
Abstract
Objectives
To compare vascular risk factors among patients receiving maintenance electroconvulsive therapy (M-ECT) versus acute ECT, and to examine cognitive outcomes associated with M-ECT.
Methods
A retrospective, single-centre, matched case-control study was conducted using a regional Health Service ECT Register (2015–2023). Adults with DSM-5 mood disorders were included. 25 received ≥6 months of M-ECT and 37 received acute-only ECT. Frequency matching achieved similar age structure and sex distribution. Vascular risk factors (hypertension, dyslipidaemia, diabetes, stroke, myocardial infarction, smoking) and a composite “high vascular risk” score (≥2 factors) were compared using Fisher’s exact tests and logistic regression. Cognition was assessed with the Montreal Cognitive Assessment (MoCA) at baseline and longitudinally with linear mixed-effects models.
Results
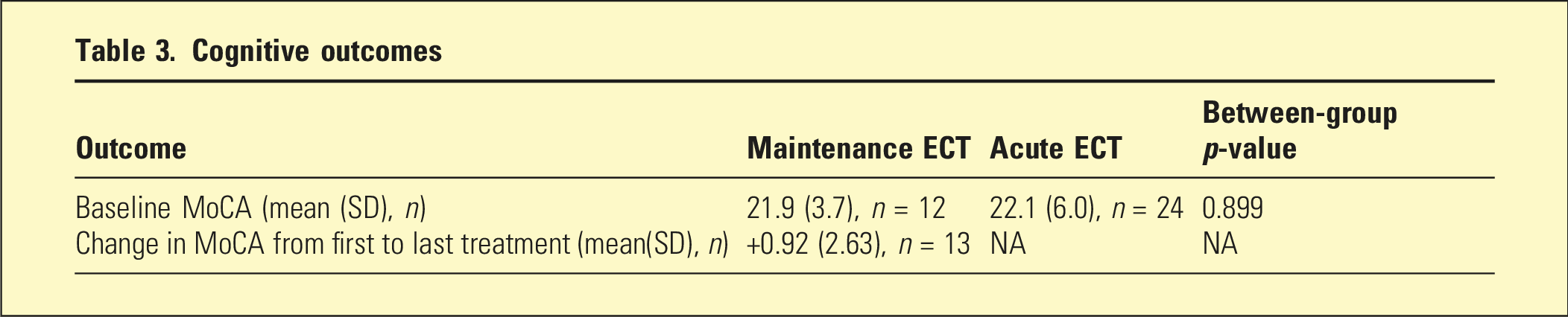
High vascular risk was common in both groups (M-ECT 76%; acute-only 68%) without significant between-group difference, although dyslipidaemia was more prevalent in the M-ECT group (OR 5.52, 95% CI: 1.51–20.20; p = 0.049). Baseline MoCA was comparable (21.9 vs 22.1) and remained stable during M-ECT (mean change +0.92; 95% CI: −0.51 to +2.35). High vascular risk, not ECT group, predicted cognition (−4.64, 95% CI: −7.45 to −2.01; p = 0.002).
Conclusions
Cognitive performance remained stable during M-ECT. Lower scores were associated with vascular comorbidity, and the higher dyslipidaemia rate underscores the need for cardiometabolic and cognitive monitoring.
ECT is effective for severe, treatment-resistant depression, yet relapse following an acute course is common. 1 Maintenance ECT (M-ECT) is used to reduce recurrence in selected patients with treatment-resistant mood disorders. 2 The local Clinical Practice Recommendation from 2017 suggests that M-ECT should be considered for cases with poor response to pharmacotherapy. 3 However, there has been limited study of the patient population that actually receive M-ECT. Previous literature reporting on M-ECT has either had heterogeneous patient population (n = 14; schizophrenia = 5, bipolar disorder = 7, and depression = 2) 4 or primarily focused on acute ECT. 5
The vascular depression hypothesis posits a link between cerebrovascular burden and antidepressant non-response/recurrence in late life. 6 A systematic review found that cardiovascular disease was the most commonly reported physical predictor of treatment-resistant depression (TRD). 7 These mechanisms could plausibly increase the likelihood of requiring M-ECT. We conducted a matched case-control study to test whether vascular risk factors differ between M-ECT cases and acute-only controls, and to describe cognitive outcomes associated with ECT in a single institution.
The aims of this study were to (1) describe M-ECT cohort including vascular risk factors and outcomes, (2) compare vascular risk factors between those receiving M-ECT versus acute ECT, and (3) identify predictors of cognitive outcomes between vascular risk factors + ECT type (M-ECT vs acute ECT).
Materials and methods
Design and setting
The study was a retrospective matched case-control study of adults treated within a regional Health Service, using the ECT Register and electronic medical records from 2015 to 2023. Inclusion criteria were all adults aged 18 years and over with a DSM-5 mood disorder (major depressive disorder or bipolar disorder) who received ECT during the study period. Acute-only ECT was defined as a course of ECT administered at least twice per week. Maintenance ECT (M-ECT) was defined as ≥ 6 months of ECT after an acute course, delivered at reduced frequency compared to acute ECT. 8 Exclusion criteria included primary psychotic disorders as an index indication.
Cases and comparator matching
Between 2015 and 2023, there were 25 eligible patients who received M-ECT. Controls were selected from the same register period using frequency matching to the case distribution by sex (exact) and age (5-year bands) at an approximate ratio of 1:1.5 (cases:controls). Matching variables were also included as covariates in adjusted analyses to account for any residual imbalance. Between 2015 and 2023, there were 37 eligible patients who solely received acute ECT.
Variables
Data were collected from a regional Health Service Electroconvulsive Treatment Register and local medical records databases. Records were reviewed independently by two authors. Covariates recorded included demographic variables (age at ECT phase and sex); clinical variables (diagnosis, mental health legislation status, history of psychiatric hospitalisations, and use of psychotropic medications); ECT variables (number of treatments, type of ECT used); and vascular risk factors, including smoking and alcohol use, hypertension, dyslipidaemia, type 2 diabetes, and past stroke (confirmed by neuroimaging). Cognition was assessed via Montreal Cognitive Assessment (MoCA) tool, which has been validated for monitoring of cognitive function during an ECT course. 9
Outcomes
The primary outcome was the association of each vascular risk factor with case status (M-ECT vs acute). We also calculated the Risk Factor Composite Score, which is a composite measure of vascular risk. To be consistent with the existing literature, we defined high vascular risk as the presence of two or more vascular risk factors. 10 Secondary outcomes included MoCA at baseline, within-person change in MoCA score over time, and adverse outcomes reported in both groups.
Statistical analysis
Group characteristics were reported as mean (SD) or n (%). We compared vascular risk factor prevalence using Fisher’s exact tests, with the p-values adjusted using Benjamini-Hochberg procedure to control the False Discovery Rate (FDR). To reduce overfitting, we fitted separate logistic regression models for each risk factor with age and sex as covariates, reporting adjusted ORs with 95% CIs.
Baseline MoCA was compared using Welch’s t-test; longitudinal MoCA summaries were descriptive. To explore the predictors of MoCA scores over time, we used linear mixed-effects modelling to account for repeated MoCA measurements within individuals. The dependent variable was MoCA score. Fixed effects included group status (M-ECT vs acute-only), vascular risk factor (VRF; dichotomised as ≥2 vs 1 or none), age, sex, and time since baseline assessment. A random intercept for participant was specified to model within-subject correlation. Models were estimated using restricted maximum likelihood through linear mixed-effects regression. Ninety-five percent confidence intervals were derived using non-parametric bootstrap resampling (1000 iterations). Statistical significance was set at p < 0.05 (two-tailed). Analyses used Jamovi 2.6.22.0 and R 4.4.0 (R Core Team, 2024). Missing data were handled with complete-case analysis.
Ethics approval statement
This retrospective study received approval from the local Human Research Ethics Committee (HREC). All patient information was de-identified, and patient consent was not required.
Results
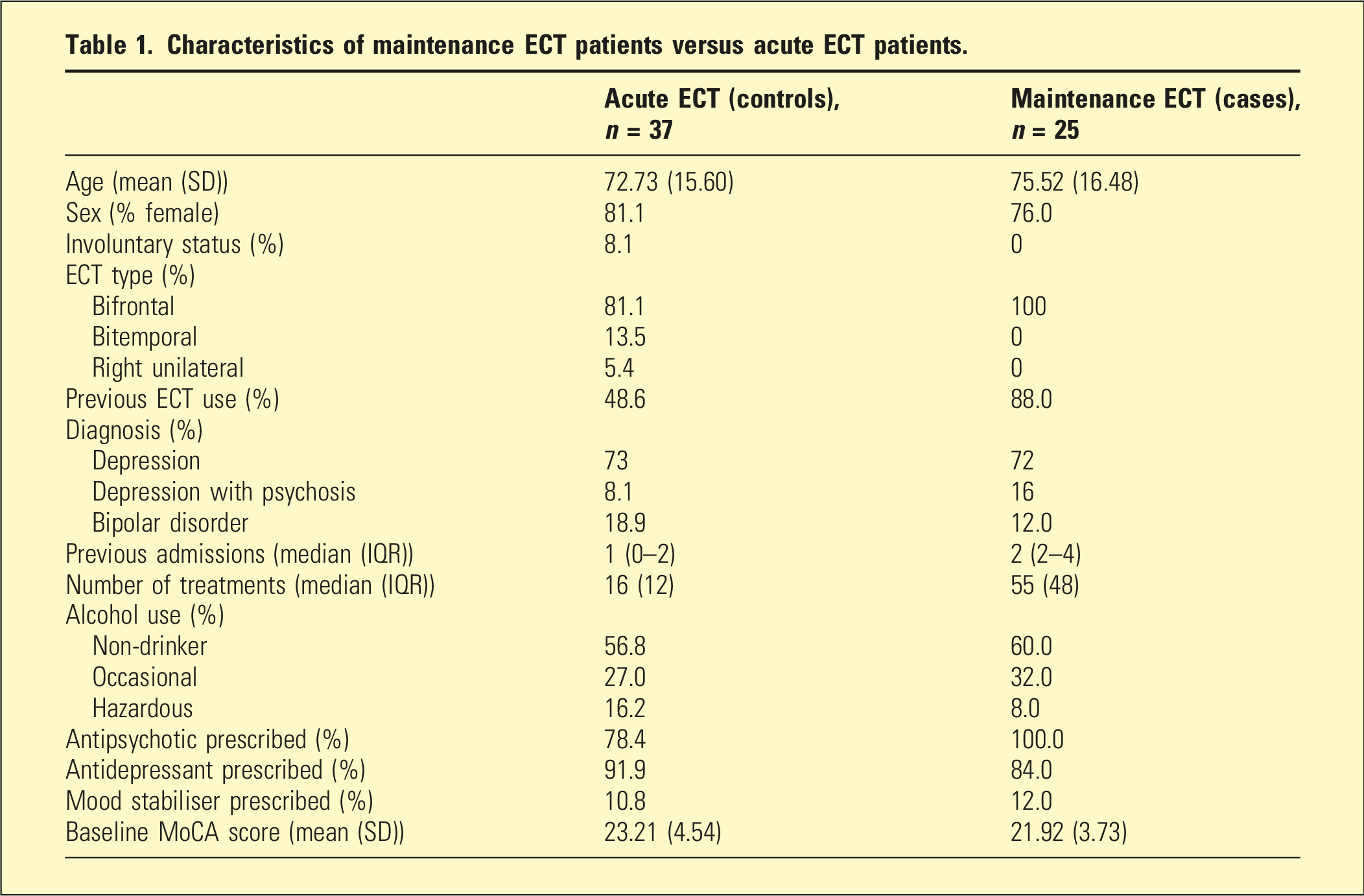
Characteristics of maintenance ECT patients versus acute ECT patients.
Adverse outcomes between groups
Within the M-ECT cohort, there were 5 adverse outcomes reported. These included three episodes of severe hypertension, one episode of asystole, and one episode of complete heart block. There were no deaths. Eight adverse outcomes were reported in the acute ECT group: one episode of supraventricular tachycardia, two episodes of oxygen desaturation, and five episodes of severe hypertension requiring treatment.
Vascular risk factors
Characteristics of maintenance ECT patients versus acute ECT patients.
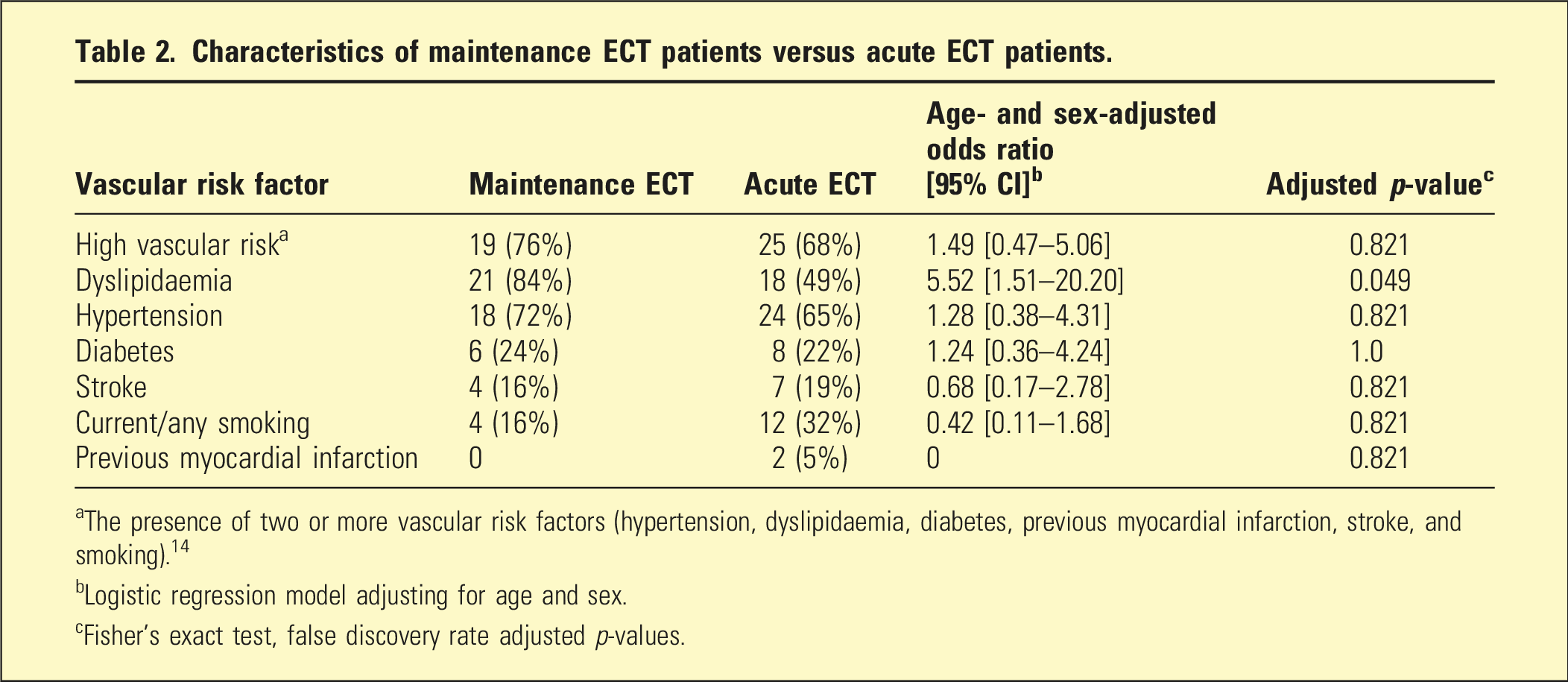
aThe presence of two or more vascular risk factors (hypertension, dyslipidaemia, diabetes, previous myocardial infarction, stroke, and smoking). 14
bLogistic regression model adjusting for age and sex.
cFisher’s exact test, false discovery rate adjusted p-values.
Cognitive outcomes
Cognitive outcomes
In the linear mixed-effects model adjusting for age, sex, and time, with group type (M-ECT vs acute-only) and composite vascular risk factor status entered as fixed effects, only vascular risk factor status was significantly associated with MoCA scores. Participants with one or more vascular risk factors scored on average 4.6 points lower on the MoCA compared to those without VRFs (estimate −4.64, 95% CI: −7.45 to −2.01, p = .002). By contrast, group type was not associated with MoCA (estimate 0.17, 95% CI: −2.42 to 2.45, p = .89). This indicates that vascular comorbidity, rather than ECT group status, accounted for poorer MoCA scores in this cohort, as displayed in Figure 1. Montreal cognitive assessment (MoCA) scores over time by vascular risk factor status, estimated from the linear mixed-effects model adjusting for age, sex, and group type (M-ECT vs acute-only). Participants with high vascular risk (orange line, shaded 95% CI) consistently scored lower than those without vascular risk factors (blue line, shaded 95% CI). No significant change in MoCA scores was observed over time in either group (A = M-ECT; B = acute-only).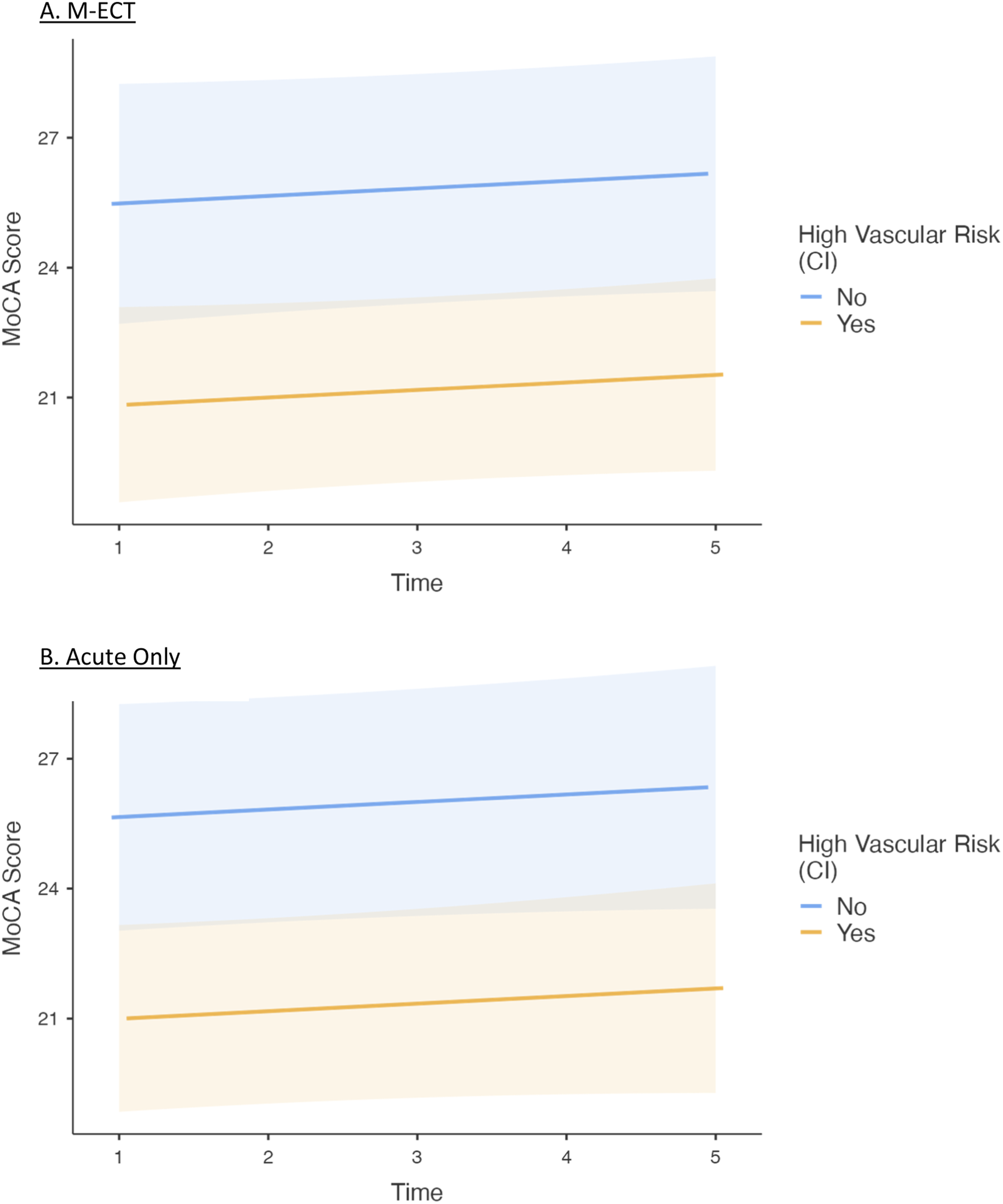
Discussion
In this matched case-control study from a regional Australian service, dyslipidaemia was substantially more common in patients who proceeded to M-ECT than in those who received an acute course only. By contrast, hypertension, diabetes, prior stroke, previous myocardial infarction, and smoking did not differ meaningfully between groups, although confidence intervals for these estimates were wide. Importantly, our cognitive results align with prior evidence that continuation/M-ECT does not produce clinically meaningful deterioration at the group level. Baseline MoCA was similar between groups and within-person change during maintenance was stable, which complements outcomes reported in PRIDE Phase 2 and its longitudinal neurocognitive follow-up, as well as meta-analytic data.11–13 Interpretation of these findings should consider that MoCA scores are not always significantly influenced by current depressive symptom severity. 14 The relatively low baseline scores in our study are consistent with normative data in older adults and likely reflect age-related cognitive decline, reduced cognitive reserve, and a higher burden of subclinical neurodegenerative and medical comorbidity.15,16 Although both groups were predominantly female (76% vs 81%), no significant gender differences were identified, and sex was not associated with cognitive outcomes in adjusted analyses. Our study also highlights the importance of optimising cardiovascular risk factors in individuals with depression, given the significant impact this has on global cognitive score as measured by the MoCA.
Surprisingly, there were no significant differences in vascular risk factors between individuals receiving maintenance and acute courses of ECT, other than dyslipidaemia which was marginally significant. The research on individual vascular risk factors has been mixed, hence the use of composite measures to categorise high and low vascular risk patients.17,18 Notably, our cohort had significantly high presence of vascular risk factors (76% in M-ECT and 68% in acute-only ECT had ≥2 risk factors), compared to previous studies investigating vascular risk factors in acute-only ECT (40–49%).18,19 Overall, our finding of high ECT usage in this vascular depression cohort is consistent with the broader vascular depression literature demonstrating that ECT is superior to pharmacotherapy alone in achieving remission.18,19
Overall, these findings are consistent with the broader vascular depression literature linking cerebrovascular burden to treatment resistance and recurrence. However, causality cannot be inferred, and further studies are needed to clarify whether dyslipidaemia contributes directly to M-ECT need or represents a correlate of more severe, recurrent illness.18,19
Clinical implications follow directly from these observations. First, cardio-metabolic assessment and treatment should be routine when considering or continuing M-ECT, with explicit attention to lipid profiles and optimisation of dyslipidaemia alongside usual mood-disorder care. Given the haemodynamic effects of ECT and anaesthesia associated with the treatment, proactive management of blood pressure is prudent even though hypertension prevalence did not differ statistically between groups. Our adverse-event profile, with several severe hypertensive episodes, underscores this point. 20 These events are consistent with the known biphasic autonomic response to ECT, which can be characterised by asystole, 21 transient arrhythmias and hypertension. Prior studies indicate that these effects are typically short-lived and manageable, even in medically complex populations. 22 Lifestyle-based interventions recommended by international taskforces may be particularly relevant in this older cohort, complementing pharmacotherapy and ECT.23,24 Finally, our study can reassure patients, families, and clinicians that M-ECT is not associated with cognitive decline, consistent with previous literature. 25 This is further supported by studies comparing commonly used anaesthetic agents, such as propofol and etomidate, which demonstrate no significant differences in cognitive outcomes, depressive symptom improvement, or ECT parameters between groups. 26
Several limitations temper interpretation. The regional context introduces unique factors that may have influenced these findings. Variability in access to preventive and specialist care may also affect the identification and management of vascular risk factors, potentially leading to underestimation or misclassification. In addition, patterns of service use in regional settings, including later presentation and greater illness severity, may contribute to a more medically complex cohort. The analysis is retrospective, single-service, and modest in size, with binary registry coding of vascular risks (no timing, severity or laboratory thresholds), unmeasured confounders (e.g., statin use, intensity of antihypertensive therapy, BMI, and renal and thyroid function), and missing cognitive data that limit precision and may introduce bias. Matching was at the frequency level rather than individual pairing and residual confounding is therefore possible. Multiple comparisons also raise the chance of false-positive findings.
To build on these exploratory results, future work should use prospective, adequately powered, multi-site designs with pre-specified inclusion/exclusion criteria and adjudicated maintenance designation; quantitative lipid panels and medication exposures (e.g., statins); structural and vascular neuroimaging (e.g., white-matter hyperintensities with Fazekas ratings and diffusion metrics); inflammatory markers; and richer neuropsychological batteries alongside MoCA. Designs that incorporate time-to-event outcomes (e.g., time to maintenance initiation, relapse, or hospitalisation) and causal approaches (e.g., propensity methods or mediation analyses to test whether vascular burden mediates the path from treatment resistance to M-ECT) would advance the field.
In conclusion, this single institution study contributes to the limited literature on M-ECT by describing the vascular and cognitive characteristics of patients requiring this treatment. By identifying possible vascular risk factors that may influence the transition from acute to M-ECT, this study contributes to a deeper understanding of the patient profiles requiring ongoing treatment. While no significant predictors beyond dyslipidaemia were identified, the prevalence of vascular comorbidities in this population highlights the need for further research to clarify their role in treatment-resistant depression and M-ECT. Understanding these risk factors could help inform clinical decision-making and enhance the long-term management of patients undergoing M-ECT.
Footnotes
Acknowledgements
Matthew Kang is supported by the Nick Christopher PhD scholarship and the Research Training Program Scholarship from the Department of Psychiatry, University of Melbourne, with contributions from the Australian Commonwealth Government, and the Ramsay Hospital Research Foundation.
Ethical considerations
This study received approval from the Human Research Ethics Committee (HREC), Barwon Health (approval# QA/106728/VICBH-2024-421309(v2)) on April 08, 2024. This is an HREC-approved retrospective study, all patient information was de-identified, and patient consent was not required. Patient data will not be shared with third parties.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Malcolm Forbes is supported by a Deakin University PhD Scholarship, the RANZCP Foundation, and has received funding from the NHMRC and Avant Mutual.
Matthew Kang is supported by the Nick Christopher PhD scholarship and the Research Training Program Scholarship from the Department of Psychiatry, University of Melbourne with contributions from the Australian Commonwealth Government, and the Ramsay Hospital Research Foundation.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data are not publicly available due to ethical restrictions on patient privacy. Anonymised data are available from the corresponding author, [FA], upon reasonable request.