
Abstract
Objectives
To systematically review the effectiveness, safety, and care models of telehealth-supported ketamine for depression and/or anxiety in adults and consider implications for Australasian clinical practice.
Methods
Following PRISMA 2020, we searched for randomised or observational studies of adults receiving at-home telehealth-supported ketamine for depression and/or anxiety, to August 2025. Primary outcomes were ≥50% symptom reduction and remission. Programme characteristics were synthesised narratively. Risk of bias and certainty of evidence were assessed. Protocol was not registered, and the study was not funded.
Results
Of 3,857 records screened, three met criteria, all from US commercial providers. Programmes differed in dosing schedules, clinical staffing, supervision, and safety monitoring. Across up to 16,876 patients, follow-up outcome data were available for a minority. Response ranged 49.5–62.8% (PHQ-9) and 47.6–62.9% (GAD-7), and remission 20.7–32.6% and 23.9–31.3%, respectively. All studies were at critical overall risk of bias. GRADE certainty for effectiveness and safety was very low.
Conclusions
Telehealth-supported sublingual racemic ketamine was associated with symptom improvements in selected populations. Yet, the evidence base is provider generated, and at critical risk of bias. Its main contribution to Australasia is to inform consideration of model components for a future hybrid service design.
Depression and anxiety are a major and growing public health issue across Australia and New Zealand. In Australia, nearly one in three people will experience an anxiety disorder in their lifetime, and about one in six will experience an affective disorder such as depression. 1 Barriers to accessing mental health care in Australia are pronounced outside major cities, where there are fewer specialist mental health services and workforce shortages with increasing distance from metropolitan centres. 2 Telehealth is now an established component of Australian mental health service delivery, including specialist telepsychiatry for people in regional and remote areas.
Ketamine is an N-methyl-D-aspartate (NMDA) receptor antagonist that is increasingly recognised for its efficacy as an antidepressant.3–5 In Australia, intranasal esketamine (Spravato) is approved by the Therapeutic Goods Administration (TGA), and is PBS-listed, for treatment-resistant depression. 6 Racemic ketamine is also used off label for depression in Australian psychiatric practice, 7 although unlike intranasal esketamine it is not TGA-approved for this indication. 8
In Australia and New Zealand, ketamine treatment for depression is governed by controlled-medicine regulation and jurisdiction-specific prescribing requirements.8,9 Contemporary Australasian practice guidance emphasises psychiatrist-led assessment, informed consent, structured monitoring across dosing sessions, and clear escalation pathways.9,10 Intranasal esketamine (Spravato) is used within its approved product licence and in Australia, is administered in treatment centres rather than at-home.6,8 The use of off-label racemic ketamine is addressed in The Royal Australian and New Zealand College of Psychiatrists professional practice guidelines, suggesting a highly structured, clinic-based approach. 8
In parallel with broader expansions in telemedicine in the context of the COVID-19 pandemic, there has been rapid growth in telehealth models that deliver oral or sublingual ketamine for self-administration at-home in the United States (US). 11 Geographical distance remains a significant barrier to accessing mental health care in remote and regional Australia, 12 which may increase interest in alternative ketamine treatment models. Thus, we examine the models of care of US programmes to identify which elements of remote care might inform a potential future hybrid approach, while recognising that direct implementation of at-home ketamine administration in Australia is unlikely under the current regulatory environment.8–10
Notably, telehealth-assisted ketamine administration carries substantial safety concerns. 11 Ketamine is known to carry risks including medical, psychiatric, and dependency risks.13–16 Emerging reports have described serious events, including overdose and severe psychiatric deterioration, in the context of telehealth-prescribed ketamine.11,17 These raise the question of whether current US regulations are sufficient in this rapidly expanding sector. Telehealth-supported at-home ketamine programmes in the US are also not a single, standardised intervention, and differ between providers. Models vary in eligibility screening, prescriber background, dosing strategy, session structure, and the intensity of monitoring during and after administration. The programme structure may influence both effectiveness and safety.
Despite the developments in ketamine provision via telehealth, the evidence base investigating the phenomenon remains insufficient. To our knowledge, no prior review has systematically synthesised outcome data from telehealth ketamine programmes for depression and anxiety and appraised their risk of bias. We therefore conducted a systematic review evaluating at-home, telehealth-supported ketamine administration for adults with depressive and/or anxiety disorders. Our objectives were to (1) summarise symptom and safety outcomes, and to assess the risk of bias of these studies, (2) to rate the certainty of the evidence using the GRADE (Grading of Recommendations Assessment, Development, and Evaluation) framework, 18 and (3) to describe the telehealth-supported ketamine models of care and consider their potential relevance to Australasian clinical practice. Given Australia’s geography, evolving telehealth policy, and increasing availability of ketamine-based treatments, synthesising evidence from telehealth at-home ketamine programmes is directly relevant to Australasian clinical governance and service planning.
Methods
This systematic review followed PRISMA 2020 guidelines, 19 and our PRISMA 2020 checklist can be found as a supplementary file. This review was not prospectively registered, no protocol was prepared, and no amendments were made after commencing the review. We systematically searched PubMed, Embase, PsycINFO, CINAHL, Cochrane Library, and ClinicalTrials.gov trial registry up to August 2025, as detailed in Supplemental File 1. We planned to include randomised controlled trials and observational studies reporting outcomes of adults receiving ketamine administered at-home with telehealth-support to treat depressive and/or anxiety symptoms. We excluded single case reports, case series without systematic follow-up, cross-sectional studies, protocols without reported results, studies of clinic-only interventions, those involving recreational ketamine use, and non-English-language publications. Screening was conducted in Rayyan, 20 where the abstracts, full texts, and data were initially screened and extracted by one reviewer. The second reviewer independently verified the screening process and disagreements were resolved by discussion. Primary outcomes were response (≥50% reduction on PHQ-9 or GAD-7) and remission, with remission defined according to each study’s prespecified criteria. For efficacy outcomes we extracted response and remission proportions at the end of the initial dosing course. We calculated 95% confidence intervals using the Clopper–Pearson method based on available case denominators. For safety outcomes we extracted the percentage of patients with serious adverse events and discontinuation of treatment due to adverse effects. We did not formally assess publication bias as less than 10 studies were included and ethics approval was not required as this study synthesised published, de-identified data.
We planned separate narrative syntheses for depression, anxiety, and safety outcomes, including studies that reported the relevant domain. The prespecified primary timepoint was the post-treatment assessment at the end of the initial dosing course. If multiple timepoints were reported, we extracted the prespecified primary post-treatment timepoint for synthesis and other timepoints were recorded but not synthesised. Meta-analysis, formal heterogeneity exploration, and sensitivity analyses were not performed due to the small number and heterogeneity of included studies. Given the differences in study designs and outcome reporting, a narrative synthesis was undertaken. One reviewer assessed risk of bias using ROBINS-I, 21 and certainty of evidence using GRADE, 18 with verification by a second reviewer.
We used a large language model 22 to assist with wording and structure of the manuscript, and on a few occasions to suggest relevant references, which were checked against the original sources by the authors. It was not used for the formal database searches, study selection, data extraction, or analysis. Final responsibility for content and accuracy rests with the authors.
Results
Review of the literature
Our search strategy, conducted in August 2025, identified 4,079 records from five databases and one trial registry. After removal of 222 duplicates, 3,857 unique records were screened by title and abstract. Nine full-text reports were assessed and six were excluded, with reasons detailed in Supplemental Table 1. The PRISMA flowchart in Figure 1 summarises the selection procedure, which resulted in the inclusion of three papers. Given that we found so few studies that met our inclusion criteria, a meta-analysis was not considered appropriate and a narrative review was performed. The studies that met our inclusion criteria are outlined in Table 1. They included: Hassan et al., Hull et al., and Mathai et al.23–25 All studies examined sublingual racemic ketamine administered at-home with telehealth-support, with a total of up to 16,876 patients across all three studies. Overlap between Hull et al.
24
and Mathai et al.
25
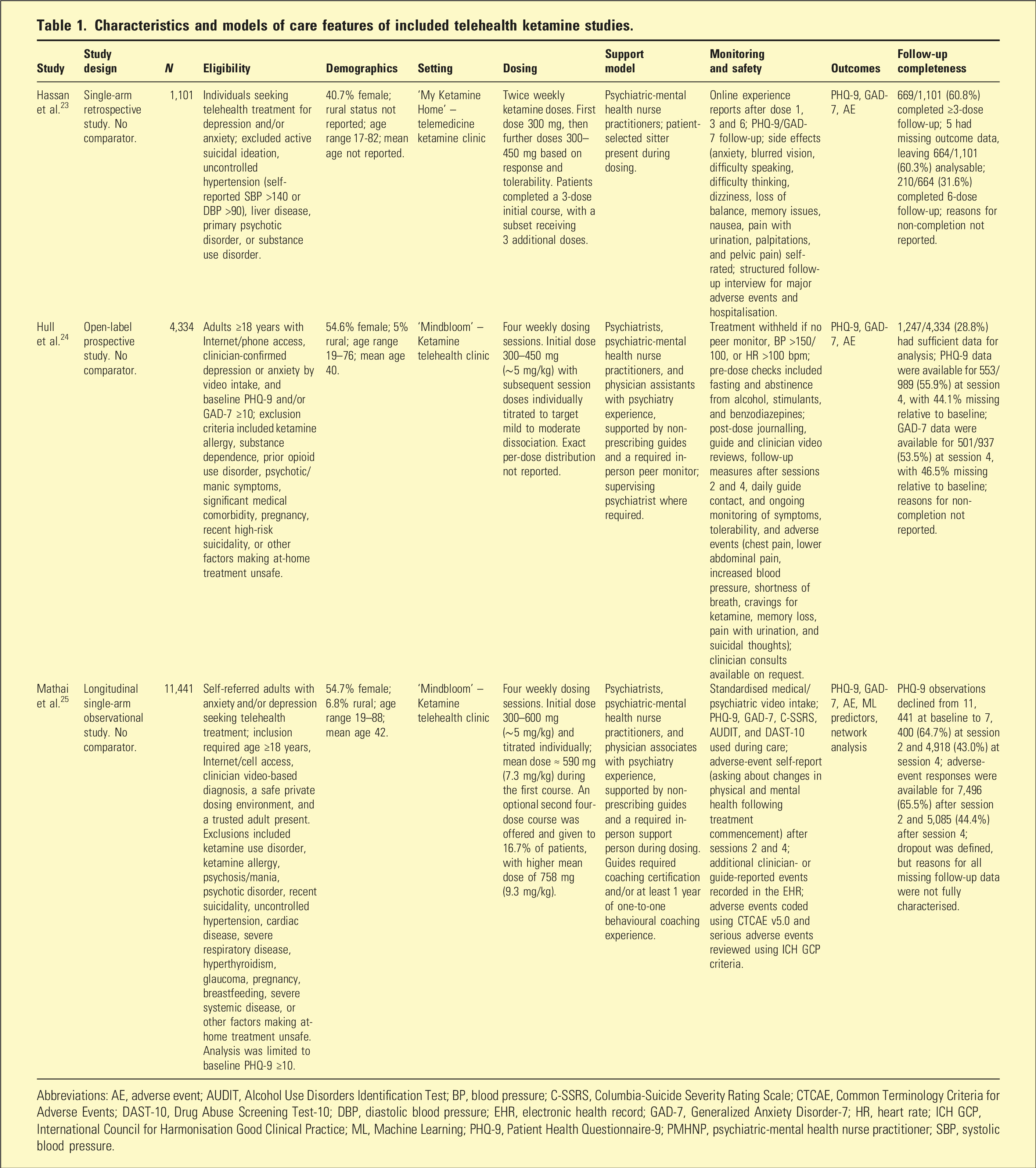
cohorts is possible and unique participant counts cannot be confirmed. PRISMA 2020 flow diagram of study selection. A total of 4,079 records were identified from five databases and one trial registry, with 222 duplicates removed prior to screening. Of the 3,857 records screened by title and abstract, 3,848 were excluded. Nine full-text reports were retrieved and assessed for eligibility. Out of these, six were excluded for the following reasons: wrong intervention (n = 1), ineligible study design or publication type (n = 2), wrong setting (n = 1), wrong indication and population (n = 1), protocol without reported results (n = 1). Adapted from Page et al. (2021) PRISMA 2020 statement: an updated guideline for reporting systematic reviews, BMJ 2021;372:n71, under the CC BY 4.0 licence. Characteristics and models of care features of included telehealth ketamine studies. Abbreviations: AE, adverse event; AUDIT, Alcohol Use Disorders Identification Test; BP, blood pressure; C-SSRS, Columbia-Suicide Severity Rating Scale; CTCAE, Common Terminology Criteria for Adverse Events; DAST-10, Drug Abuse Screening Test-10; DBP, diastolic blood pressure; EHR, electronic health record; GAD-7, Generalized Anxiety Disorder-7; HR, heart rate; ICH GCP, International Council for Harmonisation Good Clinical Practice; ML, Machine Learning; PHQ-9, Patient Health Questionnaire-9; PMHNP, psychiatric-mental health nurse practitioner; SBP, systolic blood pressure.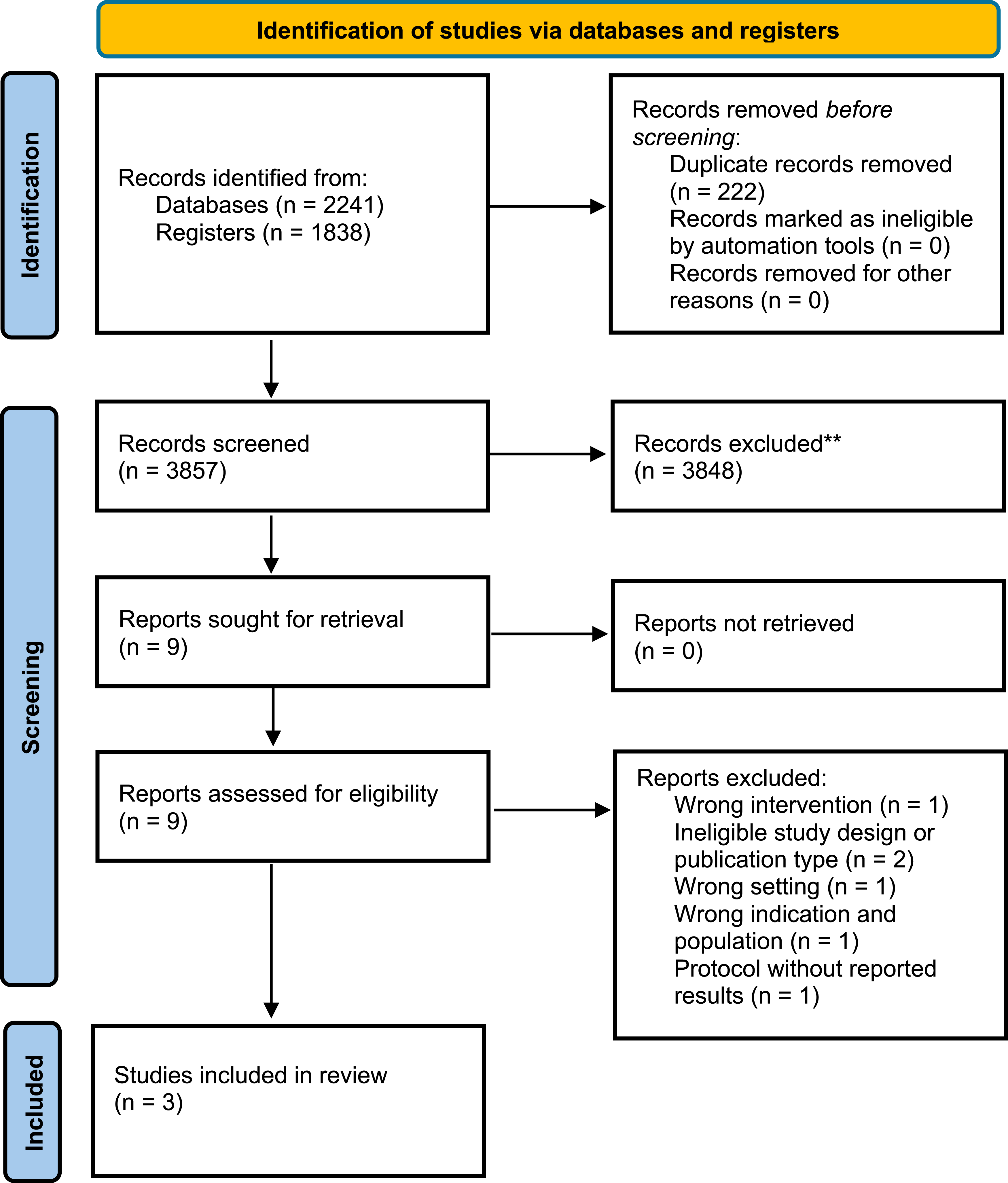
Programme characteristics and dosing regimens
Across the three studies, the telehealth models shared several core elements but differed in dosing strategies, workforce composition and monitoring structure, summarised in Table 1. Hassan et al. 23 examined patients who received twice-weekly doses over 2–3 weeks, with most patients completing either three or six sessions, starting at 300 mg and titrating up to a maximum of 450 mg. Hull et al. 24 and Mathai et al. 25 studied patients who were treated with a four-session protocol over 4 weeks. The Hull et al. 24 cohort received an initial dose of 300–450 mg and the Mathai et al. 25 cohort received an initial dose of 300–600 mg. Subsequent doses were individually titrated to achieve a target clinician-observed level of dissociation. An optional second four-dose course was offered in Mathai et al. 25
In Hassan et al. 23 psychiatric-mental health nurse practitioners prescribed ketamine and oversaw treatment. Patients were instructed to dose in the presence of a sitter and complete structured online follow-up reports. Hull et al. 24 and Mathai et al. 25 employed broader psychiatric prescriber networks, including psychiatrists, psychiatric-mental health nurse practitioners, and physician assistants or associates with psychiatry experience, supported by non-prescribing guides and a required in-person peer monitor during dosing. Monitoring intensity also differed. Hull et al. 24 described pre-dose physiological screening and ongoing guide-led follow-up, whereas Mathai et al. 25 reported a more structured safety framework. This incorporated validated symptom scales, adverse-event self-report, and additional clinician or guide-reported events recorded in electronic health records.
Efficacy of telehealth ketamine administration for depression and anxiety
Telehealth ketamine outcome on depression (PHQ-9) at primary follow-up.
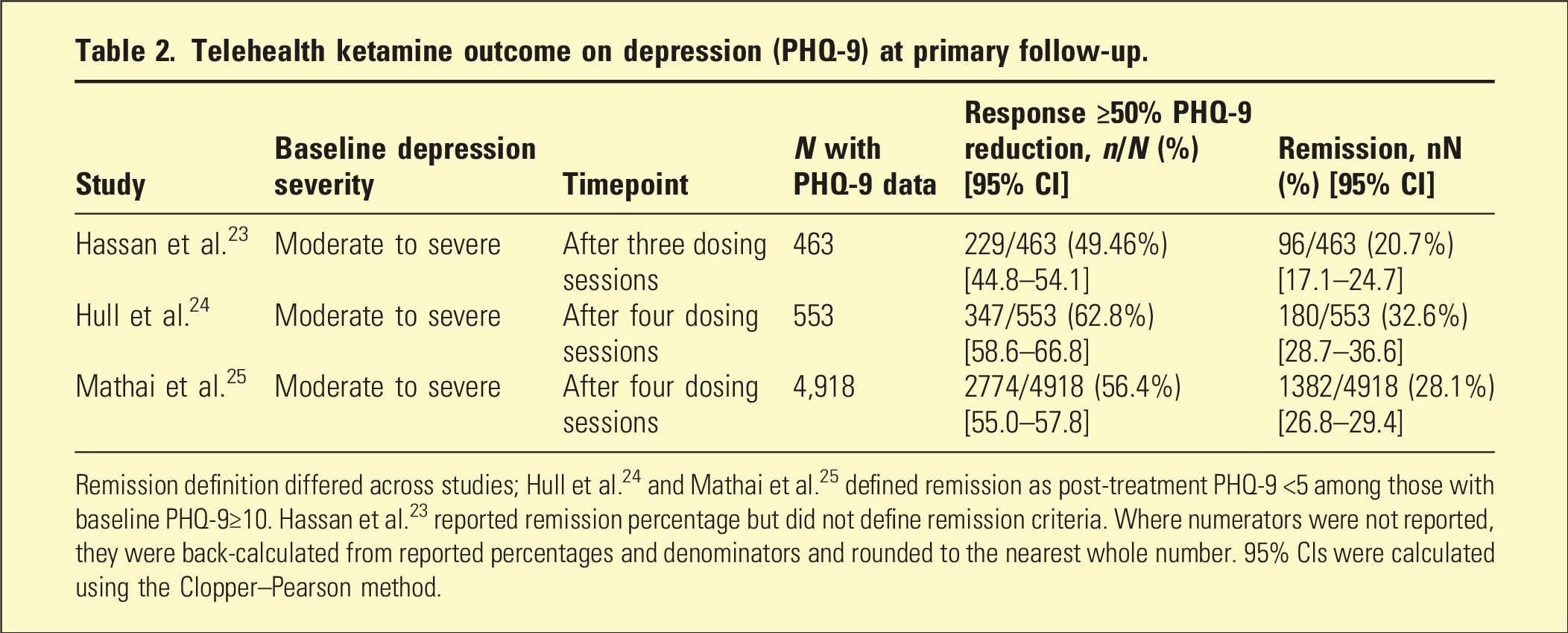
Remission definition differed across studies; Hull et al. 24 and Mathai et al. 25 defined remission as post-treatment PHQ-9 <5 among those with baseline PHQ-9≥10. Hassan et al. 23 reported remission percentage but did not define remission criteria. Where numerators were not reported, they were back-calculated from reported percentages and denominators and rounded to the nearest whole number. 95% CIs were calculated using the Clopper–Pearson method.
Telehealth ketamine outcome on anxiety (GAD-7) at primary follow-up.
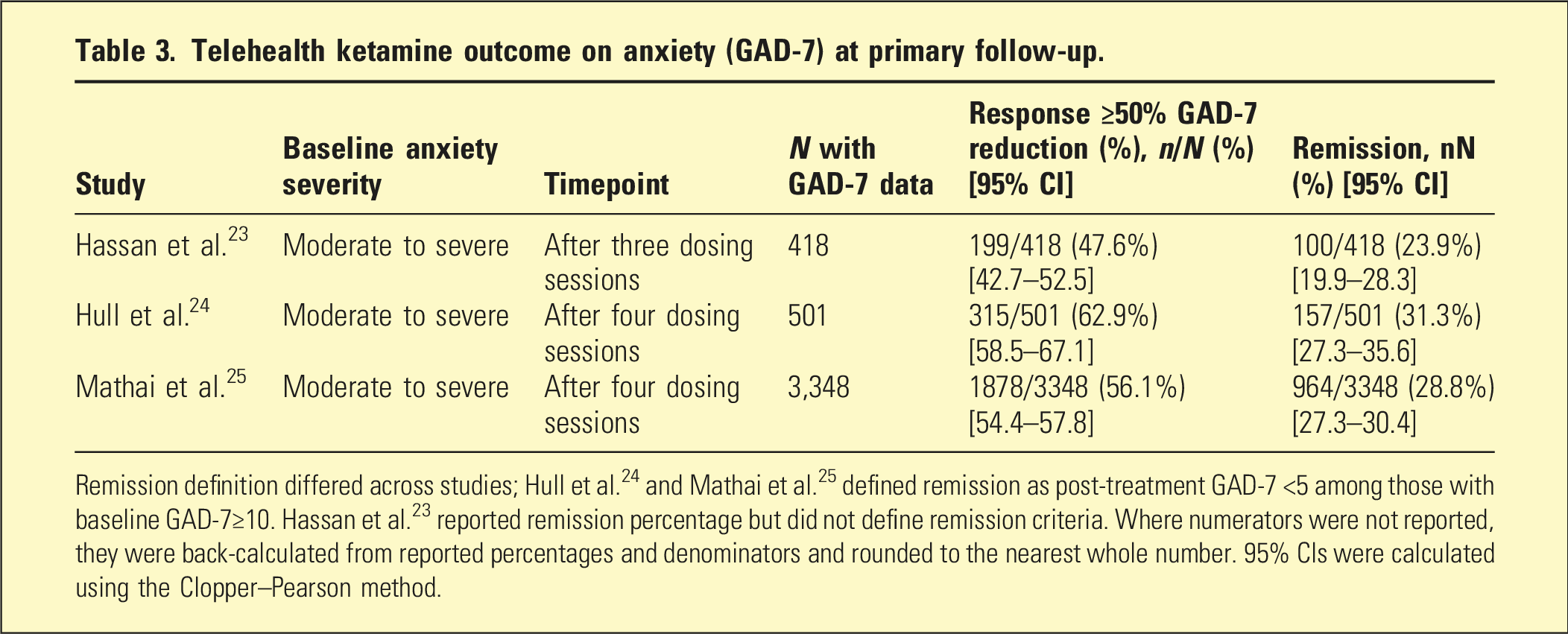
Remission definition differed across studies; Hull et al. 24 and Mathai et al. 25 defined remission as post-treatment GAD-7 <5 among those with baseline GAD-7≥10. Hassan et al. 23 reported remission percentage but did not define remission criteria. Where numerators were not reported, they were back-calculated from reported percentages and denominators and rounded to the nearest whole number. 95% CIs were calculated using the Clopper–Pearson method.
Anxiety outcomes showed a similar pattern (Table 3). Across cohorts, patients with at least moderate baseline anxiety displayed response rates (≥50% reduction in GAD-7) of 47.6 to 62.9% and remission rates of 23.9 to 31.3% on their post-treatment evaluation shortly after completing 3–4 ketamine dosing sessions.23–25 Outcomes were assessed at the end of the initial course, corresponding to approximately 2–4 weeks depending on programme schedule. Remission was defined as a baseline score of GAD-7≥10 and a post-treatment score of GAD-7<5 for Mathai et al. 25 and Hull et al. 24 Remission percentages were reported but not defined in Hassan et al 23 ; therefore, remission is not directly comparable across cohorts.
Safety and tolerability
Across 16,876 treated patients, telehealth ketamine was reported as generally well tolerated in the short-term. The most common adverse effects were dissociation, dizziness, nausea, and transient imbalance, usually rated as mild or moderate and resolving without medical intervention.23–25 Serious acute events during supervised dosing were rare. In the largest cohort, serious adverse events, such as severe depression, suicidal ideation, or psychosis, occurred in less than 0.05% (n = 6) of patients, and treatment discontinuation due to adverse events occurred in 0.4%. 25 However, adverse event data relied on patient self-reports and was limited to the treatment period duration.
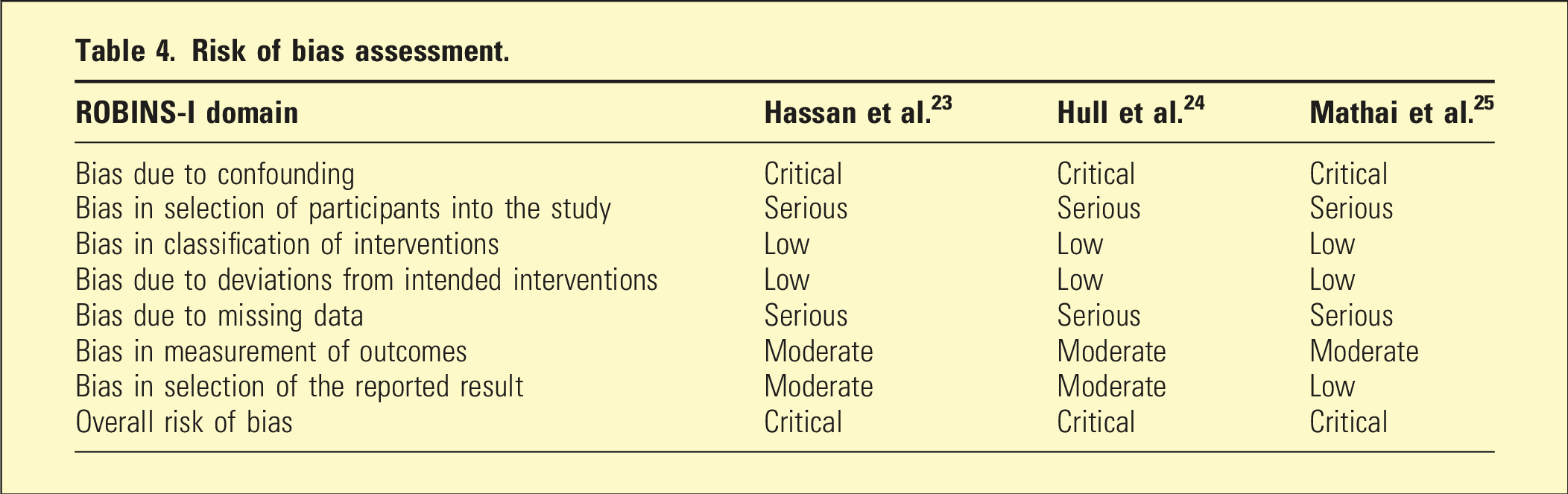
Risk of Bias
Risk of bias assessment.
GRADE Summary of Findings
GRADE summary of findings.
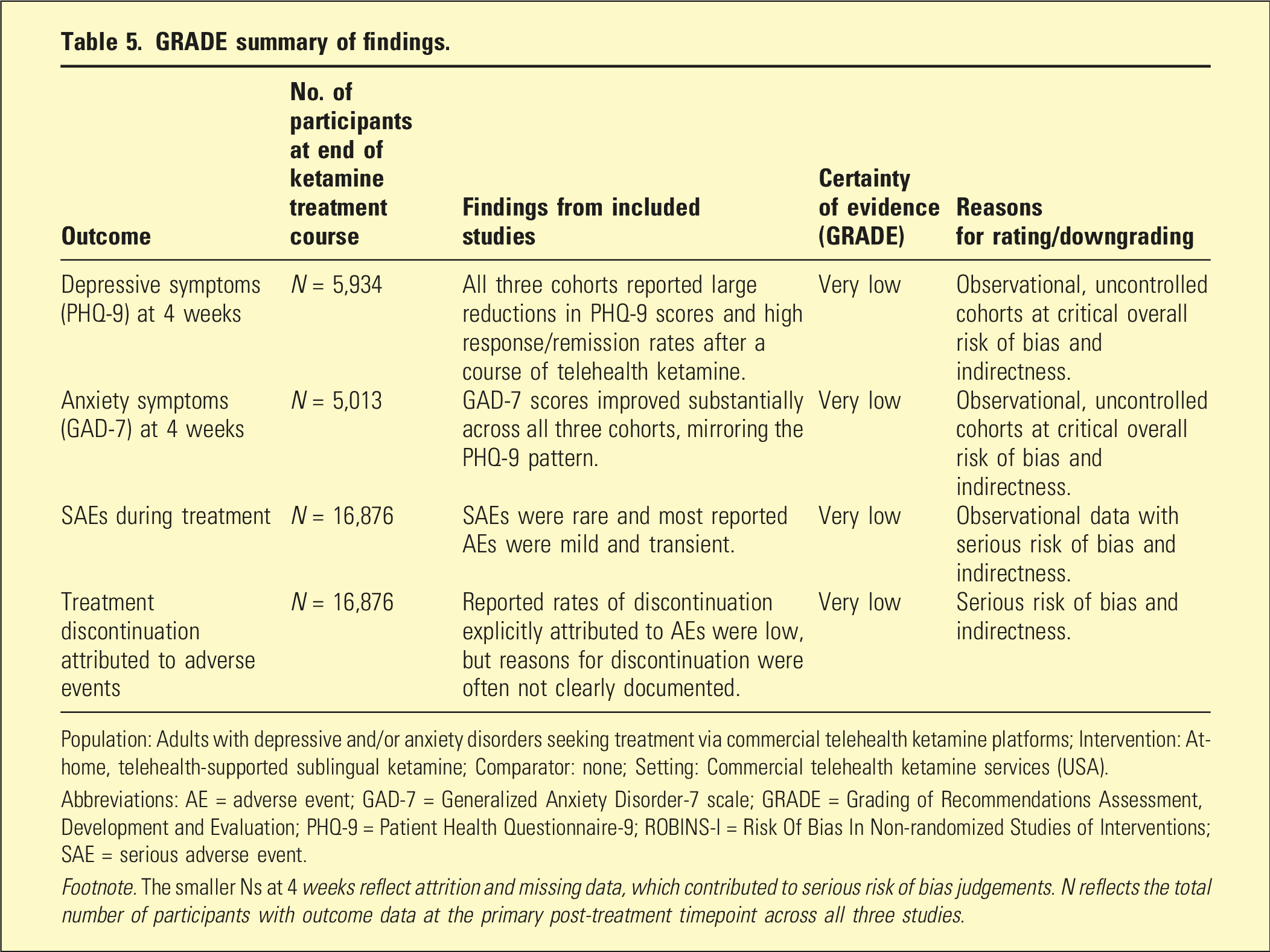
Population: Adults with depressive and/or anxiety disorders seeking treatment via commercial telehealth ketamine platforms; Intervention: At-home, telehealth-supported sublingual ketamine; Comparator: none; Setting: Commercial telehealth ketamine services (USA).
Abbreviations: AE = adverse event; GAD-7 = Generalized Anxiety Disorder-7 scale; GRADE = Grading of Recommendations Assessment, Development and Evaluation; PHQ-9 = Patient Health Questionnaire-9; ROBINS-I = Risk Of Bias In Non-randomized Studies of Interventions; SAE = serious adverse event.
Footnote. The smaller Ns at 4 weeks reflect attrition and missing data, which contributed to serious risk of bias judgements. N reflects the total number of participants with outcome data at the primary post-treatment timepoint across all three studies.
Discussion
This systematic review identified only three observational cohorts evaluating telehealth ketamine for depression and anxiety. Across 16,876 treated patients, provider-generated datasets reported large reductions in PHQ-9 and GAD-7 scores and response rates around 50–60%, with remission in roughly one quarter to one third of patients who chose to complete follow-up. Short-term tolerability was reported as favourable, with mostly mild and transient adverse effects and few serious acute complications during supervised dosing.
However, the certainty that these findings reflect a true causal benefit of telehealth ketamine is very low. All three studies were single-arm, non-randomised cohorts at critical overall risk of bias on ROBINS-I. Without any concurrent comparison group, the large improvements in PHQ-9 and GAD-7 scores cannot be disentangled from regression to the mean, spontaneous symptom fluctuation, study participation effects, placebo responses, or concurrent changes in other treatments. Participants were self-selected, treatment-seeking users of commercial telehealth platforms, and inclusion in analytic samples depended on completing a minimum number of doses and opting in to provide follow-up outcome data. Substantial attrition from baseline to post-treatment follow-up raises a high risk of bias from missing data, and none of the studies used analytical methods to explore the impact of non-completion. These issues underpinned our ROBINS-I judgements and GRADE ratings of very low certainty for both depression and anxiety outcomes.
Short-term safety data, although based on large cohorts, are also limited. Adverse events were ascertained via patient self-report and routine platform monitoring over a relatively brief time frame, focussing on events during dosing sessions and early follow-up. Under-ascertainment of adverse events is therefore likely, particularly for harms that emerge after treatment or outside the service’s awareness. Reasons for treatment discontinuation were not consistently separated into adverse-event-related versus efficacy, financial, or logistical factors, making it difficult to estimate true discontinuation rates due to tolerability. Hence, we judged the certainty of evidence for safety outcomes to be very low.
When mapped against Australasian guidance on ketamine use in psychiatric practice, the telehealth models reviewed here raise questions regarding supervision intensity, monitoring, documentation, and risk mitigation. Regulatory communications and case reports raise additional safety concerns not captured in cohort studies.17,26–28 In Australia, only intranasal esketamine has regulatory approval for treatment-resistant depression. Its use is governed by Therapeutic Goods Administration conditions and an associated Risk Management Plan, which mandate in-person administration under direct healthcare professional supervision in a clinical setting, with post-dose monitoring. 6 In Australia, intranasal esketamine can only be prescribed by psychiatrists accredited by the manufacturer, who must complete training in esketamine prescribing and administer it in accredited facilities. In addition, guidance from the Royal Australian and New Zealand College of Psychiatrists provides further practice recommendations including, careful patient selection, governance structures, and monitoring standards for ketamine use in psychiatric practice.8,10,29
Australian regulators and professional bodies have also highlighted patient-safety risks in evolving commercial telehealth prescribing models, 30 including medicinal cannabis 31 and stimulant prescribing for ADHD. 32 Regulatory and disciplinary action regarding ketamine prescribing has also been reported in Australia, reinforcing the governance and monitoring requirements that constrain ‘take-home’ ketamine in psychiatric practice. 33 For this reason, the relevance of these at-home models to current Australian psychiatric practice is primarily conceptual rather than practice-changing.
The included studies provide a preliminary view of how telehealth-supported ketamine clinics are operationalised in practice. All three programmes used structured screening, multi-session treatment courses, and some form of remote follow-up, but they differed in workforce composition, supervision intensity, and safety monitoring. Hassan et al. 23 used a psychiatric-mental health nurse practitioner-led model with sitter-supported dosing and online follow-up reports. Hull et al. 24 and Mathai et al. 25 used broader psychiatric prescriber networks supported by non-prescribing guides and a required in-person peer monitor, with greater emphasis on preparation and integration support. Among these, Mathai et al. 25 described the most formalised safety framework, including structured symptom and safety instruments, explicit adverse-event capture, and standardised adverse-event coding.
Across the three programmes, strengths of the telehealth models included the potential to improve access to care, reduce in-person treatment burden, and support scalable delivery. Their main limitations included the potential for delayed recognition of adverse events, limited control over the dosing environment, fragmented continuity of care, and reliance on self-report, non-clinical supports, and non-psychiatrist prescribers.23–25 As such, the most transferable contribution of the current literature may be the identification of service components that could inform a future hybrid model, rather than the estimation of treatment efficacy. Potential future adaptation in the Australian context would likely require more stringent eligibility criteria, psychiatrist-led governance, clearer escalation pathways, and more structured physiological and adverse-event monitoring than those described in the current US telehealth models. Any hybrid model would also need to be developed within Australian regulatory requirements. Any expansion of ketamine service models in Australia should also be considered through an equity lens, including access for rural and remote communities and culturally safe care for Aboriginal and Torres Strait Islander peoples.
A distinctive feature of the articles included in the analysis is their tight coupling between intervention, data source, and investigators. All three cohorts analysed data generated by commercial providers, and several authors were employees, consultants, founders, or otherwise professionally or financially linked to these companies. In some instances, the service itself appears to have been responsible for data collection, analysis, and/or manuscript preparation. Such alignment introduces a high risk of conflicts of interest and industry-sponsored bias, further reducing confidence that published results present a balanced picture of benefits and harms. Clinicians and policymakers should therefore interpret existing data with caution. Future research should prioritise independently funded, prospectively registered studies with appropriate comparators and robust methods to mitigate bias. Pragmatic randomised trials and longer-term follow-up are needed to clarify the true benefits, durability of response, and spectrum of harms associated with telehealth-supported at-home ketamine.
This review also has methodological limitations. The protocol was not prospectively registered. Screening and data extraction were undertaken by one reviewer with verification by a second, rather than full independent duplicate processes. All included cohorts were drawn from US commercial telehealth services using sublingual racemic ketamine, which limits generalisability to other formulations, service models, and Australasian health systems. As a result, our findings should be interpreted as an early, low-certainty synthesis rather than a definitive evaluation of telehealth ketamine.
Conclusion
Our systematic review suggests that telehealth at-home sublingual racemic ketamine is reported to be associated with substantial short-term improvements in depressive and anxiety symptoms in highly selected, commercially treated populations in the US. It also suggests that serious acute adverse events during supervised dosing appear uncommon in these settings. Nevertheless, the evidence is characterised by critical risk of bias, substantial conflicts of interest, and limited generalisability, leading to very low certainty for effectiveness and safety. With intranasal esketamine approved in Australia and subsidised under the PBS for treatment-resistant depression, high-quality, independently conducted research is required before this model of care can be considered an evidence-based treatment for depression and anxiety within the Australasian context. At present, the most useful contribution of this literature may be in identifying telehealth service-model components and implementation considerations, rather than providing reliable estimates of treatment efficacy.
Supplemental material
Supplemental material - Telehealth-supported ketamine for depression and anxiety: A systematic review
Supplemental material for Telehealth-supported ketamine for depression and anxiety: A systematic review by Eden Mane and Saras Mane in Australasian Psychiatry
Footnotes
Author contributions
Concept design – EM and SM; Search and screening – EM and SM; Data extraction – EM and SM; Risk of Bias and GRADE – EM; Drafting – EM.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data were extracted from published studies. No new datasets were generated and no analytic code was used.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.