
Abstract
Objectives
In 2021 depressive disorders were the fourth leading cause of Disability-Adjusted Life Years (DALYs) in Australia accounting for 926.92 DALYs per 100,000 people.1 This review aimed to identify which non-pharmacological non-psychological treatments are effective augmentation strategies in treating depression and which primary therapies they most effectively augment.
Methods
PubMed, CENTRAL, and PsycINFO were searched for randomised-controlled trials for non-pharmacological non-psychological augmentation strategies in adults with unipolar depression. The results were synthesised qualitatively following the Synthesis Without Meta-analysis (SWiM) guidelines. Risk of bias was assessed using the JBI critical appraisal tool.
Results
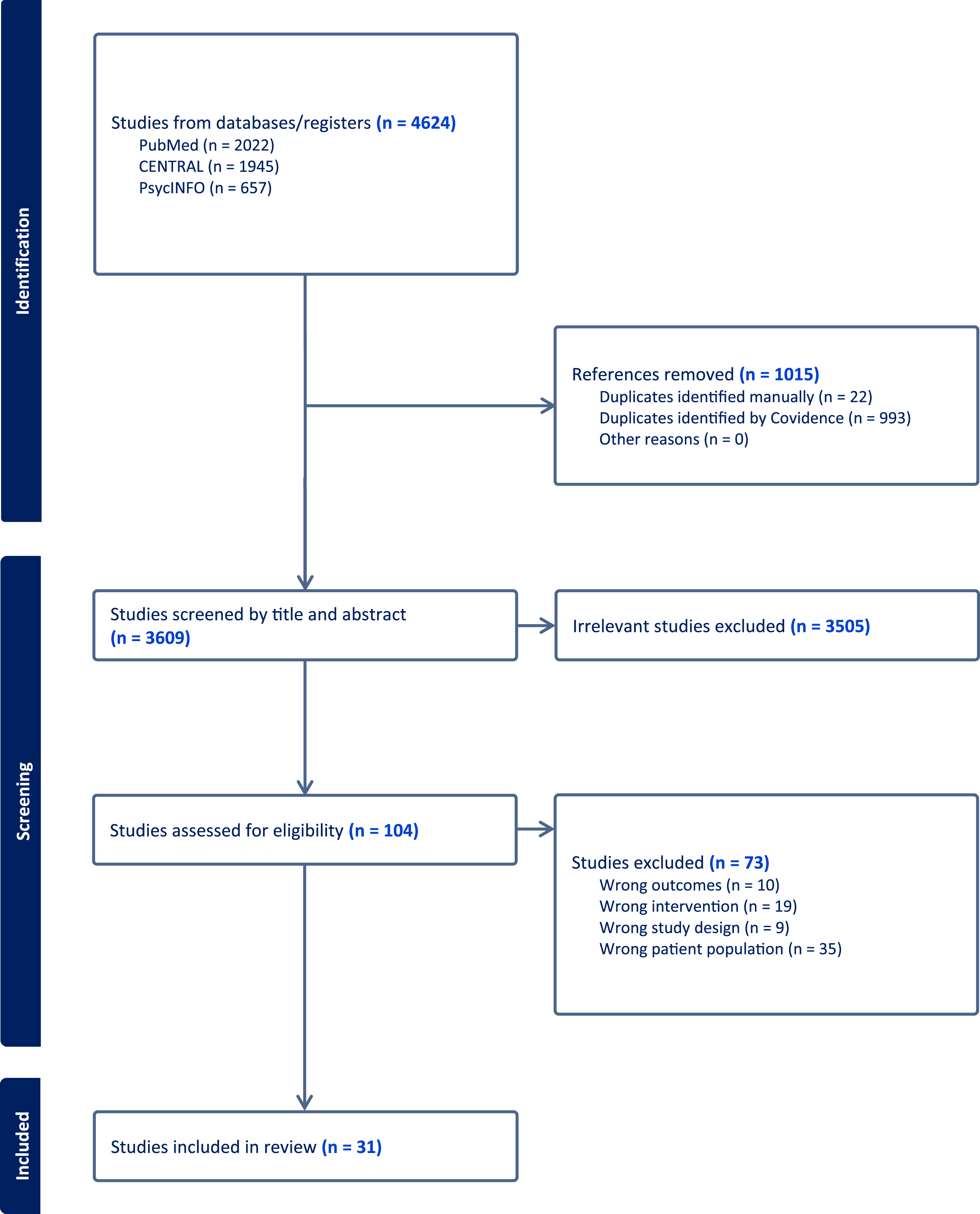
3609 studies were screened against title and abstract and 3505 irrelevant studies were excluded. 104 studies were assessed for full-text eligibility. 31 studies were included for analysis. Included studies investigated augmentation with photobiomodulation, neurostimulation, exercise therapies, probiotics and acupuncture.
Conclusion
Non-pharmacological non-psychological augmentation strategies can be useful for patients with suboptimal response to standard treatment; however, more high-quality large RCTs are needed to investigate the effectiveness of these treatments in augmenting specific therapies. Due to their low cost and favourable safety profiles bright light therapies and exercise should be considered to augment standard treatment in adults with depression. There is lower levels of evidence for acupuncture and probiotics.
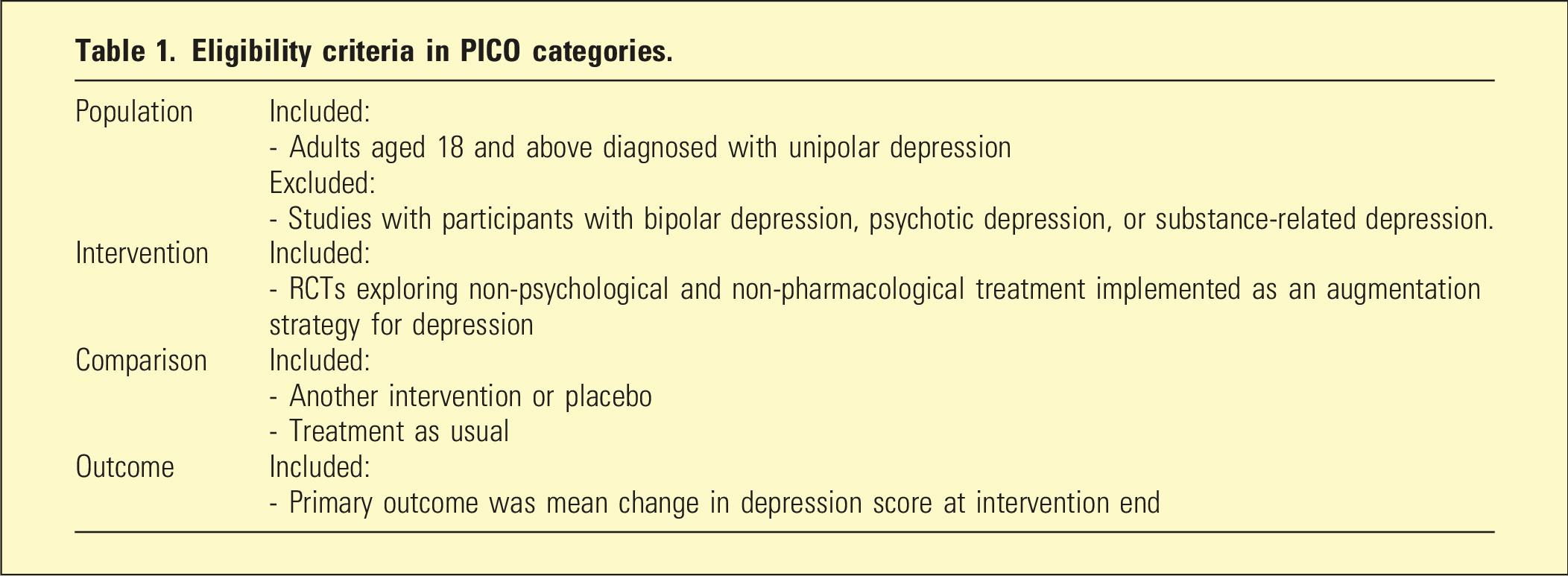
Eligibility criteria in PICO categories.
Methods
A systematic review of the literature was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA). 8 Ethics approval was not required for this study.
Search strategy
Two reviewers independently searched PubMed, CENTRAL, and PsycINFO on the 25th March 2025 for English language studies published between 1st January 1980 and 25th March 2025. Supplemental file 1 contains the full search strategy for each database.
Study selection
The eligibility criteria were constructed to capture studies in which the intervention was implemented and investigated as an augmentation strategy to another primary treatment. Studies were included if they met the following criteria: (a) participants were adults aged 18 and above diagnosed with a unipolar depression, (b) study design was a prospective randomised-controlled trial, (c) primary outcome measure was change in depression score at intervention end, and (d) the augmentation strategy was a non-psychological non-pharmacological treatment (Table 1). The comparator could be another intervention or treatment as usual. Studies were excluded if the intervention was not implemented as an augmentation strategy, or if they included participants with bipolar depression, psychotic depression, or substance-related depression. Conference abstracts and pilot studies were excluded. The titles and abstracts of studies selected were screened independently by two reviewers to identify studies that potentially meet the selection criteria. The full text of the identified studies was assessed independently by two reviewers for inclusion. A third person resolved any discrepancies.
Data selection
Two reviewers independently extracted the data from each study which included study design and characteristics, number of participants, participant demographics, intervention and comparators characteristics, outcome measures, and results presented in tabular form.
Quality appraisal
Risk of bias in the studies was assessed using the Joanna Briggs Institute (JBI) critical appraisal tool for randomised-controlled trials independently by two reviewers and a third person resolved any discrepancies. 9 The overall risk of bias for each study is assessed as low, high, or unclear.
Data analysis
A meta-analysis was planned for this review however due to the high risk of bias and heterogeneity in the studies retrieved, a meta-analysis was not considered appropriate (see Table 3 risk of bias assessment). The results were summarised using qualitative synthesis and descriptive statistics following the Synthesis Without Meta-analysis (SWiM) guidelines. 10
Results
On March 25th 2025 a total of 4624 articles were retrieved before removing 1015 duplicates, with 22 duplicates identified manually and 993 duplicates identified by Covidence.
11
3609 studies were screened against title and abstract and 3505 irrelevant studies were excluded. 104 studies assessed for full-text eligibility. 31 studies were included for review (Figure 1). Most studies reported data as mean ± standard deviation, or mean with 95% confidence interval [CI], with significance level set at 0.05. Change in depression score was measured using scales where higher scores indicated more severe depression. In summarising the outcome of change in depression score the mean number of points change is given when reported. For studies where the rate of remission is reported the number needed to treat (NNT) for remission is given. Remission was defined by most studies as a greater than 50% improvement in score from baseline. NNT was calculated by these authors when not given by the paper. PRISMA flow diagram for study selection for systematic review. Generated with covidence.
11
Summary of included studies with results grouped by type of augmentation strategy.
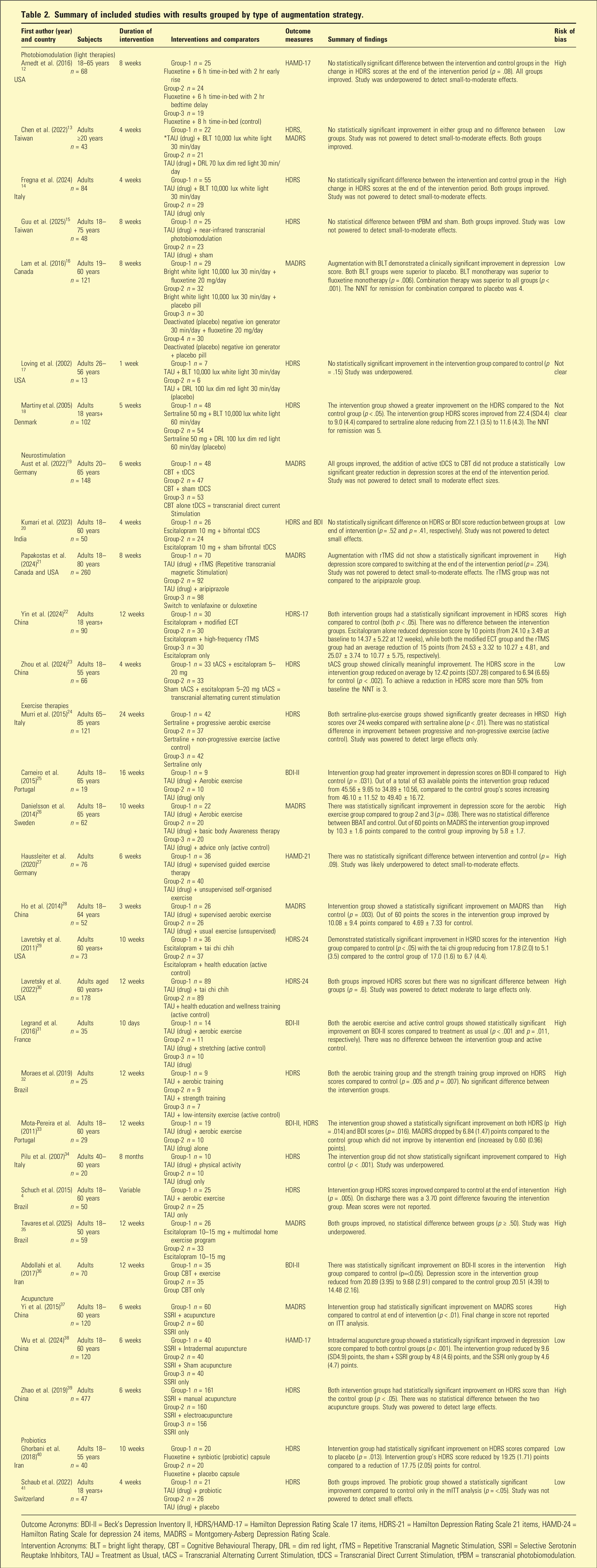
Outcome Acronyms: BDI-II = Beck’s Depression Inventory II, HDRS/HAMD-17 = Hamilton Depression Rating Scale 17 items, HDRS-21 = Hamilton Depression Rating Scale 21 items, HAMD-24 = Hamilton Rating Scale for depression 24 items, MADRS = Montgomery-Asberg Depression Rating Scale.
Intervention Acronyms: BLT = bright light therapy, CBT = Cognitive Behavioural Therapy, DRL = dim red light, rTMS = Repetitive Transcranial Magnetic Stimulation, SSRI = Selective Serotonin Reuptake Inhibitors, TAU = Treatment as Usual, tACS = Transcranial Alternating Current Stimulation, tDCS = Transcranial Direct Current Stimulation, tPBM = transcranial photobiomodulation.
Risk of bias assessment
Risk of bias assessment using JBI critical appraisal tool
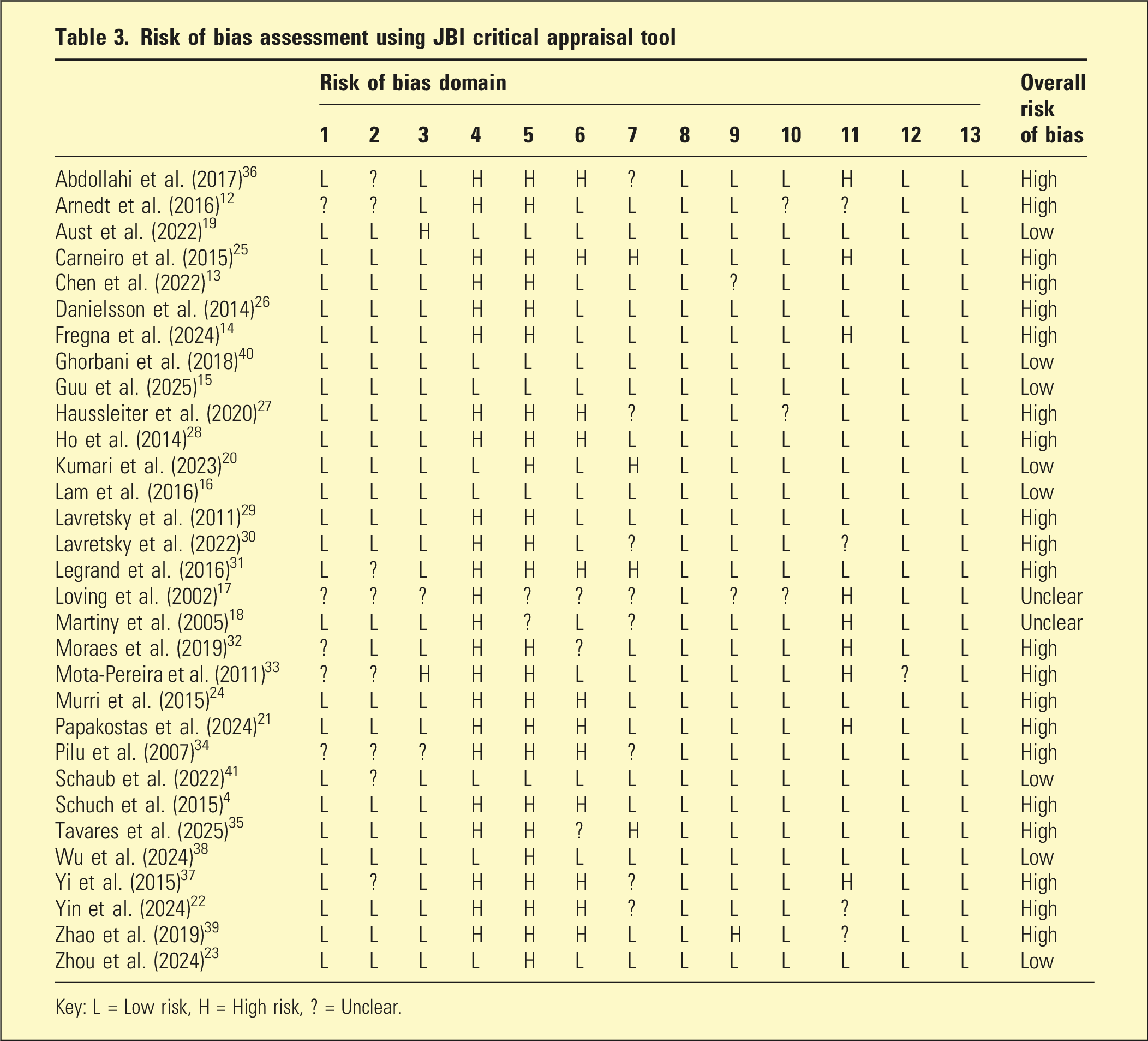
Key: L = Low risk, H = High risk, ? = Unclear.
Discussion
Bright light therapy may have a small effect on reducing depressive symptoms and should be considered as an adjunct to treatment because it has a great safety profile, is easy for patients to undertake in their own home, and is very affordable. 43 The evidence supports a regimen of exposure to 10,000 lux of bright white light for 30 min daily. Physical exercise may provide a small-to-moderate effect when implemented adjunctively and most types of exercise are suitable including aerobic exercise, strength training, and Tai Chi, and can be effective when undertaken both individually and in group formats. Most RCTs used structured supervised exercise programs which may be superior to self-organised exercise, however more evidence is needed. Acupuncture may demonstrate a mild reduction in depressive symptoms and also has a favourable safety profile. Of the neurostimulation techniques tDCS and tACS may offer small benefits. Probiotics may provide a small reduction in depressive symptoms however the evidence is not there to recommend any particular probiotic regimen. The only study on sleep deprivation included in this review found sleep deprivation ineffective. Other augmentation strategies not covered in this review include diet modification and occupational therapy, which the existing literature indicates may have a small effect on reducing depressive symptoms.44,45 There is a large body of evidence supporting rTMS and ECT as primary treatments for depression and as such we have not included these in any further analysis.7,46,47
Many studies included in this review did not use an adequate placebo, sham or active control, and this contributed to an overall high risk of bias. This limits the ability to recommend these interventions as augmentation strategies. Addressing this gap in the evidence base is important due to the ongoing high cost to the community of depression or partially treated depression, and clinicians require high-quality evidence to support treatment regimens.
Limitations
The eligibility criteria were constructed to capture studies in which the intervention was specifically investigated as an augmentation strategy to another primary treatment. As a consequence there were interventions included in this review that would normally be implemented as the primary treatment, including ECT and TMS, as the study investigators implemented these as adjunctive treatments in their clinical trials. This review accepted studies in which change in depression score at intervention end was the primary reported outcome and as a result there were several studies that were excluded due to only reporting the rate of remission as an outcome rather than change in depression score. This review did not investigate the rate of remission or the effect of interventions in accelerating response to treatment or consider follow up. Studies were limited only to articles published in English language.
Conclusions
Non-pharmacological non-psychological augmentation strategies have the potential to improve outcomes in patients with suboptimal treatment response without the burden of increased drug effects. However, more high-quality large placebo-controlled RCTs are needed to generate the evidence needed to support these interventions as augmentation strategies in individualising treatment for depression. The evidence is not yet there for being able to recommended specific augmentation strategies based on the primary treatment. The was limited evidence for acupuncture and probiotics, and improving evidence for bright light therapy and exercise.
Supplemental material
Supplemental material - Systematic review of non-pharmacological non-psychological augmentation strategies for the treatment of unipolar depression: Synthesis without meta-analysis (SWiM)
Supplemental material for Systematic review of non-pharmacological non-psychological augmentation strategies for the treatment of unipolar depression: Synthesis without meta-analysis (SWiM) by Hana Chapman, Rodney Blanch, Nishad Samad in Australasian Psychiatry
Supplemental material
Supplemental material - Systematic review of non-pharmacological non-psychological augmentation strategies for the treatment of unipolar depression: Synthesis without meta-analysis (SWiM)
Supplemental material for Systematic review of non-pharmacological non-psychological augmentation strategies for the treatment of unipolar depression: Synthesis without meta-analysis (SWiM) by Hana Chapman, Rodney Blanch, Nishad Samad in Australasian Psychiatry
Footnotes
Acknowledgements
Non-author contributors: • Emma White contributed to article screening and selection and risk of bias assessment. • Natalie Tam contributed to risk of bias assessment and manuscript editing.
Ethical considerations
Ethics approval was not required for this study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Use of AI declaration
Generative Artificial Intelligence (AI) was not used in the production of this paper.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.