
Abstract
Purpose
To provide a representative Australian sample of ADHD assessment information available to consumers prior to booking an appointment, psychologists, psychiatrists, and paediatricians (N = 736) were contacted through a secret shopper design. Assessment information included the types of measures, the number of measures, the use of multiple informants, and the number of sessions required for adult and child assessments.
Major Findings
56% of providers declined to provide information about assessment content before booking an appointment. Psychologists provided information at a higher rate than psychiatrists and paediatricians. The majority of providers did not indicate the use of multiple informants (76.8% of psychologists and 100% of psychiatrists for adult assessments; 53.2% of psychologists, 85.7% of psychiatrists, and 50% of paediatricians for child assessments).
Conclusions
These findings demonstrate a lack of readily available information to consumers prior to booking ADHD assessments, limiting the consumer’s ability to anticipate if best-practice methods would be used.
Introduction
Attention Deficit Hyperactivity Disorder (ADHD) costs the Australian health system approximately $814.5 million per year, with 80% of this cost covered by the Australian government. 1 Despite this significant investment, there are no standardised processes or tools required for ADHD assessment.2,3 Considering potential variations in practices, significant impacts of assessment processes on diagnostic outcomes 4 and wellbeing,5–7 and high costs of assessments, 8 determining if consumers are being provided with sufficient information to make informed choices is essential.
No previous studies have addressed the availability of ADHD assessment information to prospective consumers in Australia. While guidelines recommend a combination of interviews, questionnaires, and multiple informants as key components of a quality ADHD diagnosis, 3 the lack of requirements has led to significant variation in practice.9–11 Without information about assessment practices, consumers are unable to determine if best-practice methods would be used, making it difficult to choose an appropriate provider.
While the three main practitioner types assessing for ADHD in Australia are psychologists, psychiatrists, and paediatricians,1,2,12 new reforms are allowing specifically trained general practitioners to diagnose ADHD. 13 Considering this change, assessing the management of information given to clients by those already in routine practice may provide an opportunity to inform the training and policy in this area going forward.
The current study aimed to address the gap in the literature and provide a national representative sample of the information available to consumers prior to booking ADHD assessments across psychologists, psychiatrists, and paediatricians for both adult and child assessments. Information provided during secret shopper phone calls regarding assessment content was investigated, including the types of measures, the number of measures, the use of multiple informants, and the number of sessions required.
Methods
Sample
To determine the appropriate number and distribution of calls, the amount of each clinician type (psychologist, psychiatrist, and paediatrician) registered or estimated in each state or territory across remoteness categories was gathered.14,15 Based on workforce proportion data and previous research, 8 a total sample of 736 clinicians were called, including 444 psychologists, 164 psychiatrists, and 128 paediatricians.
The Australian Bureau of Statistics’ 16 Postal Areas 2021 and Remoteness Areas 2021 Shapefiles were joined using the Geopandas Python library 17 to allow the classification of postcodes by remoteness categories (Major City, Inner Regional, Outer Regional, Remote, and Very Remote). Clinician density and remoteness data were then mapped proportionally to determine the appropriate sample size of calls for each category (clinician type, state, remoteness).
Listed psychologists, psychiatrists, and paediatricians on publicly available directory sites and online Google searches were used to develop a representative sample of phone numbers for contact (Yellow Pages = 439; HealthShare = 105; Australasian Society for Developmental Paediatrics = 74; Your Health In Mind = 62; Australian Psychological Society = 40; Google = 12; Healthengine = 4). Searches were conducted using ‘clinician type’ + ‘ADHD’ and refined by state and postcode for remoteness. Prior to data collection, duplicate phone numbers were removed, and disconnected numbers were replaced to maintain the clinician type and remoteness distribution. While clinicians were included based on their listed practice location, during calls they were not asked if they also provided online assessment services.
Data collection
Secret shopper studies involve researchers posing as consumers to gain information about a service from a consumer perspective, without the service’s knowledge that they are being involved in research. 18 This allows for the gathering of realistic, unbiased information, as in healthcare settings discrepancies have been observed between provider-reports and actual service.19,20
Following advised methodological procedures, 18 two researchers (CO & JF) utilised written scripts and standardised responses during telephone calls to services posing as a parent seeking an assessment for themselves and/or their child. Those answering calls included both clinicians and administrative staff, though this was not directly asked or recorded as this unusual question from a potential consumer may have raised suspicion. Clinicians and administrative staff are referred to as respondents, or providers if an ADHD assessment was available. Reference to specific clinician types is indicative of the clinician listed for contact, regardless of direct clinician or administrative contact.
Respondents were first asked if they provided ADHD assessments, before being asked what age groups they would assess to determine which of two vignettes would be used. The vignettes involved the parent, and/or their child, a 7-year-old boy with suspected ADHD. A general question was posed regarding assessment content (What is involved in the assessment?), with prompts for use of multiple informants and specific measures utilised if not yet provided (Will I/they need to complete any questionnaires or tests? Do we need reports from anyone else?). Separate data was collected for adults and children when services provided assessments for both. If asked to provide a referral, respondents were told that one would be completed before the assessment was scheduled. If details were requested, basic demographic information (i.e. name and date of birth) was provided. If more information was requested, the researchers deferred from answering stating they were not yet ready to book an appointment. If an appointment was offered, researchers deferred from accepting, stating they would call back if needed. No appointments were scheduled.
A mobile phone with no caller identification was used to make calls, so that the researcher’s area code was not visible. Voicemail messages were not left, and email or booking portals were not utilised to maintain researcher anonymity. Calls were made between the 10th of May 2024 and the 9th of August 2024, on weekdays between 8 am and 5 pm. A maximum of two calls were made to each service, on different days. If the call was not answered, but information about availability was provided (e.g. answering machine stating open days/times), this was noted, and second calls were made within these times.
Additional data including clinician availability, wait times, first session cost, and total assessment cost were also collected, and are reported elsewhere. 21
Statistical analysis
Statistical analyses were conducted using JASP 0.19.3. 22 Levene’s statistic was utilised to test the assumption of homogeneity of variance where appropriate. The Shapiro-Wilk test of normality was utilised to test the assumption of normality, and non-parametric tests were used for analyses if this was violated. For all initial analyses α = 0.05. Bonferroni adjustments were applied within each family of related comparisons (i.e. post-hoc analyses) to control the family-wise error rate.
Ethics approval
The research protocol was approved by the University of Wollongong Research Ethics Committee (Protocol number 2023/256).
Results
Sample
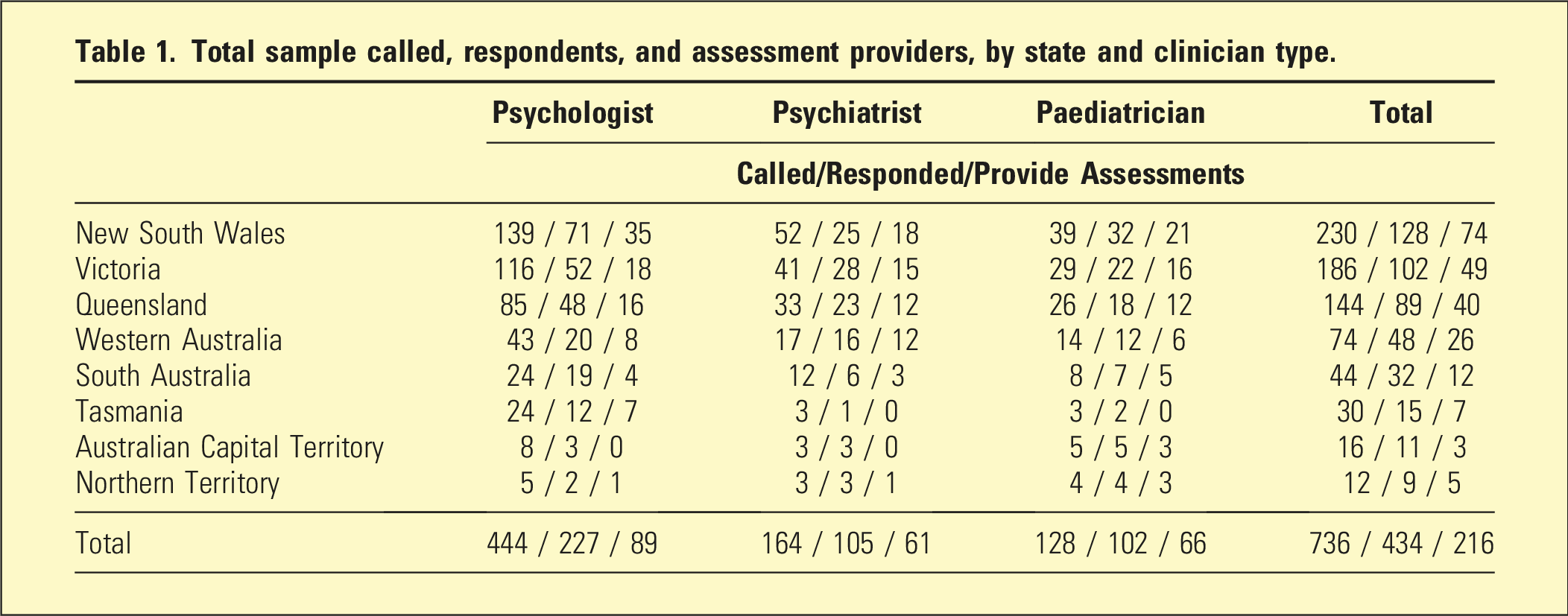
Total sample called, respondents, and assessment providers, by state and clinician type.
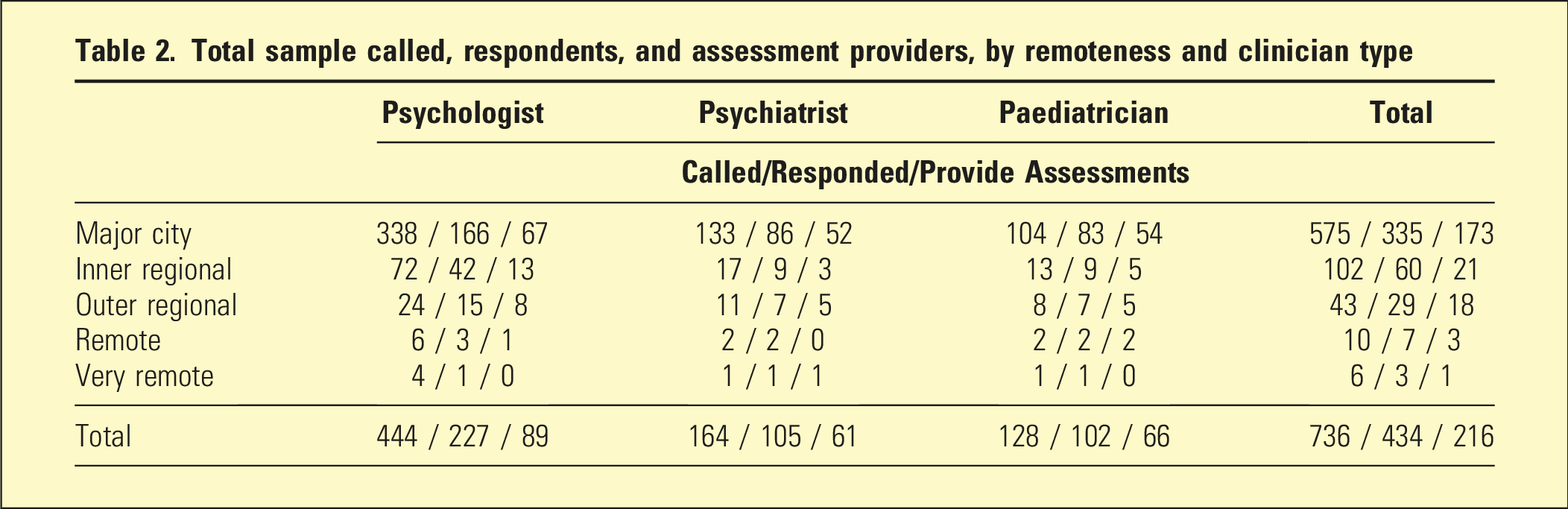
Total sample called, respondents, and assessment providers, by remoteness and clinician type
A Pearson’s chi-square test of contingencies compared the response rates between clinician types. The result was statistically significant (χ2 (2, n = 736) = 35.728, p < .001, Cramer’s V = 0.220), demonstrating that paediatricians responded at higher-than-expected rates, and psychologists at lower-than-expected rates.
Assessment content
Across ages and clinician types, 56% of providers (121 of 216) declined to provide information about their assessment content. Provider answers were transcribed and coded categorically by two researchers (CO & JF), with initial inter-rater agreement >90% and disagreements resolved through open discussion.
Adults
Providers that reported details of their adult assessment process included 56 psychologists and 13 psychiatrists (n = 69). A Pearson’s chi-square test indicated that psychologists provided details of their adult assessment process at a higher rate than psychiatrists (χ2 (1, n = 131) = 38.301, p < .001, Cramer’s V = 0.541).
Adult assessment content
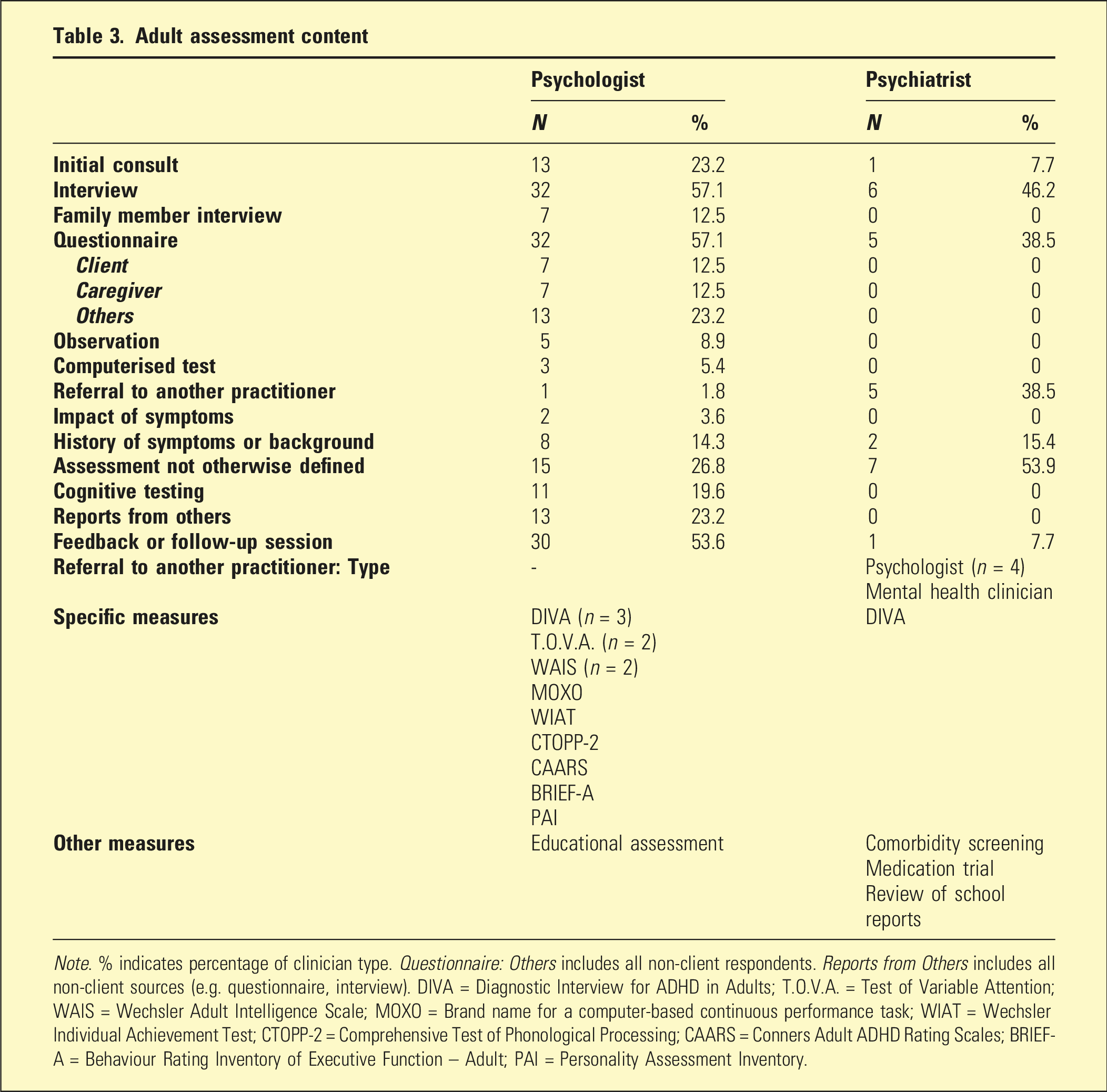
Note. % indicates percentage of clinician type. Questionnaire: Others includes all non-client respondents. Reports from Others includes all non-client sources (e.g. questionnaire, interview). DIVA = Diagnostic Interview for ADHD in Adults; T.O.V.A. = Test of Variable Attention; WAIS = Wechsler Adult Intelligence Scale; MOXO = Brand name for a computer-based continuous performance task; WIAT = Wechsler Individual Achievement Test; CTOPP-2 = Comprehensive Test of Phonological Processing; CAARS = Conners Adult ADHD Rating Scales; BRIEF-A = Behaviour Rating Inventory of Executive Function – Adult; PAI = Personality Assessment Inventory.
A Mann–Whitney U test comparing the number of measures reported for adult assessments was non-significant (U (67) = 246, p = .06, d = −0.0324), indicating no significant difference between the number of measures reported by psychologists (M = 3.268, SD = 1.355) and psychiatrists (M = 2.462, SD = 0.877).
The use of multiple informants was not indicated by 76.8% of psychologists and 100% of psychiatrists. A Pearson’s chi-square test found no significant difference in the indicated use of multiple informants by psychologists and psychiatrists in adult ADHD assessments (χ2 (1, n = 69) = 3.718, p = .05).
Children
Providers that reported details of their child assessment process included 62 psychologists, 7 psychiatrists, and 14 paediatricians (n = 83). A Pearson’s chi-square test comparing the availability of assessment information between clinician types was significant (χ2 (2, n = 158) = 48.303, p < .001, Cramer’s V = 0.553). Planned contrasts revealed that higher rates of information were available from psychologists compared with paediatricians (χ2 (1, n = 142) = 46.726, p < .001, Cramer’s V = 0.574) as well as psychiatrists (χ2 (1, n = 93) = 13.589, p < .001, Cramer’s V = 0.382) for child ADHD assessments. There was no significant difference between paediatricians and psychiatrists (χ2 (1, n = 81) = 1.077, p = .30). When tested against a Bonferroni-adjusted α of 0.0167, all contrasts remained significant.
Child assessment content
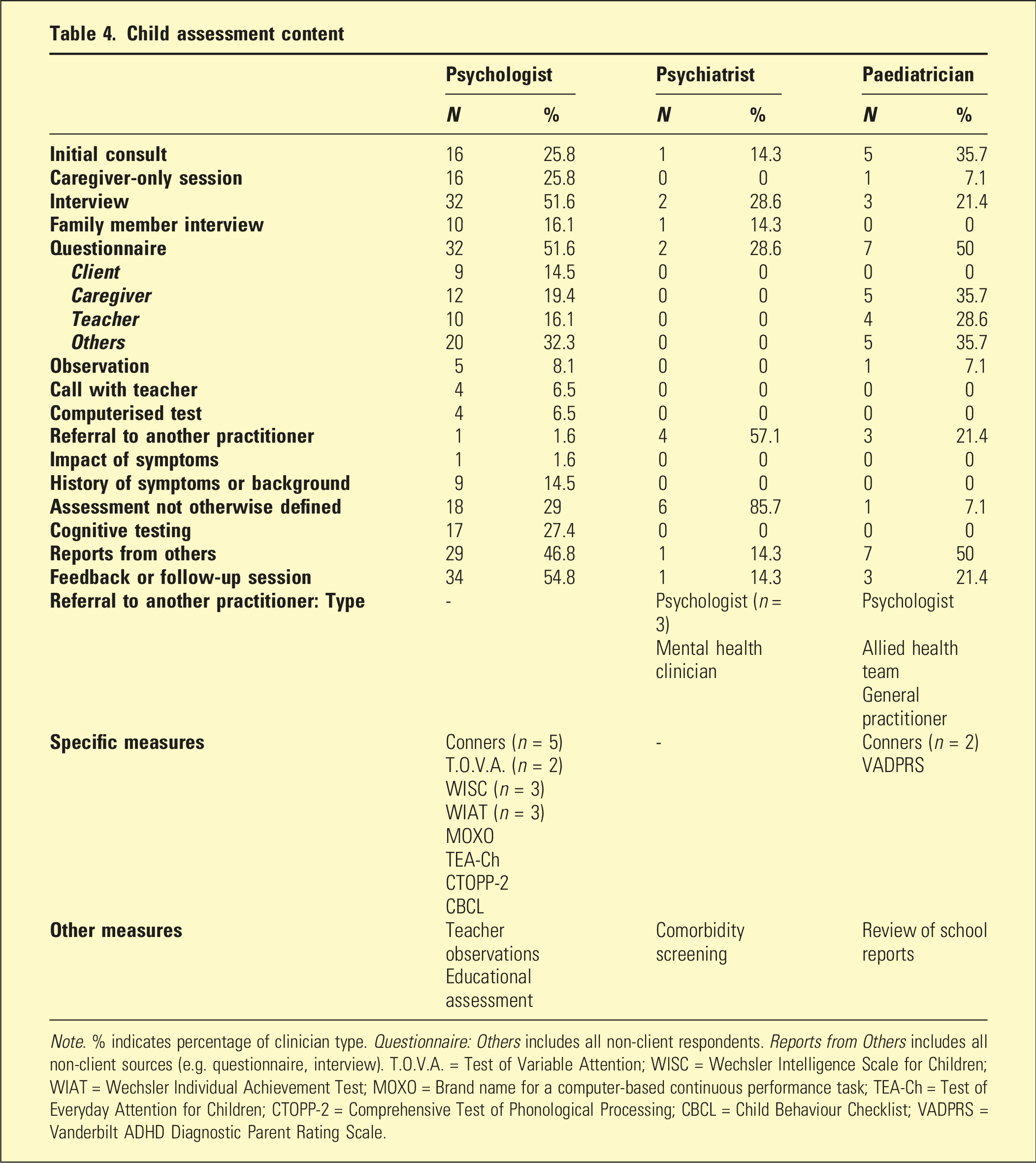
Note. % indicates percentage of clinician type. Questionnaire: Others includes all non-client respondents. Reports from Others includes all non-client sources (e.g. questionnaire, interview). T.O.V.A. = Test of Variable Attention; WISC = Wechsler Intelligence Scale for Children; WIAT = Wechsler Individual Achievement Test; MOXO = Brand name for a computer-based continuous performance task; TEA-Ch = Test of Everyday Attention for Children; CTOPP-2 = Comprehensive Test of Phonological Processing; CBCL = Child Behaviour Checklist; VADPRS = Vanderbilt ADHD Diagnostic Parent Rating Scale.
A one-way between groups ANOVA comparing the number of measures indicated between clinician types was statistically significant (F (2, 80) = 5.898, p = .004, η2 = 0.129). Post-hoc analyses with Tukey’s HSD found that psychologists (M = 3.435, SD = 1.532, range 1–8) reported significantly more measures than paediatricians (M = 2, SD = 1.301, range 1–5). No significant differences were found between psychologists and psychiatrists (M = 2.714, SD = 0.756, range 2–4), or psychiatrists and paediatricians. Effect sizes for these comparisons were d = −0.746, −0.278, and −0.238, respectively.
The use of multiple informants in child ADHD assessments was not endorsed by 53.2% of psychologists, 85.7% of psychiatrists, and 50% of paediatricians. A Pearson’s chi-square test of contingencies comparing the indicated use of multi-informant methods by clinician types was not statistically significant (χ2 (2, n = 83) = 2.888, p = .24).
Number of sessions
As the number of sessions required for an ADHD assessment was often provided as a range (e.g. three to four sessions), the average of the range was used for calculations aside from minimum and maximum values. As data on the duration of sessions was not collected during this study, the potential relationship between session number and length was not able to be investigated.
Adults
Respondents who provided session numbers for their adult ADHD assessments included 66 psychologists and 50 psychiatrists (n = 116). The average number of sessions for an adult assessment across clinician types was 2 (SD = 1.33, range 1–10). A Mann–Whitney U test comparing session numbers between clinician types was statistically significant (U (114) = 912, p < .001, d = −0.447), with psychologists (M = 3.045, SD = 1.451) requiring a higher number of assessment sessions than psychiatrists (M = 1.960, SD = 1.049) for adult assessments. See Figure 1. Adult average session number.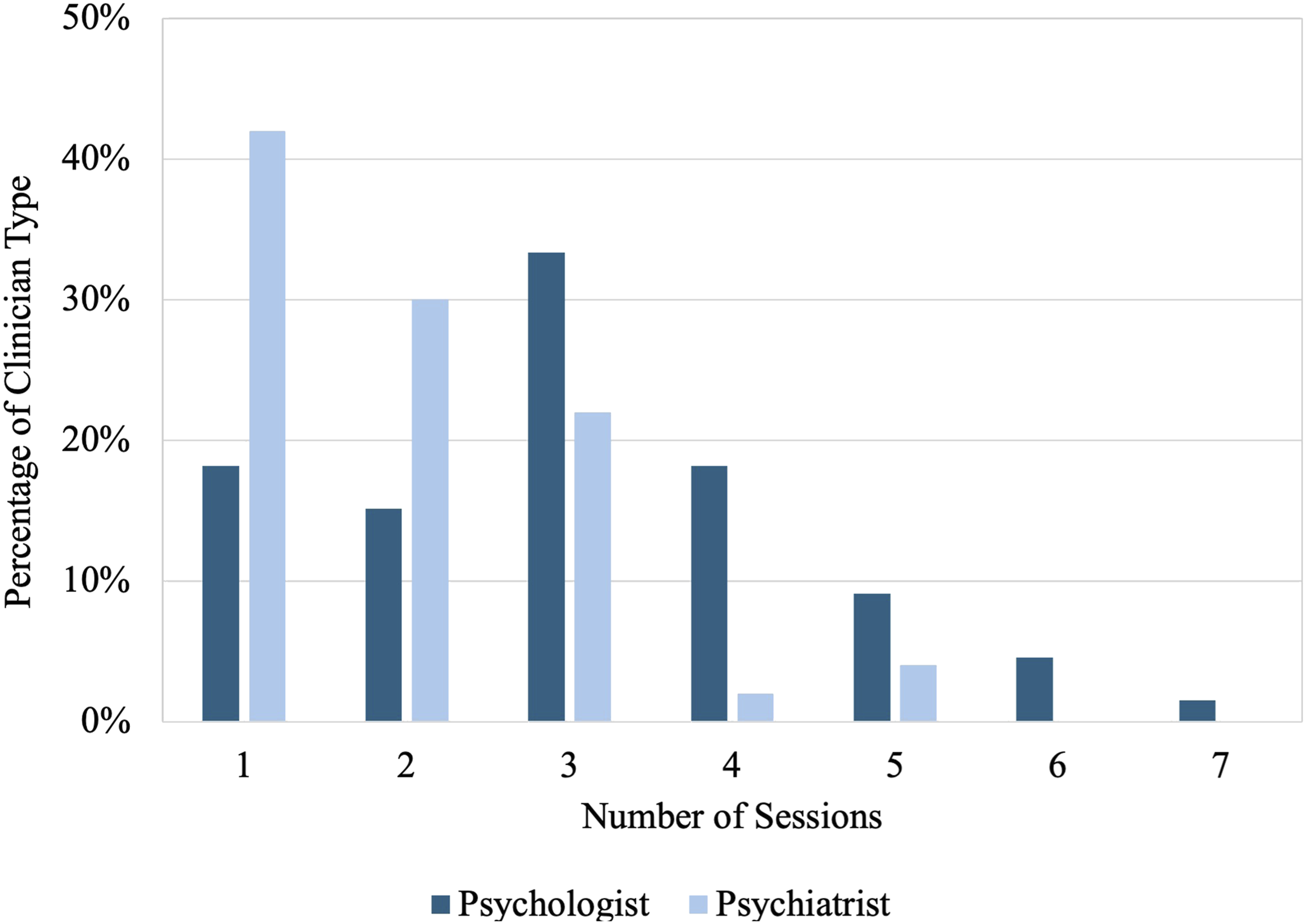
Children
Respondents who provided session numbers for their child ADHD assessments included 68 psychologists, 13 psychiatrists, and 37 paediatricians (n = 118). The average session number for a child assessment across clinician types was 3 (SD = 1.38, range 1–10). A significant Kruskal–Wallis test indicated that the number of sessions required varied between clinician types (H (2) = 20.024, p < .001, η2 = 0.157). Post-hoc Dunn’s comparisons demonstrated that psychologists (M = 3.294, SD = 1.415) reported requiring significantly more sessions than both paediatricians (M = 2.081, SD = 1.140) (p < .001) and psychiatrists (M = 2.308, SD = 1.251) (p = .019). No significant differences were found between paediatricians and psychiatrists (p = .62). When tested against a Bonferroni-adjusted α of 0.0167, only the contrast between psychologists and paediatricians remained significant. See Figure 2. Child average session number.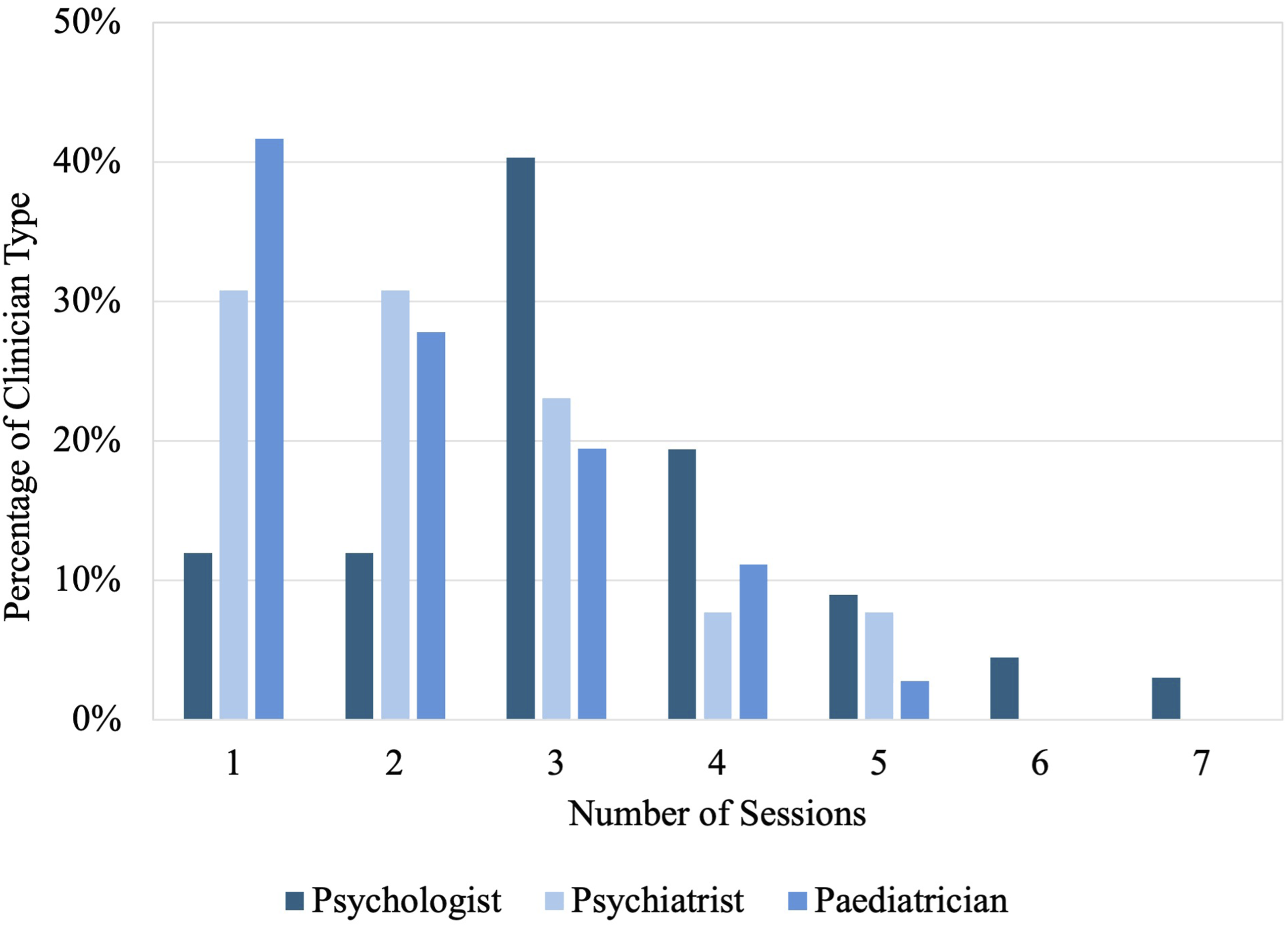
Discussion
This is the first study of its kind to investigate the information provided to consumers prior to booking an ADHD assessment across all Australian states and territories. As the study included the three most common clinician types in assessing ADHD,1–3 and called a representative sample of clinicians based on remoteness and clinician density, the generalisability of this study is strengthened. The inclusion of adult ADHD assessments in this study extends our knowledge of assessment practices into an increasingly important area. 2
There was a notable lack of information available to consumers, as 56% of assessment providers declined to provide any information about assessment content, limiting consumers’ ability to compare services before committing to potentially costly and lengthy assessment pathways.2,8 For both child and adult assessments, psychologists were found to provide details of their assessment process at higher rates than other clinician types. Of those providers who did report some information, it was often vague (i.e. 53.9% of psychiatrists offering adult assessments and 85.7% of psychiatrists offering child assessments reported ‘Assessment not otherwise defined’). It is possible that structural factors, such as referral requirements, medico-legal considerations, or administrative workflows may contribute to the lack of information provided by prescribing clinicians (i.e. psychiatrists and paediatricians) compared to psychologists. Some providers may also limit information about assessment procedures prior to referral confirmation or intake processes due to assessment integrity, consumer safety, or triage considerations.
Consistent with previous studies of Australian ADHD assessment practices,9–11 substantial variation in reported assessment processes was apparent. Higher rates of referrals to other practitioners were indicated by psychiatrists (and to a lesser extent paediatricians) than psychologists for both child and adult assessments. As these were most often referrals to psychologists as part of the assessment process, this highlights a potentially complex pathway towards a complete assessment. Consumers may be required to complete assessments with multiple practitioners (e.g. psychiatrist with referral to a psychologist) in order to receive treatment. This therefore increases the total cost, wait times, and number of sessions required to be completed, reducing the accessibility of these assessments.
While ADHD assessment guidelines often recommend the use of multiple informants, 3 these were not reported as part of the assessment process by the majority of providers (76.8% psychologists and 100% psychiatrists for adults; 53.2% of psychologists, 85.7% of psychiatrists, and 50% of paediatricians for children). No difference was found between clinician types in their reported use of multiple informants during assessments. This result should be interpreted with caution, as it may reflect limited information passed on by administrative staff, rather than actual clinical practice. However, studies of self-reported ADHD assessment practices have revealed similarly high guideline non-adherence (51.4%), 23 which is consistent with previous research demonstrating deviation from guidelines and variation in Australian assessment practices.9–11 This finding suggests that consumers seeking guideline-adherent assessments are unable to use clinician type as an indicator and should instead seek specific information from potential providers. Additionally, clinicians providing quality ADHD assessments may be motivated to ensure prospective clients are aware of their assessment practices in order to differentiate themselves. As administration staff may be responding to client calls, ensuring sufficient information about what is involved in assessments is available to staff may improve information accessibility.
The number of sessions required to complete an assessment indicated a longer process for psychologists (modal average of three sessions across ages) than psychiatrists (modal average of one session) for adult assessments, and paediatricians (modal average of one session) for child assessments. Analysis of session numbers may be complicated by an assumption of ongoing care by a paediatrician or psychiatrist for medication treatment, while an episode of care with a psychologist may be limited to the assessment process. A further complication is the duration of sessions, which is not necessarily uniform. Typical initial sessions for psychologists and psychiatrists are 50 to 60 minutes, and 30 to 45 minutes for paediatricians. 8 However, a single assessment session can last multiple hours, complicating attempts to relate session times to assessment duration, and especially as a proxy for thoroughness.
This study provides new data on the availability of assessment information from psychologists, psychiatrists, and paediatricians across Australia. The generalisability of this study is supported by the inclusion of all Australian states and territories, and the collection of the sample across clinician types and remoteness categories proportional to their distribution.14,15 The use of a secret shopper methodology reduced potential bias from participants’ awareness of being studied, and provided realistic data from a consumer perspective. 18
This study is limited by several factors. Due to the available contact data, responses were provided by clinicians and administrative staff. When both were available, clinician responses were prioritised. While the study provides a clear indication of available data to consumers prior to booking, this factor prohibits the application of reported practices as indicative of actual practices. As a secret shopper study, real-life outcomes in assessment content and session number could not be assessed. Due to available clinicians and response rates, data was not available for all clinician types and remoteness categories. Responses from psychiatrists and paediatricians about assessment content were limited and therefore impact the generalisability of this data. As leaving messages for return calls was not part of this study’s protocol, this may have reduced contact rates. This study does not include online-only assessment providers (without listed practice locations), who may vary in their practices.
Future studies are needed to investigate the decision-making processes and influencing factors for clinicians contributing to the availability of assessment information to consumers. Investigation of online-only assessment providers would also be pertinent, to gain a more comprehensive understanding of options available to consumers.
In conclusion, our findings demonstrate a lack of readily available information for consumers prior to booking an ADHD assessment in Australia. This lack of transparency limits the consumer’s ability to make informed choices before committing to a considerable financial and time investment. Based on these findings, clinicians may be motivated to improve administrative staff and client awareness of assessment practices. Policy changes may improve this area by clarifying the minimum information consumers should receive prior to booking appointments, or through improving consistency in assessment processes.
Footnotes
Ethics considerations
The research protocol was approved by the University of Wollongong Research Ethics Committee (2023/256).
Consent to participate
Consent to participate was waived by the ethics committee.
Author contributions
Clare O’Toole: Conceptualisation, Data curation, Formal analysis, Investigation, Methodology, Visualisation, Writing – Original draft, Writing – Review and editing
John Finlayson: Conceptualisation, Investigation, Methodology, Software, Writing – Review and editing
Stuart Johnstone: Supervision, Writing – Review and editing
Kate Croaker: Supervision, Writing – Review and editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by an Australian Government Research Training Program (RTP) Scholarship doi.org/10.82133/C42F-K220.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Due to limitations of ethics, data is not able to be made available.