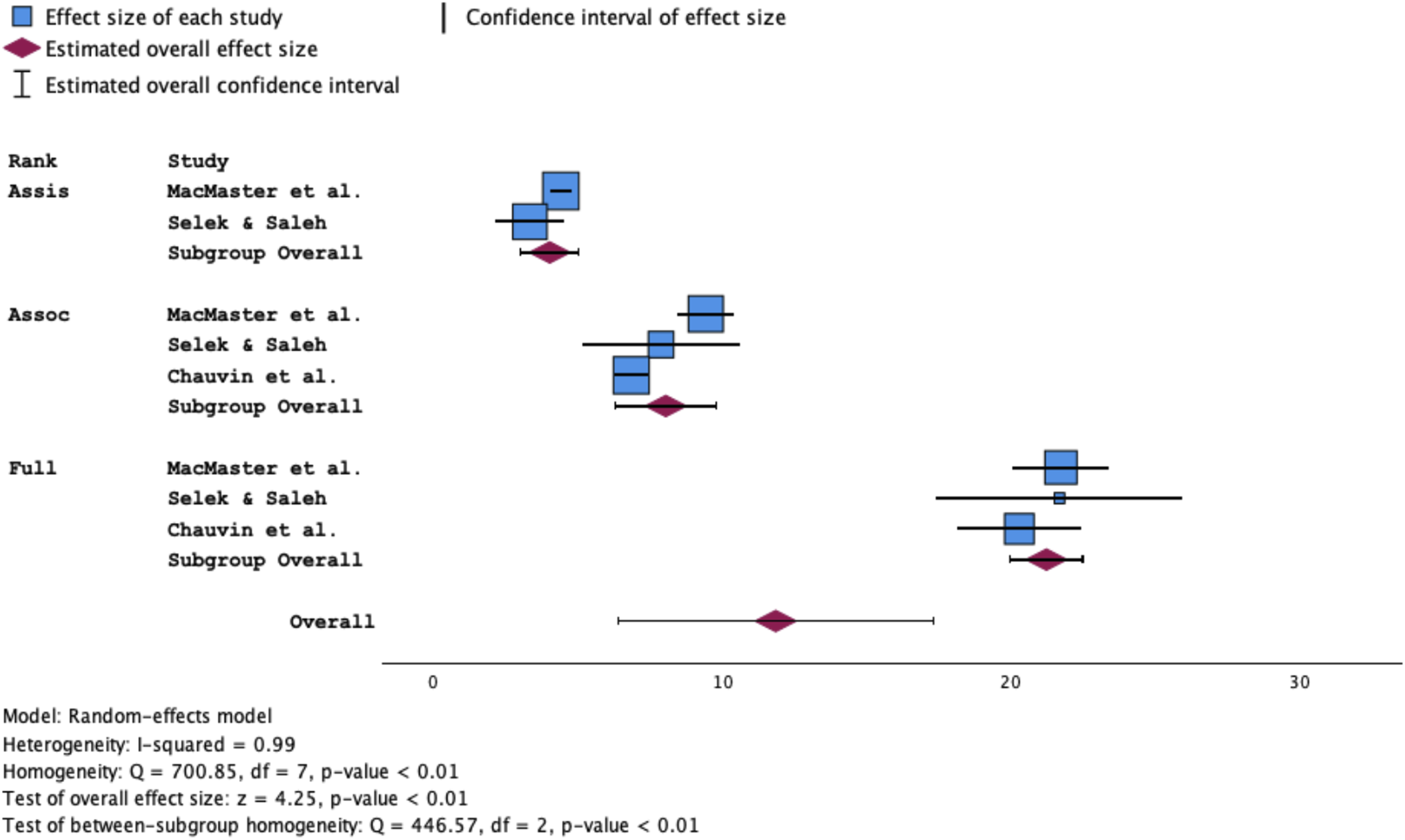
Discussion
To date, and based on a review of PROSPERO registrations, there appears to be no published meta-analysis of H-index values across professorial academic ranks within the discipline of psychiatry. Accordingly, the results from our study are novel. Our principal finding is that, consistent with prior research in multiple medical and surgical disciplines,
1
mean H-index increases in parallel with seniority of academic rank. Using pooled estimates, benchmark values were identified for each professorial level, providing contextual reference points for comparing research productivity across individuals and institutions. When compared with other medical and surgical disciplines using data from the most recent multidisciplinary meta-analysis,
1
psychiatry ranked low for Assistant Professors (2 out of 14) and Associate Professors (3 out of 14), and at the median level (7 out of 13) for Full Professors (Figure 3). These findings suggest that research productivity, as measured by the H-index, lags behind many other specialties at junior and mid-career stages, while converging at senior academic levels. Overall, professorial rank accounted for nearly two-thirds of the variance in H-index across studies, indicating that academic rank is a major determinant of research productivity within psychiatry. Mean H-index stratified by rank comparing different medical disciplines. Note: No mean H-index data available for General Surgery for Full Professor.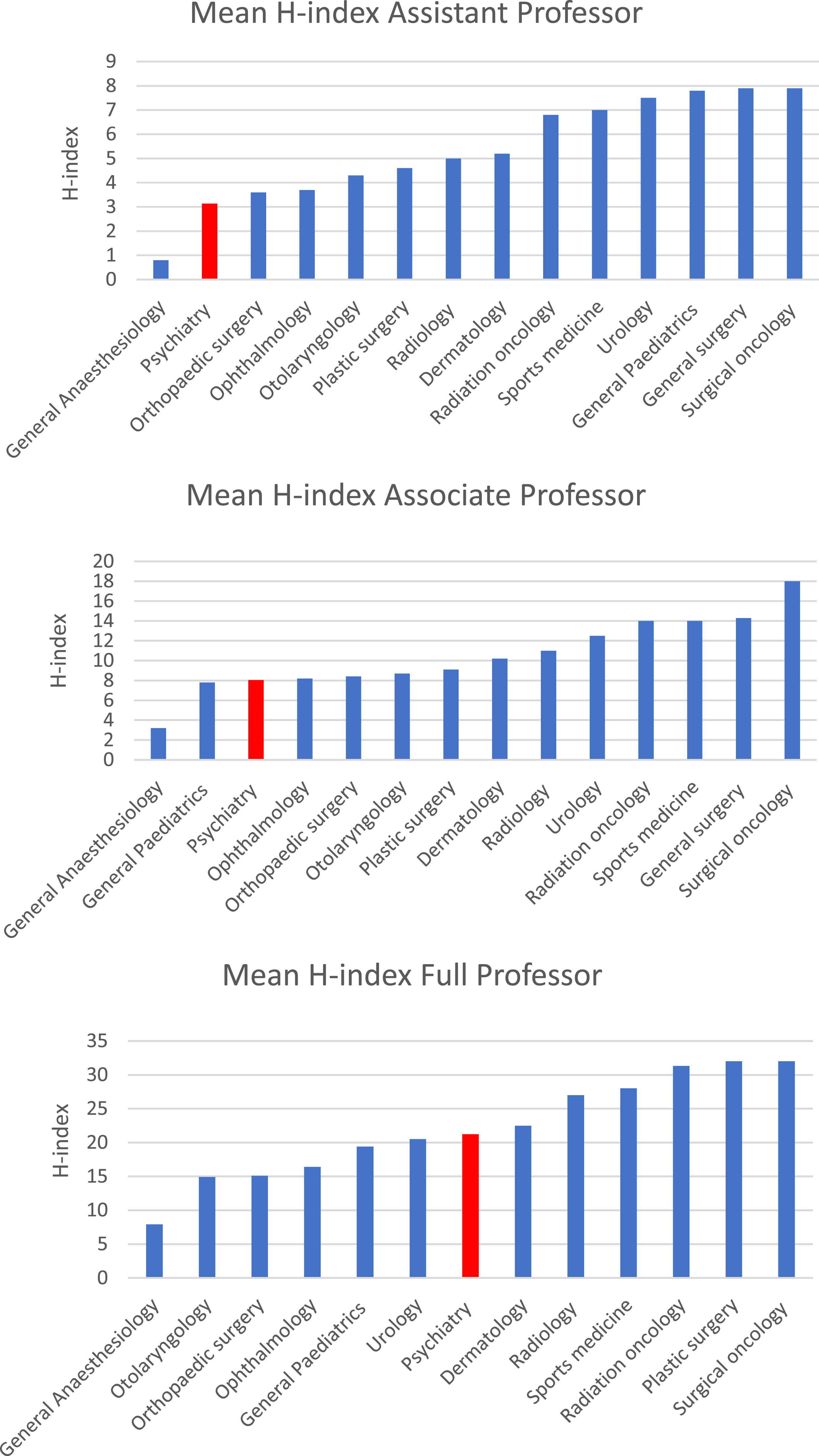
However, the studies included in this meta-analysis surveyed only US and Canadian universities, which may limit the generalisability of findings beyond the North American context. In Australian and New Zealand universities, career-graded academic levels are commonly mapped to North American academic ranks, with Australian Level B (Lecturer) broadly equivalent to Assistant Professor, Australian Level C (Senior Lecturer) aligning more closely with Associate Professor, and Australian Level D (Associate Professor) comparable to Full Professor, although responsibilities and expectations vary by institution. 9 There are currently no published Australian or New Zealand studies reporting H-index benchmarks stratified by professorial academic rank in psychiatry, representing a significant evidence gap. Although Australia, New Zealand and the United Kingdom share broadly similar university promotion frameworks with North America, differences in healthcare funding models, academic employment structures, and access to protected research time may influence research productivity and bibliometric outcomes across academic ranks. In Australia, clinical academic appointments commonly involve split university-health service contracts, with protected research time varying by institution, jurisdiction, and grant support. These structural differences may affect research output and citation accrual among academic psychiatrists, underscoring the need for Australasian H-index benchmarks.
Beyond these geographical considerations, it is also important to recognise the intrinsic methodological limitations of the H-index itself. Although the H-index is a widely used measure of research productivity and impact, it has several important shortcomings. It tends to favour researchers who have been publishing for longer periods, since the index increases with a greater number of publications and citations. Consequently, it may undervalue early-career academics who produce high-quality research at a rapid rate but have had limited time in their academic careers. Another limitation is that publication counts vary across databases. For instance, Google Scholar includes conference abstracts, which can spuriously inflate publication numbers, while Scopus may misclassify authors under multiple identifiers (e.g. maiden and married names). 1 The H-index should also be interpreted with caution, as it can vary by discipline, be inflated by self-citation or citation cartels, and fails to distinguish between single- and multi-authored works. 1 While its inability to differentiate between middle, first, and last authors is a limitation, the H-index nonetheless has the advantage of recognising collaborative contributions rather than excluding them. Accordingly, the H-index should be interpreted as a contextual indicator rather than a definitive measure of academic merit.
In response to these limitations, alternative metrics have been developed to complement or refine the H-index, and these could be valuable in future studies of academic psychiatry. 2 The M-index adjusts for career duration by dividing an individual’s H-index by the number of years since their first publication, thereby providing a fairer measure of trajectory and mitigating disadvantage to early-career researchers. The G-index, proposed by Egghe in 2006, gives more weight to highly cited publications by defining the largest number G of papers that together received at least G2 citations. 10 This allows researchers with a few highly influential papers to receive higher scores than would be reflected by their H-index alone. Another promising indicator is the Relative Citation Ratio (RCR), introduced by Hutchins et al. in 2016, which normalises citation rates by comparing a paper’s citation frequency to that of its co-citation network. 2 This field- and time-normalised, article-level metric evolves dynamically as citation networks change and could provide a more nuanced assessment of research impact within psychiatry. Together, these complementary metrics may provide a more comprehensive assessment of research impact when used alongside the H-index.
National higher education statistics show that “teaching-only” (or education-focused) academic positions have increased substantially in Australia over the last decade – nearly doubling in full-time equivalent (FTE) terms from 2015 to 2024. 11 Many Australian universities now have formal academic promotion policies that explicitly allow for education-focused or teaching-focused pathways.12,13 While these policies often permit academics to apply for promotion (including for professorial positions) based primarily on excellence in teaching and educational leadership rather than research criteria, there is no discipline-specific evidence that psychiatry professors are being appointed primarily on teaching achievements instead of research.12,13 The Steering Group appointed by the RANZCP board have encouraged academic psychiatrists to integrate clinical practice with both academic research and teaching, thereby enabling contributions which are critical for the primary investigation, translation, and dissemination of novel findings regarding the prevention, early detection, diagnosis, and evidence-based management of psychiatric disorders. 14 Although the development of a metric analogous to the H-index for academic teaching is intuitively appealing and should be considered, its implementation is inherently challenging due to the heterogeneity of teaching roles, variation in teaching intensity and scope, discipline-specific educative requirements and approaches, and the subjectivity and context-dependence of commonly used indicators such as student evaluation tools.
Several limitations of the present review should be noted. First, the number of eligible studies was small and restricted to North America, although the combined sample of over 10,000 academics lends statistical strength to the derived benchmarks. Second, incomplete reporting in two studies limited the data available for meta-analysis. Third, the use of different bibliographic databases (Scopus, Web of Science, Google Scholar, and Microsoft Academic Search) may have introduced variability in reported H-indices between studies.
Future research should examine why Assistant and Associate Professors in psychiatry demonstrate comparatively lower benchmark H-indices, whereas Full Professors rank at the median level across disciplines. Potential explanatory factors may include delayed entry into academic psychiatry following prolonged clinical training, reduced access to protected research time at junior and mid-career stages, greater teaching and clinical service demands, and lower research output thresholds within appointment and promotion committees relative to other disciplines. Studies conducted outside North America would enhance international benchmarking and could explore stratification by world-university ranking or healthcare-system type to provide truly global comparisons.
Beyond methodological issues, structural challenges confront academic psychiatry, and academic medicine more broadly. The proportion of physicians engaged in research in the United States has declined dramatically from 4.75% in the 1980s to 1.5% in 2022. 15 In the United Kingdom between 2004 and 2023, total academic psychiatry posts fell by 38% from 330 to 206, even though medical schools expanded by 53% (from 30 to 46). 16 Although comprehensive workforce or bibliometric data for Australian academic psychiatrists are lacking, policy commentary suggests similar pressures on clinician-researchers in Australia and New Zealand.17,18 These trends highlight the importance of situating bibliometric benchmarks within broader workforce and policy contexts.
Bibliometric benchmarks do not exist in isolation but both reflect and shape the academic environments in which clinician-scientists operate. Building capacity and cultivating future leaders in academic psychiatry are essential for sustaining the discipline’s leadership in evidence-based care and for ensuring that new discoveries translate rapidly into improved clinical outcomes.17,19 Yet fewer psychiatrists appear to be pursuing academic careers, and those who do often face significant obstacles.17,18 The RANZCP President’s update in October 2025 stated that academic psychiatry is at a “critical juncture,” due to “declining funding, limited career pathways, and increasing clinical demands that constrain research and teaching.” 18 More broadly, there have even been warnings of an existential threat to clinician-scientists, who are increasingly pressured either to abandon research altogether or to become “desktop scientists” analysing large datasets rather than conducting experimental studies that drive genuine discovery.17,20 To reverse these trends, Utz et al. proposed a multifaceted strategy including immersive researchexperiences for medical trainees, reduced financial barriers to academic careers, revitalised mentorship, and stronger physician-scientist networks. 15 An Australian perspective on these issues would be particularly valuable given the Royal Australian and New Zealand College of Psychiatrists’ recent initiatives to examine and strengthen the academic psychiatry workforce. 17
Conclusion
Our systematic review and meta-analysis demonstrate that H-index increases with successive academic rank among North American psychiatrists. Pooled benchmark H-indices have been identified for each rank, though generalisability is limited by the small number of studies available and their restriction to American and Canadian institutions. The H-index should not be used in isolation for evaluating faculty performance, as academic excellence also encompasses clinical care, education, mentorship, leadership, research grant income, and professional and community service. Future research should examine the integration of the H-index with alternative metrics such as the M-index, G-index, and Relative Citation Ratio, ideally across comparable international contexts and healthcare systems. Consideration should be given to the development of composite measures that capture both research and teaching contributions.
Footnotes
Author contributions
All authors have satisfied: substantial contributions to the conception or design of the work; the acquisition, analysis, or interpretation of data for the work; drafting the work or revising it critically for important intellectual content; final approval of the version submitted; and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: PAM, TB, SA, FAW, and JCLL are editorial team members for the journal and were not involved in the independent editorial assessment or peer-review of the paper.
Data Availability Statement
Data sharing is not applicable as no new data were generated or analysed during this study.