
Abstract
Purpose
This study aimed to evaluate psychological distress and subjective sleep-related outcomes among individuals exposed to the Kahramanmaraş earthquakes.
Methods
This was a cross-sectional observational study comparing 68 earthquake survivors with 66 non-exposed controls. Participants’ levels of anxiety and depression, daytime sleepiness, sleep quality, post-traumatic stress, and risk of obstructive sleep apnea (OSA) were assessed using validated Turkish versions of standardized questionnaires. Between-group comparisons were performed using nonparametric tests, followed by age-adjusted regression analyses.
Results
Earthquake survivors exhibited significantly higher anxiety, depression, post-traumatic stress, and poorer subjective sleep quality (Pittsburgh Sleep Quality Index) compared with controls, and these associations remained significant after age adjustment (all p < 0.05). Daytime sleepiness (Epworth Sleepiness Scale) did not differ between groups. Although STOP-BANG scores differed in unadjusted analyses, this association was no longer significant after adjustment for age.
Conclusion
Earthquake exposure was associated with persistent psychological distress and impaired subjective sleep quality approximately one year after the disaster, independent of age differences. These findings underscore the importance of integrated mental health care and assessment of sleep complaints in disaster-affected populations, while highlighting the need for future studies incorporating objective sleep measures.
Earthquakes are disasters that leave profound impacts not only on the physical environment but also on social lives and psychological well-being. As sudden and unpredictable events, earthquakes can disrupt individuals’ sense of safety and trigger psychological trauma. 1 They are known to cause a range of psychiatric disorders such as acute stress disorder, depression, anxiety disorders, and post-traumatic stress disorder (PTSD), in addition to notable disturbances in sleep patterns.1,2
Sleep quality is a fundamental indicator of both physical and mental health. Traumatic experiences can lead to persistent sleep complaints, including disturbed subjective sleep quality and excessive daytime sleepiness, and may also increase vulnerability to sleep-disordered breathing through stress-related pathways. 2 However, the extent to which post-disaster sleep complaints remain evident after accounting for key confounders such as age and gender is less clearly described.
The earthquakes that occurred in southeastern Türkiye on February 6, 2023, with their epicenter in Kahramanmaraş, caused not only widespread physical destruction but also had a significant adverse impact on the mental health of the population. Subsequent research has demonstrated that the disaster had environmental, respiratory, and psychological consequences.3–5
Following the two major earthquakes (moment magnitude [Mw] 7.7 and 7.6), thousands of aftershocks occurred, with magnitudes reaching as high as Mw 6.7, and aftershocks have continued to occur. It is therefore reasonable to expect that such a rare, high-magnitude, and ongoing traumatic event would be associated with a wide range of psychological problems, including persistent subjective sleep complaints. While many disaster studies emphasize acute outcomes, fewer have examined self-reported sleep-related disturbances approximately one year after the event. Accordingly, the present study aimed to compare anxiety, depression, post-traumatic stress symptoms, and self-reported sleep-related outcomes between earthquake survivors and non-exposed controls about 1 year after the earthquake.
Methods
This study was designed as a cross-sectional observational study to evaluate the differences in psychological symptoms and sleep-related outcomes between individuals affected by the Kahramanmaraş earthquakes on February 6, 2023, and those who were not affected. Participants in both groups were recruited from pulmonology outpatient clinics.
Participants in the earthquake survivor group were adults (aged 18 and over) who had been present in earthquake-affected areas during the disaster and later presented to the Pulmonology Outpatient Clinic of Samandağ Hospital. The control group consisted of adults (aged 18 and over) who had not been exposed to the earthquake and were recruited from patients presenting to the Pulmonology Outpatient Clinic of Hacettepe University Faculty of Medicine. Participants in both groups were recruited using consecutive sampling among patients presenting to the respective clinics. Data were collected approximately one year after the earthquake through face-to-face interviews using structured questionnaire forms. Written informed consent was obtained from all participants prior to enrollment. To minimize the potential confounding effect of pre-existing mental health conditions on the study outcomes, individuals with a known psychiatric diagnosis or those receiving active psychiatric medical treatment prior to the earthquake were excluded.
To assess anxiety and depression levels, the Beck Anxiety Inventory (BAI)6,7 and the Beck Depression Inventory (BDI)8,9 were used. The Epworth Sleepiness Scale (ESS) was used to evaluate daytime sleepiness10,11; the Pittsburgh Sleep Quality Index (PSQI) was used to assess sleep quality12,13; and the PTSD Checklist for DSM-5 (PCL-5) was used to assess post-traumatic stress levels.14,15 The risk of OSA was assessed using the STOP-BANG questionnaire.16,17 All sleep-related outcomes were assessed using self-report questionnaires; no objective sleep measurements (e.g., polysomnography or actigraphy) were performed.
Statistical analyses were conducted using SPSS version 23.0 and Python (version 3.x). Continuous variables were summarized as medians and interquartile ranges (IQR), and categorical variables as frequencies and percentages. Between-group comparisons of continuous variables were conducted using the Mann–Whitney U test, and Chi-square test or Fisher’s exact test, as appropriate.
Given the significant age difference between earthquake survivors and controls, multivariable regression models were constructed to evaluate the association between disaster exposure and outcomes while accounting for age and sex. In these models, psychological symptoms and sleep-related measures were treated as the dependent variables, while survivor status (survivor vs control), age, and sex were entered as independent predictors. For continuous outcomes, multivariable linear regression was used to calculate unstandardized Beta (β) coefficients with 95% confidence intervals (CIs). For categorical outcomes based on clinical cut-offs, multivariable logistic regression was used to calculate odds ratios (ORs) with 95% CIs. Among earthquake survivors, sex differences in scale scores were evaluated using age-adjusted linear regression models, with scale scores as dependent variables and sex as the independent variable. Missing data across variables were minimal (ranging from 1 to 5 cases for most variables and 13 cases for PCL-5) and were handled via complete-case analysis. A two-sided p-value <0.05 was considered statistically significant.
The study was conducted with the necessary institutional approvals, and ethical approval was obtained from a non-interventional clinical research ethics committee (approval date: May 21, 2024; decision number: 14).
Results
Demographic characteristics of earthquake survivors and controls
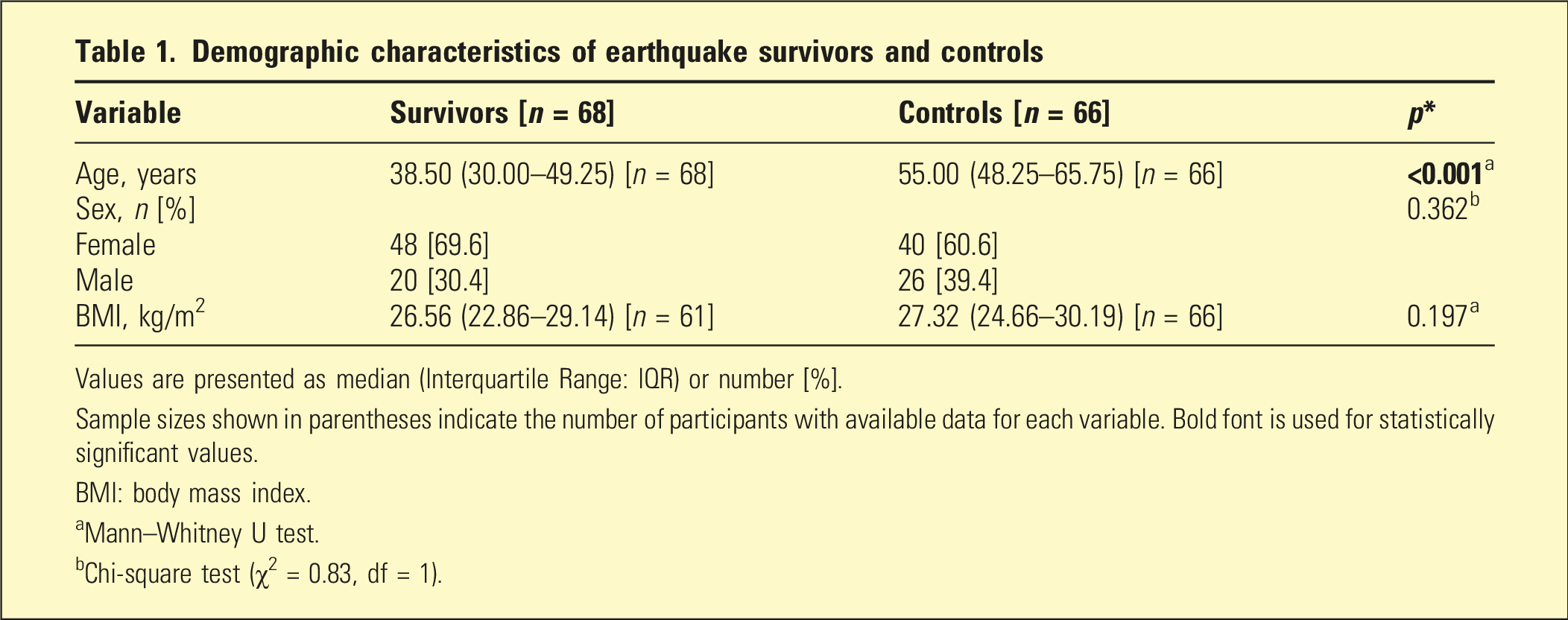
Values are presented as median (Interquartile Range: IQR) or number [%].
Sample sizes shown in parentheses indicate the number of participants with available data for each variable. Bold font is used for statistically significant values.
BMI: body mass index.
aMann–Whitney U test.
bChi-square test (χ2 = 0.83, df = 1).
Comparison of scale scores between survivors and controls, with age- and sex-adjusted associations
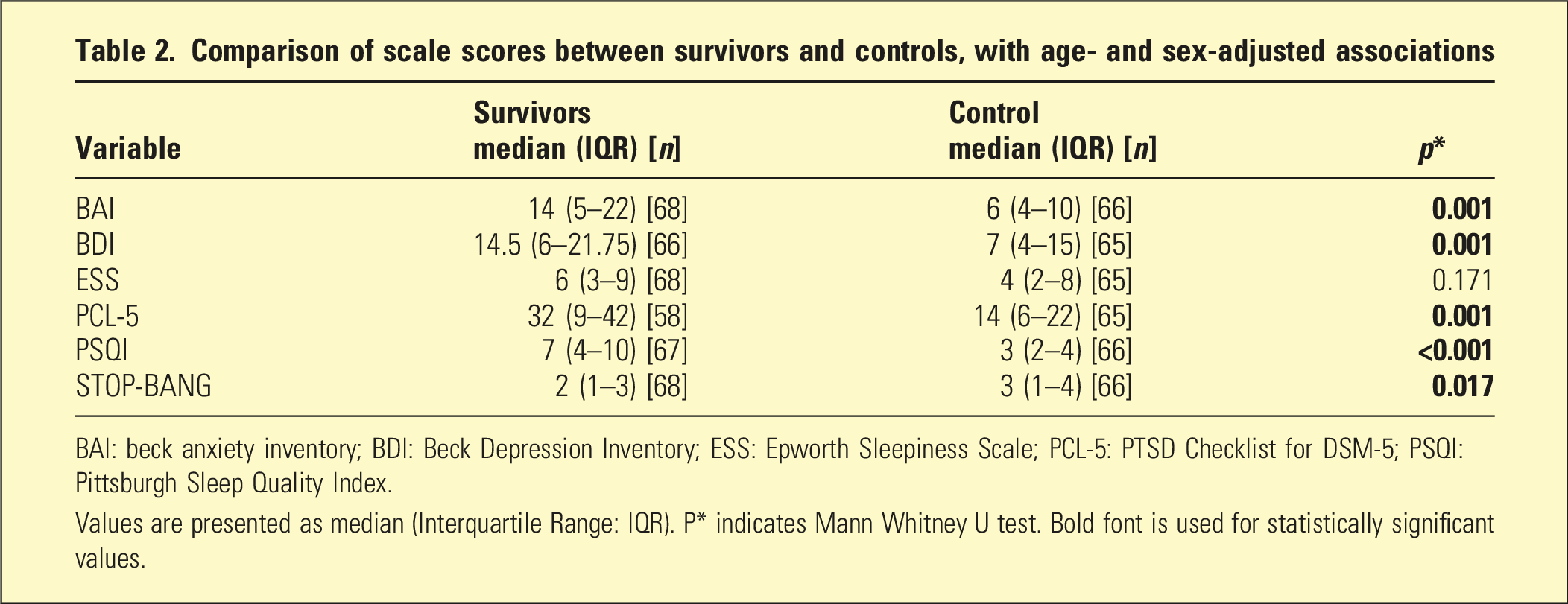
BAI: beck anxiety inventory; BDI: Beck Depression Inventory; ESS: Epworth Sleepiness Scale; PCL-5: PTSD Checklist for DSM-5; PSQI: Pittsburgh Sleep Quality Index.
Values are presented as median (Interquartile Range: IQR). P* indicates Mann Whitney U test. Bold font is used for statistically significant values.
Multivariable regression analyses for the survivors and controls
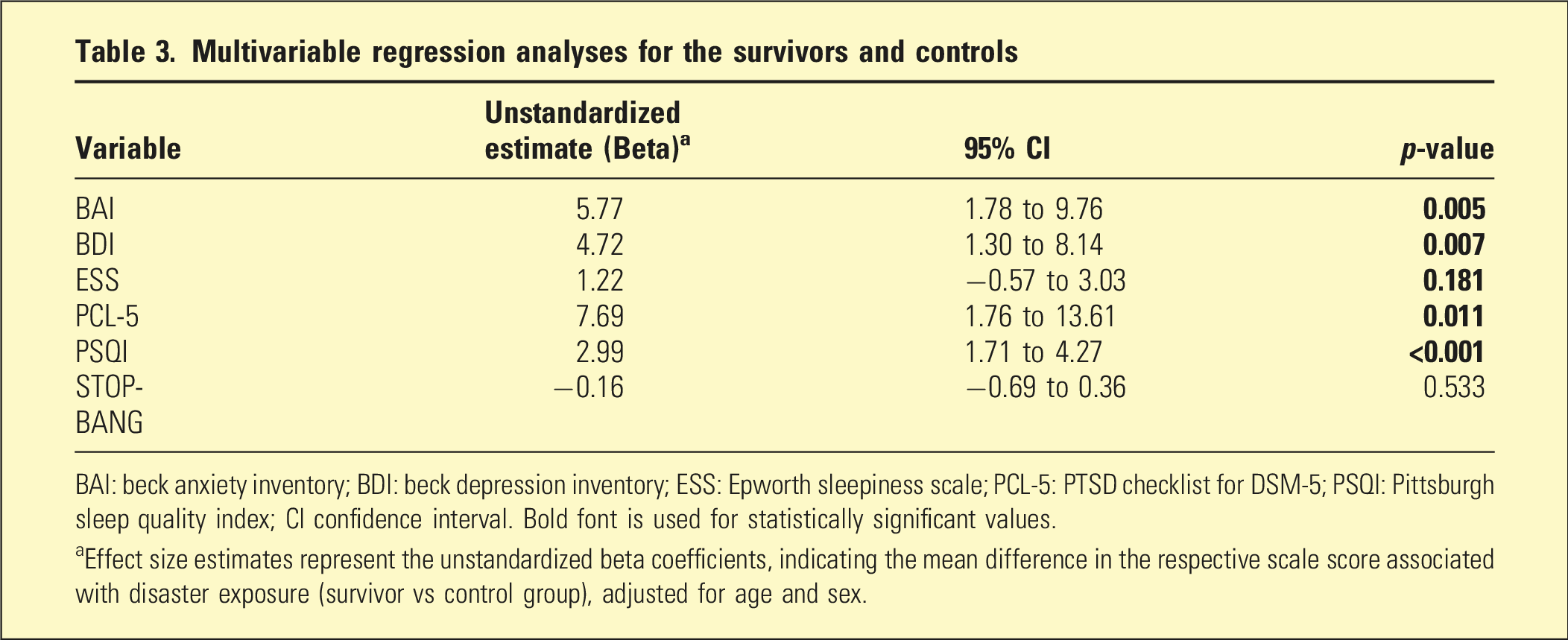
BAI: beck anxiety inventory; BDI: beck depression inventory; ESS: Epworth sleepiness scale; PCL-5: PTSD checklist for DSM-5; PSQI: Pittsburgh sleep quality index; CI confidence interval. Bold font is used for statistically significant values.
aEffect size estimates represent the unstandardized beta coefficients, indicating the mean difference in the respective scale score associated with disaster exposure (survivor vs control group), adjusted for age and sex.
With respect to scale positivity, survivors more frequently exceeded cutoff values for BAI (p < 0.001), BDI (p < 0.001), PCL-5 (p = 0.001), and PSQI (p < 0.001) compared in unadjusted analyses. In age- and sex-adjustment multivariable logistic regression models, these associations remained significant, with survivors demonstrating higher odds of positivity for BAI (OR = 5.51, 95% CI: 1.92 to 15.75, p = 0.001), BDI (OR = 3.67, 95% CI: 1.46 to 9.22, p = 0.006), PCL-5 (OR = 14.35, 95% CI: 1.61 to 127.78, p = 0.017), and PSQI (OR = 5.71, 95% CI: 2.41 to 13.53, p < 0.001). ESS positivity did not differ between groups in either unadjusted (p = 0.623) or age- and sex-adjusted analyses (OR = 1.21, 95% CI: 0.40 to 3.67, p = 0.726).
Sex differences in scale scores among earthquake survivors (unadjusted and age-adjusted)
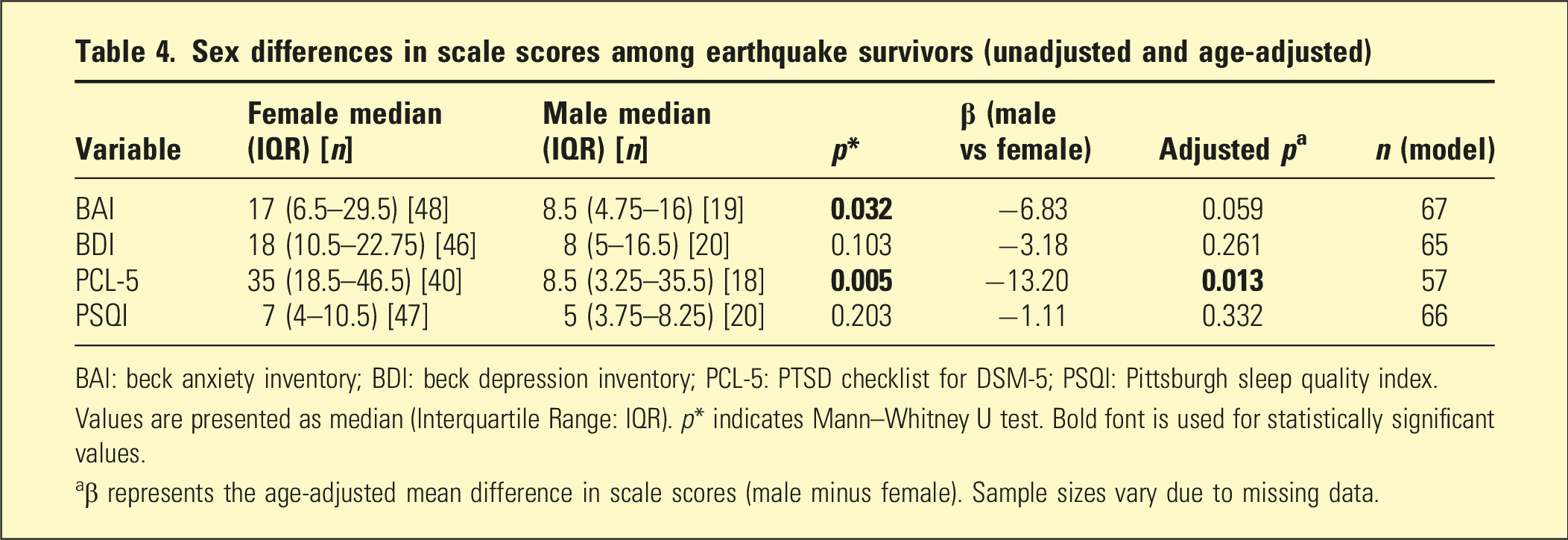
BAI: beck anxiety inventory; BDI: beck depression inventory; PCL-5: PTSD checklist for DSM-5; PSQI: Pittsburgh sleep quality index.
Values are presented as median (Interquartile Range: IQR). p* indicates Mann–Whitney U test. Bold font is used for statistically significant values.
aβ represents the age-adjusted mean difference in scale scores (male minus female). Sample sizes vary due to missing data.
Discussion
In this study, conducted approximately one year after the Kahramanmaraş earthquakes, we found that earthquake survivors exhibited significantly higher levels of anxiety, depression, and post-traumatic stress symptoms, as well as poorer subjective sleep quality, compared with non-exposed controls. Importantly, these associations remained significant after adjustment for age, indicating that the observed differences were not solely attributable to the younger age of the survivor group. In contrast, daytime sleepiness (ESS) and OSA risk as assessed by STOP-BANG were not independently associated with survivor status after age adjustment. These findings largely align with the existing literature, which emphasizes that earthquakes can have long-lasting psychological effects in addition to their physical impact.
The significantly higher BAI and BDI scores among earthquake survivors reflect common psychological responses to traumatic experiences.18,19 Psychological distress following disasters is believed to be driven not only by the traumatic event itself but also by post-disaster uncertainty, disruption of social support, and chronic stress. 3 Similar to our findings, persistent anxiety symptoms have been reported several years after major earthquakes. 19 Meta-analytic evidence suggests that older adults may experience a disproportionately higher burden of post-disaster mental health symptoms (e.g., PTSD and adjustment-related symptoms), highlighting the importance of accounting for age in disaster research. 20 Given that the survivor group was younger than the controls (Table 1), age represented a potential confounder and a source of limited generalizability to older adults. Nevertheless, depressive and anxiety symptoms remained independently associated with survivor status after age adjustment. While PTSD is often prioritized in post-disaster mental health care, our results demonstrate that depressive and anxiety symptoms were also highly prevalent and remained independently associated with survivor status after age adjustment. This highlights the need to screen not only for PTSD but also for depression and anxiety disorders in individuals with trauma exposure.3,21
The elevated PCL-5 scores among survivors are in line with the existing literature, indicating an increased likelihood of PTSD following large-scale disasters.3,5,18,22 The development of PTSD is influenced not only by trauma severity but also by factors such as perceived social support and pre-existing vulnerability.5,23 Considering the magnitude of the Kahramanmaraş earthquakes and the prolonged disruption of living conditions in the affected regions, the persistence of post-traumatic stress symptoms observed in our cohort is plausible. Notably, the between-group difference in PCL-5 scores persisted more than one year after the earthquakes, suggesting that post-traumatic stress symptoms may remain clinically relevant well beyond the acute phase and underscoring the need for sustained mental health support.
With respect to sleep-related outcomes, our findings primarily reflect subjective sleep quality rather than objective sleep physiology. Survivors reported significantly poorer sleep quality as measured by the PSQI, and PSQI positivity remained associated with survivor status after age adjustment. Similar impairments in subjective sleep quality among earthquake survivors have been reported across different populations.2,24 In contrast, ESS scores did not differ between groups, suggesting that perceived nocturnal sleep disturbance did not necessarily translate into increased daytime sleepiness in this sample. Daytime sleepiness may also be influenced by comorbid medical conditions, medication use, and sleep opportunity, which were not comprehensively captured in this study. Therefore, this discrepancy may be explained by the multifactorial nature of daytime sleepiness and the limitations inherent in self-report instruments.
Previous studies have suggested an association between PTSD and sleep-disordered breathing through mechanisms such as sleep fragmentation and autonomic dysregulation. 25 Although STOP-BANG scores differed between groups in unadjusted analyses, this association was no longer significant after age adjustment, indicating that age was a major contributor to OSA risk in this cohort. STOP-BANG is a screening tool rather than a diagnostic measure, and no objective sleep studies were performed in our study. Therefore, our findings should not be interpreted as reflecting true OSA prevalence but rather highlight the limitations of questionnaire-based OSA risk assessment in trauma-exposed populations with age imbalance.
Among survivors, female participants exhibited higher unadjusted anxiety and PTSD symptom severity, and female sex remained independently associated with higher PCL-5 scores after age adjustment. This is consistent with prior reports identifying female sex as a risk factor for post-traumatic stress following disasters.1,26,27 However, no significant sex differences were observed for depressive symptoms or subjective sleep quality after adjustment, which aligns with studies reporting inconsistent associations between sex and post-disaster depression. 28 Potential explanations proposed in the literature for sex-related differences include biological vulnerability as well as sociocultural factors such as differential exposure to stressors and help-seeking behaviors.28,29
Several limitations should be acknowledged. The cross-sectional design precludes causal inference. Sleep-related outcomes were assessed exclusively through self-report questionnaires (which may be subject to recall and reporting bias), without objective measurements such as polysomnography or actigraphy. Participants were recruited from pulmonology outpatient clinics. While this setting provides a practical, real-world clinical context for evaluating patients with sleep and respiratory complaints, it inherently introduces selection bias. Additionally, the survivor and control groups differed in age. Although we accounted for this through age-adjusted multivariable regression analyses, the potential for residual confounding remains, as age is a strong determinant of both sleep characteristics and psychological status. Moreover, selecting the control group from a different geographic region (Ankara vs Hatay) may have introduced unmeasured confounders, such as differences in baseline socioeconomic status, environmental exposures, and lifestyle characteristics. Lastly, detailed information regarding individual trauma exposure, ongoing secondary stressors (e.g., housing instability) and socioeconomic changes was not available, preventing adjustment for these potentially important confounders. Furthermore, although patients with known psychiatric diagnoses were excluded, formal psychiatric evaluations were not performed, preventing definitive adjustment for pre-earthquake mental health status.This study adds to the disaster and sleep literature by evaluating psychological symptoms and self-reported sleep-related outcomes approximately one year after the Kahramanmaraş earthquakes, a period that is less frequently addressed in post-disaster research and may better reflect longer-term clinical needs. The unique context of two consecutive high-magnitude earthquakes with ongoing aftershocks and prolonged disruption of living conditions provides an important setting to examine sustained symptom burden beyond the acute phase. The inclusion of a non-exposed control group strengthens interpretability by allowing estimation of excess psychological distress and sleep complaints associated with disaster exposure. Furthermore, by accounting for age differences in the primary analyses, we reduce the likelihood that the observed between-group differences are solely attributable to demographic imbalance. Although objective sleep assessments were not available, the combined use of validated instruments for sleep quality (PSQI), daytime sleepiness (ESS), and screening-level OSA risk (STOP-BANG) offers a clinically pragmatic characterization of sleep-related complaints that may inform post-disaster screening and referral pathways.
In conclusion, this study provides clinically relevant evidence that psychological distress and impaired subjective sleep quality, which remain observable at least one year following a major earthquake, even after accounting for age differences. Our findings emphasize the need for sustained, integrated post-disaster mental health services that address anxiety, depression, PTSD, and sleep complaints in affected populations. Screening strategies should extend beyond PTSD alone and incorporate broader psychological assessment and sleep-related symptoms. Future studies incorporating longitudinal designs and objective sleep measurements are warranted to further clarify the mechanisms linking trauma exposure and sleep disturbances.
Footnotes
Acknowledgments
Language editing support was used to improve clarity and readability of the manuscript. All scientific content, data analysis, interpretation, and conclusions were generated solely by the authors.
Ethical considerations
The study was conducted with the necessary institutional approvals, and ethical approval was obtained from the Non-Interventional Clinical Research Ethics Committee of Mustafa Kemal University on May 21, 2024, with decision number 14.
Author contributions
Hande Yuce Ozdemir: Visualization, Writing - Review & Editing, Writing - Original Draft, Data Curation, Formal Analysis, Investigation. Hayri Can Ozden: Writing - Review & Editing, Investigation, Visualization, Writing - Original Draft, Formal Analysis. Hande Celik: Visualization, Project administration, Data Curation, Conceptualization, Methodology. Basaran Demir: Project administration, Conceptualization, Methodology. Ahmet Ugur Demir: Project administration, Conceptualization, Methodology, Supervision, Formal Analysis, Writing - Review & Editing. Hande Yuce Ozdemir and Hayri Can Özden contributed equally to this work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Conference presentations
This study was presented in full as an oral presentation at the 28th Annual Congress of the Turkish Thoracic Society, held on April 23–27, 2025. Data specific to the earthquake survivor group were also presented as a poster at the ERS Sleep and Breathing Conference 2025, held on April 10–13, 2025. All authors have read and approved the final version of the manuscript. This study was conducted with the contributions of Hande Yuce Ozdemir, Hayri Can Ozden, Hande Celik, Basaran Demir, and Ahmet Uğur Demir at Hatay Samandag State Hospital and Hacettepe University.