
Abstract
Objective
This paper considers early colonial Australian incarceration as a diffuse carceral system encompassing gaols, private dwellings and sites of labour rather than discrete institutional forms. Drawing on existing records and historiography, this paper examines the nature of incarceration practices in early colonial Australia prior to the advent of the asylum.
Conclusions
Confinement operated across multiple sites, including gaols, assigned labour settings and private households, where authority was exercised through overlapping legal, medical and domestic arrangements. These were not discrete institutional responses but part of a loosely coordinated system in which surveillance and discipline were embedded in everyday colonial life. This analysis highlights how practices of punishment and care developed in tandem, circulating across sites rather than emerging solely within formal institutions. In doing so, it situates early incarceration within broader dynamics of colonial governance and social regulation.
This analysis contributes to psychiatric history by illustrating how early Australian asylums emerged from institutions with penal practices, confirming care narratives and underscoring the enduring entanglement of care and control.
Early colonial Australia did not begin with prisons and asylums as discrete institutions, but with a dispersed and improvised system of confinement. Convicts, vagrants and the mentally ill were managed through overlapping regimes of confinement prior to the formal establishment of colonial asylums. Early practices in New South Wales and Van Diemen’s Land demonstrate that those deemed “lunatic” along with the non-productive aged and physically disabled were routinely held in gaols, chain gangs and makeshift hospital wards, reflecting administrative pragmatism rather than psychiatric differentiation.1,2
The emergence of purpose-built asylums in the mid-19th century is situated within broader colonial governance, moral regulation and the transplantation of British medico-legal frameworks. Developments such as Tarban Creek Lunatic Asylum illustrate the gradual consolidation of psychiatric classification alongside state authority. Contemporary scholarship suggests these institutions functioned less as therapeutic environments, with the intention to treat using moral treatment, than as mechanisms of social ordering. 1
Accounts of psychiatric and penal history in Australia often begin with the prison and the asylum as if these were the foundational sites of confinement.2,3 Such accounts risk imposing institutional clarity on a context that was, in its early decades, anything but orderly. Prior to the establishment of purpose-built asylums and formalised prison systems, colonial Australia was already deeply carceral reflecting British contemporary approaches to managing crime and mental illness. 1
Early colonial confinement operated as a diffuse system of carcerality, distributed across multiple sites and practices rather than contained within discrete institutions. Convicts, petty offenders and individuals described as “lunatics” were managed within overlapping regimes of control in which distinctions between criminality, disorder and mental illness were unstable and often irrelevant in practice. 4
This study hypothesises that the emergence of asylums in the mid-19th century did not mark the beginning of psychiatric care but rather represented the consolidation of existing practices shaped by colonial governance, moral regulation and proto-psychiatric classification. Situating these developments within their British imperial context, Figure 1 demonstrates how inherited models of confinement were adapted to the conditions for both Australian penal colonies and free settler states. Diffuse carcerality.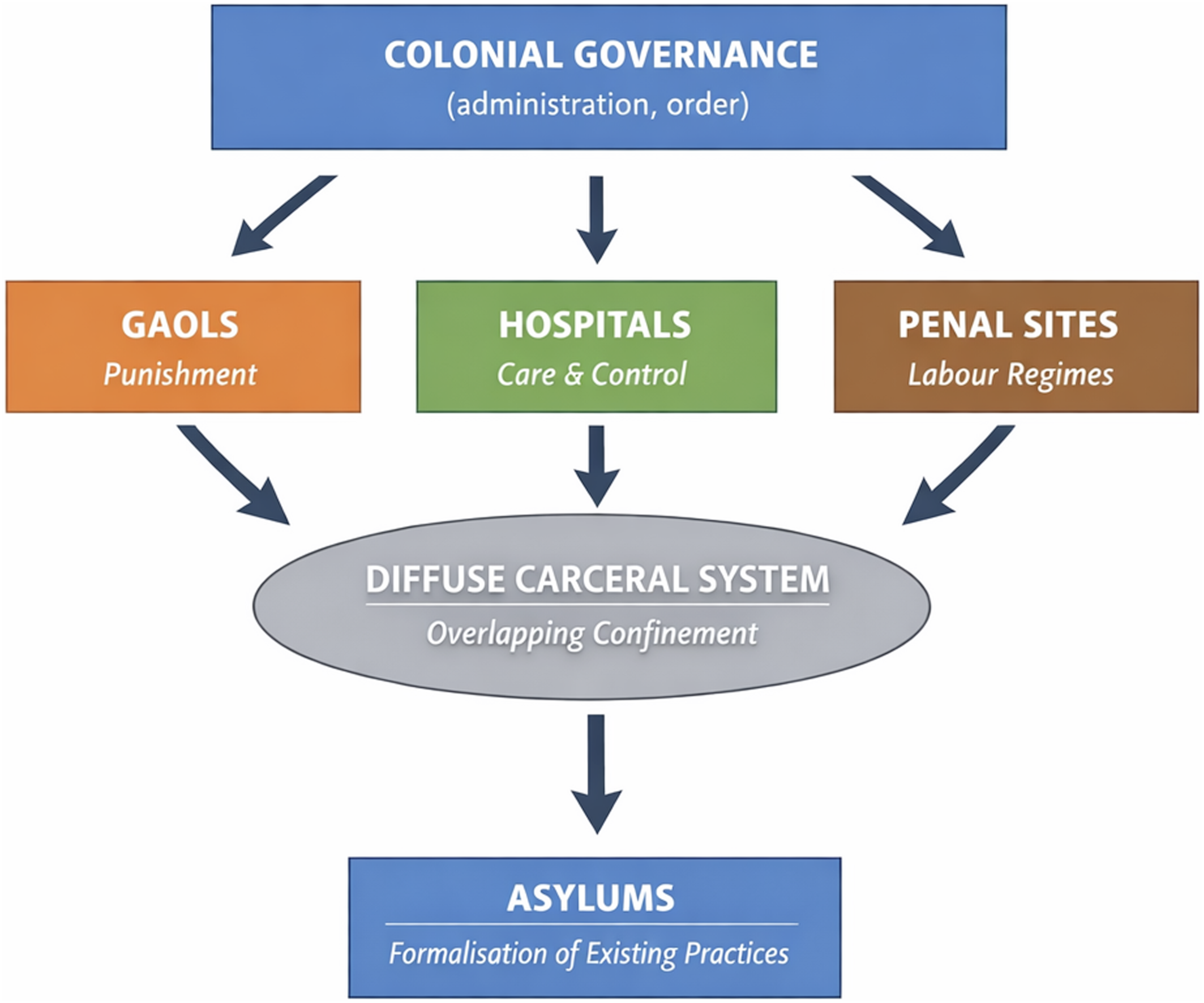
Carceral beginnings in the Australian colonies
In the early decades of the New South Wales colony, confinement was not anchored to a single institutional form. Instead, it operated across a network of sites including military guardhouses, makeshift lockups, convict huts, chain gangs and, later, barracks. 2 Punishment was primarily organised through labour allocation and physical discipline rather than long-term incarceration. 3
Archival evidence supports this dispersed model of care. Correspondence from the Colonial Secretary indicates that individuals labelled as disorderly or insane were frequently confined in local gaols or managed within private dwellings due to the absence of dedicated facilities. 4 Hospital records from Sydney likewise show patients described as “lunatic” admitted alongside the sick and injured, often under restraint. 5 In a developing colony, custodial priorities meant that provision for gaols outstripped that for the care of the mentally ill.
The 1822 report of John Thomas Bigge (1780–1843), commissioned under Lord Bathurst to review the administration of Lachlan Macquarie, reinforces that custodial priorities prevailed. Bigge noted the routine use of gaols and other improvised spaces to manage those considered disruptive or unproductive within the colony. 6 Together, these sources point to a system in which confinement was pragmatic and situational rather than formally institutionalised.
Early carceral and asylum institutions in the Australian colonies
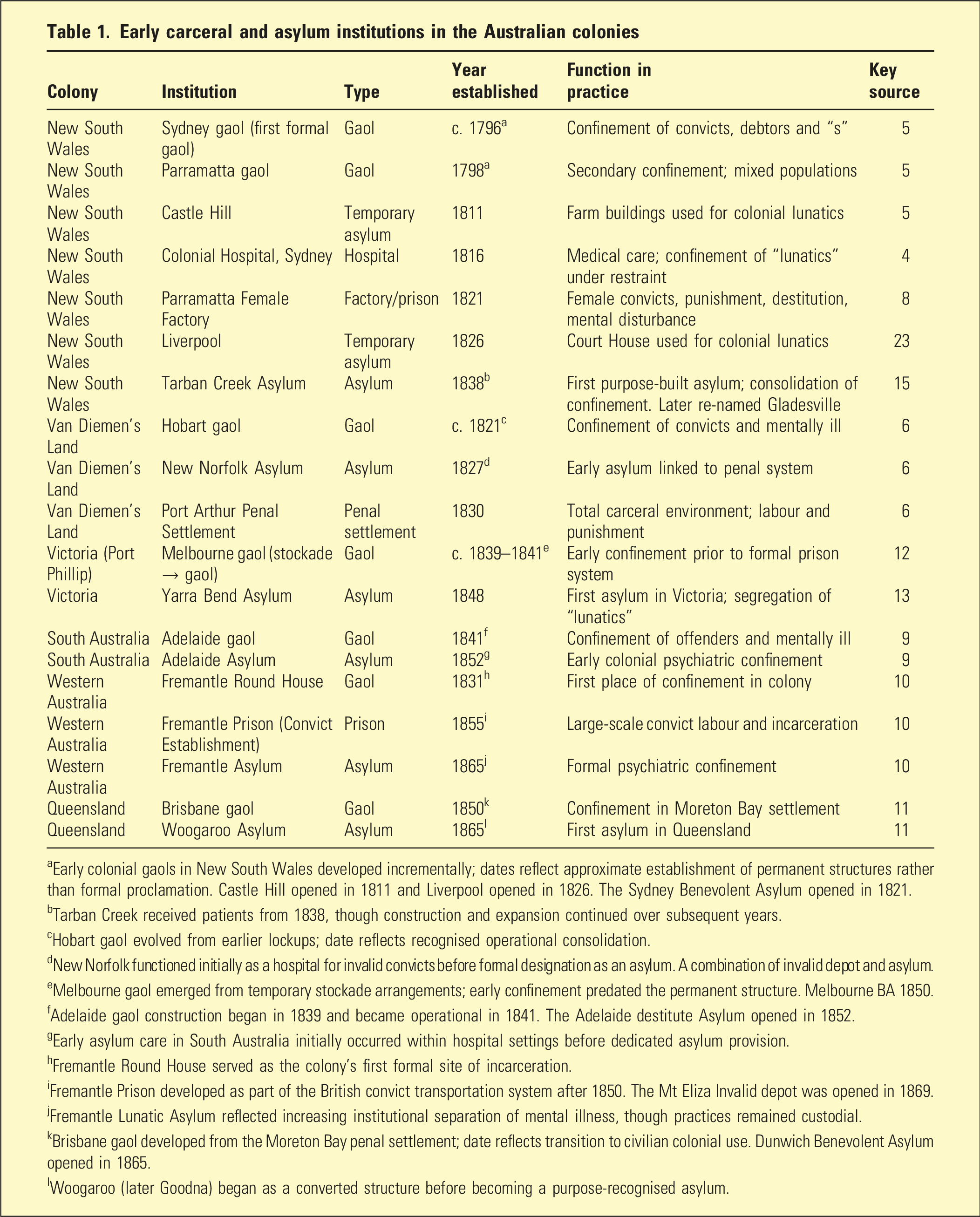
aEarly colonial gaols in New South Wales developed incrementally; dates reflect approximate establishment of permanent structures rather than formal proclamation. Castle Hill opened in 1811 and Liverpool opened in 1826. The Sydney Benevolent Asylum opened in 1821.
bTarban Creek received patients from 1838, though construction and expansion continued over subsequent years.
cHobart gaol evolved from earlier lockups; date reflects recognised operational consolidation.
dNew Norfolk functioned initially as a hospital for invalid convicts before formal designation as an asylum. A combination of invalid depot and asylum.
eMelbourne gaol emerged from temporary stockade arrangements; early confinement predated the permanent structure. Melbourne BA 1850.
fAdelaide gaol construction began in 1839 and became operational in 1841. The Adelaide destitute Asylum opened in 1852.
gEarly asylum care in South Australia initially occurred within hospital settings before dedicated asylum provision.
hFremantle Round House served as the colony’s first formal site of incarceration.
iFremantle Prison developed as part of the British convict transportation system after 1850. The Mt Eliza Invalid depot was opened in 1869.
jFremantle Lunatic Asylum reflected increasing institutional separation of mental illness, though practices remained custodial.
kBrisbane gaol developed from the Moreton Bay penal settlement; date reflects transition to civilian colonial use. Dunwich Benevolent Asylum opened in 1865.
lWoogaroo (later Goodna) began as a converted structure before becoming a purpose-recognised asylum.
Managing “lunatics” before asylums
In the Australian colonies, before the establishment of formal asylums, individuals deemed mentally ill were managed within existing colonial infrastructures. Existing structures were appropriated and functioned as sites of containment, with little differentiation between categories of confinement. 7
For example, in the Swan River colony, the first approaches to managing the mentally ill occurred outside formal institutions. A disused barge, prison structures such as the Round House and temporary shelters like Scott’s Warehouse were repurposed to confine people assessed as mentally ill alongside convicts and other inmates, illustrating the lack of institutional differentiation in early colonial practice. 8
This lack of distinction was not simply a consequence of limited resources but also of conceptual ambiguity. “Madness” was not yet identified as a medical category distinct from criminality or moral disorder. Behaviour that disrupted social order, whether interpreted as insanity, intoxication or insubordination, was subject to similar forms of control. 7
The Parramatta Female Factory illustrates this overlap. Established as a site for housing and employing female convicts, it also functioned as a place of confinement for women deemed disorderly, destitute or mentally unstable. 9 In this context, categories of gender, morality and mental state intersected, reinforcing the fluidity of classification within colonial governance. 7
Evidence from early hospital and gaol records suggests that restraint, seclusion and labour were common responses to those labelled “lunatic,” mirroring the treatment of other confined populations. 10
British models and colonial adaptation
The diffuse carceral practices observed in colonial Australia reflect the transplantation and adaptation of British systems of confinement. In Britain, the management of the poor, the criminal and the insane occurred across a range of overlapping institutions, including gaols, workhouses and private madhouses. 11
These institutions were not clearly differentiated in function. Workhouses confined the idle and destitute, gaols held a heterogeneous population including debtors and minor offenders, and “madhouses” operated as custodial spaces with attempts to use therapeutic approaches incorporating moral treatment, which emphasised character and spiritual development. 12
While colonial administrators drew on British institutional models, they adapted them to local conditions, most notably using benevolent societies rather than the workhouse system. 7 Australian benevolent asylums often acted as the primary, albeit unofficial, poor relief institutions and were characterised by similar stigmas and harsh conditions. The absence of established infrastructure, combined with the demands of a penal colony, necessitated flexibility. Confinement could occur wherever space and authority allowed, producing a system that was both more visible and fluid.12,13
Recent scholarship emphasises how colonial governance relied on such flexibility to manage populations characterised by mobility and perceived disorder.13–15 Rather than building institutions for the mentally ill first and then filling them, colonial authorities worked with available spaces, gradually formalising practices that were already in operation.
In Victoria, Collingwood stockade, built in 1853, is an example of a makeshift prison with inmates used to mine a local quarry. In 1866, the stockade became an asylum and first housed the mentally ill from other jails. 16
The emergence of the asylum
The establishment of purpose-built asylums from the late 1830s, including the first asylum at Tarban Creek in New South Wales, marked an important administrative development but not a fundamental conceptual shift. 17 Legislation in the colonies to manage the mentally ill was established in NSW with the Dangerous Lunatics Act of 1843 (covering NSW, Queensland and Tasmania as part of the then NSW colony), South Australia Lunatics Act 1864 and the Western Australia Lunacy Act 1871.
Asylums introduced new forms of classification, record-keeping and spatial organisation, distinguishing patients from prisoners in increasingly formal ways. However, these institutions retained many features of earlier carceral systems, including confinement, surveillance and regimented routine. 17
Archival sources indicate that transfers between gaols and asylums were common, and that decisions regarding placement were often administrative triage to house the mentally ill in gaols until beds in the asylum could be found. 7 This suggests that the boundary between criminality and insanity remained porous despite the emergence of specialised institutions.
Contemporary historiography has reinforced this interpretation, arguing that colonial asylums functioned as mechanisms of social regulation as much as sites of treatment.18–20 The asylum, in this sense, did not replace carcerality but reorganised it within a more formalised institutional framework.
The appointment of medical officers to oversee the “insane” in colonial Australia marked a shift from ad hoc carceral confinement toward purpose-built asylums, though this transition remained uneven and fiscally contested. In New South Wales, the arrival of Frederick Norton Manning (1839–1903) in the 1860s to become Inspector General of the Insane for the colony of NSW coincided with growing advocacy for specialised institutions grounded in therapeutic care, classification and moral management. 4 These arguments, reflecting broader British reforms, associated with John Conolly (1794–1866). Conolly, resident physician for Middlesex County Asylum and a key figure in British lunacy reform, advanced the non-restraint movement and the principles of moral management within asylums. 21
However, government investment was cautious, with building programs delayed or adapted due to financial constraints and competing priorities. Persistent shortages of trained attendants further limited implementation, as reports stressed that without adequate staffing, the therapeutic aims of asylums could not be realised. Consequently, expansion was gradual and uneven, shaped as much by labour and administrative capacity as by medical advocacy, and hybrid carceral practices persisted into the late nineteenth century.21–24
Studies of the Fremantle Lunatic Asylum reveal that the appointment and training of attendants were essential to its operation, with recruitment difficulties shaping both the pace of expansion and the costs of securing purpose-built facilities, indicating that labour constraints, as much as architectural planning or medical advocacy, influenced asylum development.25,26
Discussion
Understanding early colonial confinement as a diffuse carceral system has important implications for psychiatric history. I purport that, rather than marking the origin of organised responses to mental illness, the asylum should be understood as one element within a broader field of governance and control shaping the emergence of psychiatry. The evidence presented here demonstrates that individuals labelled as mentally ill were initially managed within the same systems used to control convicts and other marginal populations. 21 The later differentiation of these groups reflects administrative and conceptual developments rather than a wholesale transformation of practice. 18
This perspective aligns with contemporary work in carceral geography and the history of psychiatry, which emphasises the networked and expansive nature of confinement.26,27 It also highlights the enduring entanglement of care and control within mental health systems, a dynamic that continues to shape contemporary practice.
Conclusion
Early colonial Australia was characterised by a form of carcerality that preceded and exceeded the prison and the asylum. Confinement operated across a dispersed network of sites and practices, encompassing convicts, offenders and individuals deemed mentally ill within a shared system of regulation.
The appointment of medical staff in key supervisory roles resulted in an informed campaign for purpose-built housing for the mentally ill and to recruit attendants and nurses to provide care.25,26 The emergence of asylums did not mark a clear break from these practices but rather consolidated and formalised them. Recognising this continuity provides a more nuanced understanding of the historical relationship between punishment, psychiatry and governance in Australia.
Footnotes
Acknowledgement
Open access publishing facilitated by La Trobe University, as part of the Sage – La Trobe University agreement via the Council of Australian University Librarians (CAUL).
Ethics considerations
As this was a historical paper using archival and published sources, approval by a Human Ethics committee was not required.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
No data was collected or available to share for this historical paper.