
Abstract
Background
With rising youth mental health needs, there is an urgent call for new service models that are cost-effective, accessible, and non-duplicative. The Youth Engagement & Treatment Team Initiative (YETTI) was implemented in the federal Eastern metropolitan health region of Victoria, Australia, to deliver tertiary-level mental health interventions within trusted headspace sites, and to provide specialist consultation to their staff.
Method
Over six years, YETTI supported 981 young people aged 12–25 years (and families/carers) whose severe and complex mental ill-health was beyond the remit of enhanced primary care but did not meet eligibility for public mental health services.
Results
Pre-post outcome comparisons demonstrated clinically and statistically significant improvements in symptoms and functioning for 67% of the cohort, including reductions in Health of the Nation Outcome Scale Child Adolescent total and scale scores (F = 600.48, df = 1,582, p < 0.001). Further, most consumers (81.4%) reported improved mental health and functioning on the Kessler Psychological Distress Scale (K10). High satisfaction with YETTI was reported by 90% of consumers with an 84% response rate, indicating a positive impact on young people during a developmentally vulnerable period.
Conclusions
Overall, these findings suggest that YETTI is an acceptable and effective model in bridging the youth mental health service gap. Future research could examine longer-term clinical, functional and system-level outcomes.
Keywords
Mental illness is the leading cause of disease burden in young people aged 10–24, with the high and rising prevalence of mental health disorders in young people carrying significant personal, familial, and economic losses.1–3 Increasing mental health challenges experienced by Australia’s young people parallel global trends. The 2021 Australian census recorded 4.6 million young people aged 10–24 years comprising 18% of the population. Among 16–25 year-olds, 38.8% met criteria for having experienced a mental disorder in the past 12 months (a significant rise from 26.4% in 20074,5), as did 13.9% of those aged 4–17, with 2.1% of these children experiencing severe disorders requiring clinical care. 6 Of note, recent exacerbations in mental ill-health particularly in young people, have also been associated with social determinants including the pandemic and climate change. 7
National responses to this increase have included the establishment of over 150 headspace centres designed to offer early intervention to young people aged 12–25. Their effectiveness in reducing mental ill health, however, remains debated,8–10 consistent with international trends where increased investment has not significantly reduced prevalence of mental health problems.11,12 Despite this, headspace is widely trusted by Australian young people, especially vulnerable groups such as LGBTQIA+ 13 and First Nations young people, 14 as well as those from low socioeconomic or rural backgrounds.15,16
Many young people attending headspace require more intensive and specialized mental health care from private practitioners including psychiatrists, psychologists, or social workers. Barriers to access remain, however, and include high costs and inflexible centre- and appointment-based service models that do not well accommodate those affected by severe mental health difficulties. 17 The Australian public tertiary mental health system provides free multidisciplinary care to those with complex mental health disorders and psychosocial needs, though demand far exceeds capacity leaving many young people unable to access appropriate treatment.
With rising youth mental health needs, there is a growing demand for accessible, cost-effective, and non-duplicative services. YETTI was a fee-free, innovative model offering specialized multidisciplinary mental health treatment to young people whose needs exceeded the capacities of headspace or private practitioners but did not meet tertiary care criteria. YETTI aimed to bridge this critical service gap by complementing and augmenting existing youth health services. They did so through providing early intervention to young people at risk of or experiencing serious mental illness who unless they deteriorated might otherwise be inadequately or not treated. YETTI was federally funded (end 2017–end 2023) by the Eastern Melbourne Primary Health Network (EMPHN), and auspiced by the State funded Eastern Health Infant, Child & Youth Mental Health Service (ICYMHS). This paper outlines the model and evaluates its effectiveness.
Model of Care
Co-designed with young people, families, headspace, and guided by a Youth Peer & Family Carer Advisory Group, YETTI aimed to: a. Improve early identification and treatment of 12–25-year-olds with severe mental health issues, especially those from marginalised groups who do not readily access mental health services. b. Provide flexible, stage-based systemic care. c. Streamline and strengthen service pathways whilst avoiding duplication. d. Build capacity within the primary care sector.
The model embedded specialist child and youth mental health expertise within youth-friendly settings like headspace. A multidisciplinary team, led by a Consultant Psychiatrist, combined applied ICYMHS treatment expertise with strong clinical governance. Co-location at headspaces ensured a trusted entry point for young people and families which recognised their individuality and contextual needs. While headspaces focus on individuals, YETTI used a systemic approach, involving families, partners, or friends alongside the young person.
Therapeutic Interventions
YETTI offered consumers stepped and tailored treatment responses based on the young person’s and family’s clinical needs. These interventions included: • Secondary Consultation: Support to primary workers through assistance with health education, case formulation, strategy development/implementation, and referral advice. • Primary Consultation: A solution-focused session with the young person, family, and sometimes the referrer, to identify presenting issues, risks, and provide referrals, strategies and/or orientation to YETTI care. • Brief Intervention: A mental health response comprising (up to) six solution-focused sessions with the young person, alone or with family/carer.
18
• Full Assessment and Case Management: Including standard ICYMHS assessment, intervention, supervision and clinical reviews.
Large scale studies show that few children and young people with mental health issues receive even minimally adequate treatment.17,19 Therefore, alongside a focus on public health service throughput, there is increased scrutiny on outcome data to inform quality improvement and funding formulae. The aims of the current paper therefore were to: 1. Determine potential changes in functioning and symptom/wellbeing of YETTI consumers by comparing discharge to intake outcome data. 2. Examine the acceptability and tolerability of YETTI intervention using qualitative and quantitative data regarding consumer, carer and stakeholder agency satisfaction with the YETTI program.
Method
Context
The EMPHN catchment comprises 12 local government areas ranging across metropolitan and rural regions within Victoria. It covers 24% of the Victorian population (1.62 M), 1.1% of whom identify as Aboriginal or Torres Strait Islander peoples, 11% as being part of the LGBTQIA + communities, and 16% (259,200) of whom are aged 12–25%. Mental health is the primary chronic health condition in the Region. Continuous data collection, quality improvement work including 360-degree feedback, and quarterly reporting to the funding body provided rich data for review and refinement of the service. This research employed a retrospective cohort design study and explored real-world data in a naturalistic Australian ICYMHS setting. The study was approved by the organisation’s Human Ethics and Research Committee (LR25-072-121684) and followed STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines. 20
Sample
Target populations for YETTI.
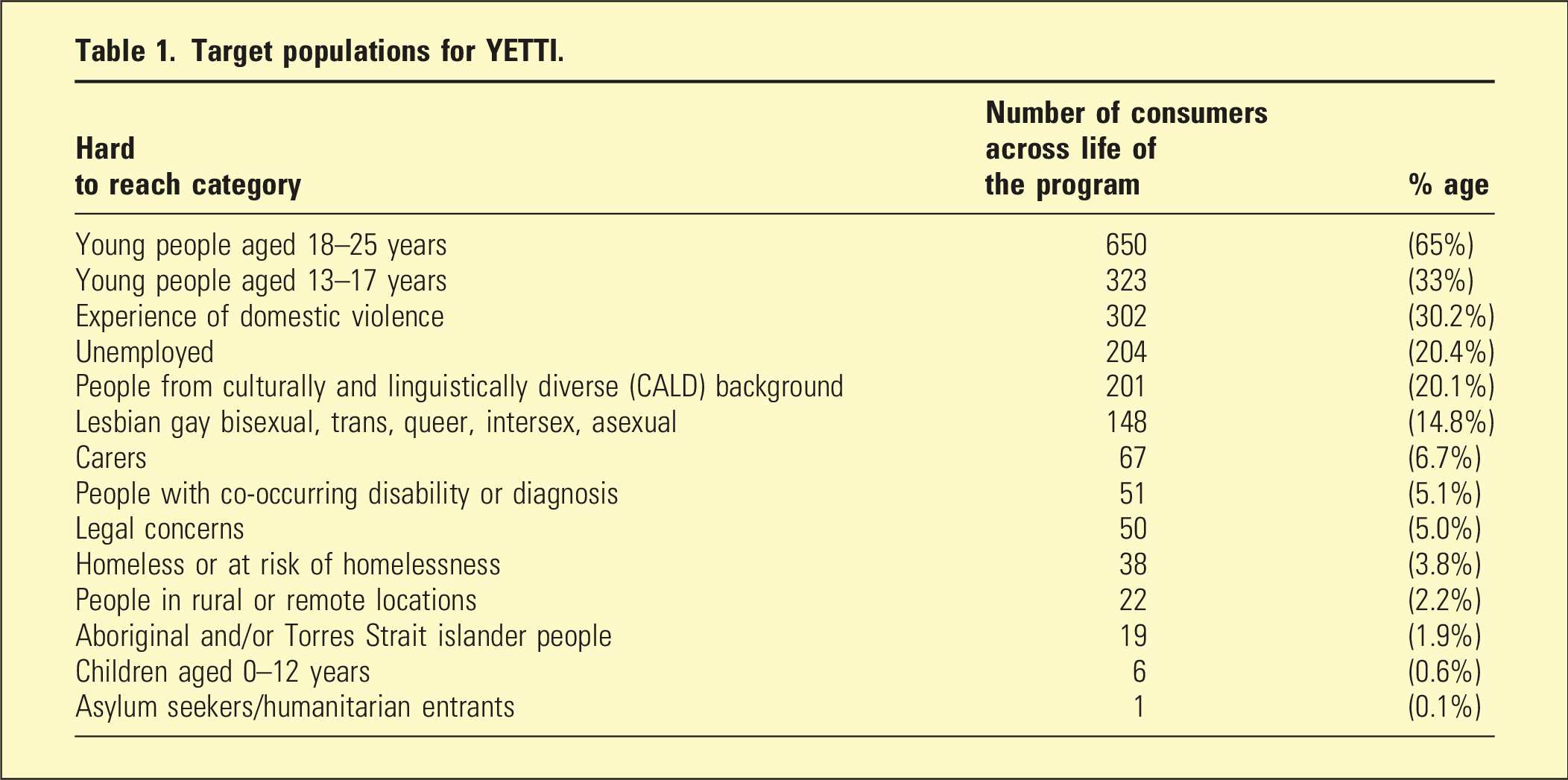
During its operation YETTI also provided indirect mental health support to approximately a further 860 young people through specialist mental health secondary consultation to the headspace and youth service staff who were working with them.
Measures
A set of consumer and clinician outcome measures was used to assess changes in consumer symptomology and functioning. A range of consumer, carer, and stakeholder measures assessing satisfaction with YETTI were also utilized. All scales used in the study (except the co-designed satisfaction-with-service measures) have extensive psychometric reliability and validity data. • The Health of the Nation Outcome Scale for Children & Adolescents (HoNOSCA)
21
is a mental health clinician rated measure which indicates severity of 13 mental health problems on a scale of 0–4, with two items examining consumer/carer knowledge regarding these difficulties. • The Kessler Psychological Distress Scale (K10)
22
is used with those aged 18 and over as a brief general measure of psychological distress associated with levels of nervousness and depressive feelings, with items scored from 1–5. • The Strengths & Difficulties Questionnaire (SDQ)
23
is a 25 item scale which measures emotional and behavioural functioning. There are versions for young people (aged 11–17), parents and teachers. • The Session Rating Scale (SRS)
24
employs four analogue scales (scaled 0–10) to assess aspects of therapeutic alliance from a consumer perspective: Relationship, Goals; Approach; and Overall satisfaction. The SRS is delivered once during the episode of care. YETTI staff and the youth advisory group co-designed two satisfaction measures aimed to assess consumer/carer and worker/agency experience of the service. The first, completed by consumers and/or family members at discharge, included five scales (rated 1–5): clinician contact, approach, support received, improvements made, and the support plan. The second, a stakeholder survey completed quarterly, was also scored from 1 to 5 and assessed: overall satisfaction, response to referrals, and consumer outcomes. Both surveys concluded with space for additional qualitative feedback.
Procedure
This suite of routine outcome measures was collected prospectively over the 6 years of operation. They were administered to all consumers at the initial session then every 3 months thereafter, and again at discharge – which was usually collaboratively planned between clinician and consumer. If the consumer solely attended a single session, only one set of completed measures was collected.
Data Analysis
The results from all available data associated with individuals, their families, and care systems were collected and cleaned with mean replacement utilized for item based missing data. Matched pair HoNOSCA data of consumer scores at intake and discharge were analysed using one-way ANOVAs through Excel and SPSS 29. Data from consumer rated measures (K10, and SDQ) were collected by the EMPHN then provided to YETTI. They are reported here percentage-wise to reflect improvement (a discharge total score of 1 or more points above the intake total score), no change (equal discharge and intake total scores), or deterioration (discharge score 1 or more below intake score). Mean consumer and carer satisfaction with YETTI is reported in graph and text form, with stakeholder satisfaction reported in text.
Results
Consumer Treatment Characteristics
Of the 981 consumers seen by YETTI, 188 attended a single session only. This generally occurred when the consumer thought the one session was beneficial and sufficient, or the consumer wanted and/or was better suited to a different service. The 793 other consumers entered case management (including brief intervention). The average length of stay across the life of the program reduced from nearly 12 months at its commencement in late 2017, to just over 7 months in 2023. Most consumers and/or family members were seen weekly. The recorded diagnosis/presenting problems of 863 (88%) YETTI consumers are shown below in Figure 1. Presenting concerns of YETTI consumers.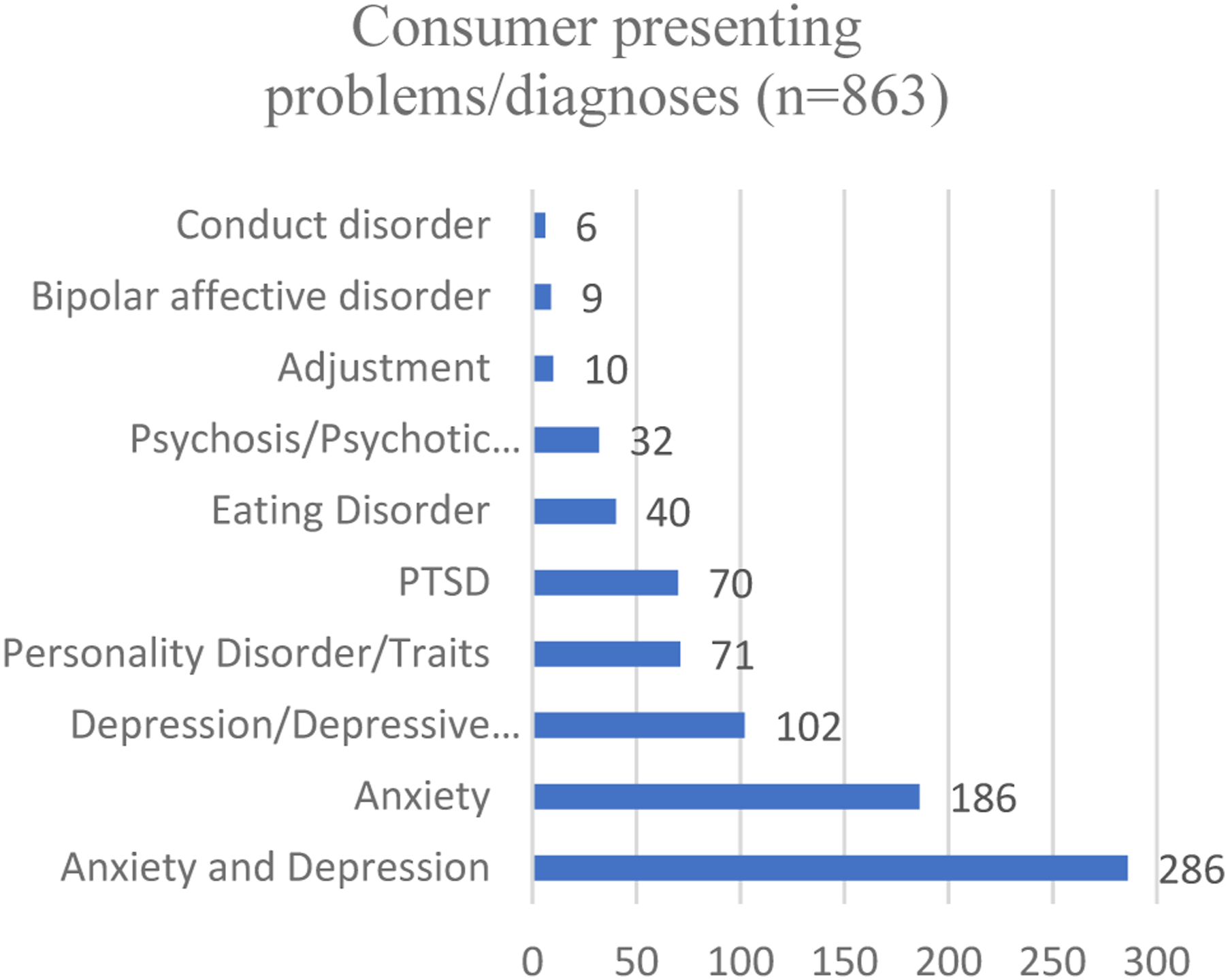
Comorbidities included: 66% with substance use problems, 80% engaged in self-harm and over 50% experienced suicidal ideation and/or actions.
Clinician Rated Outcomes
Analysis of the scores from intake and discharge matched pair treatment HoNOSCAs were available for 583 cases (representing 574 unique consumers). The mean initial total HoNOSCA score of the Service cohort was 17.5 similar to, if not slightly higher than that of same aged National Child & Youth Mental Health Service clients (M = 15.6) across the same years of operation. 25 Service data demonstrated an average symptom reduction of six points across episode of care – higher than the National CYMHS change score of 4.5.
This represents both a clinically, as well as statistically significant improvement in symptoms and functioning (F = 600.47, df = 1, 582, p < 0.001) from start of treatment to finish, with a large effect size (partial eta sq = 0.51) (Figure 2). A change in HoNOSCA score of four or over is considered significant.
26
Of the current cohort 67.2% of the cohort had a change score of four or above, with a further 13.5% having a positive change score of between one and three. Further, at discharge consumers of the Service had a mean HoNOSCA score (M = 11.5) similar to that of the Victorian CYMHS average (M = 11.1). YETTI consumer HoNOSCA scores pre to post treatment. Lower scores – reduced symptomology and improved functioning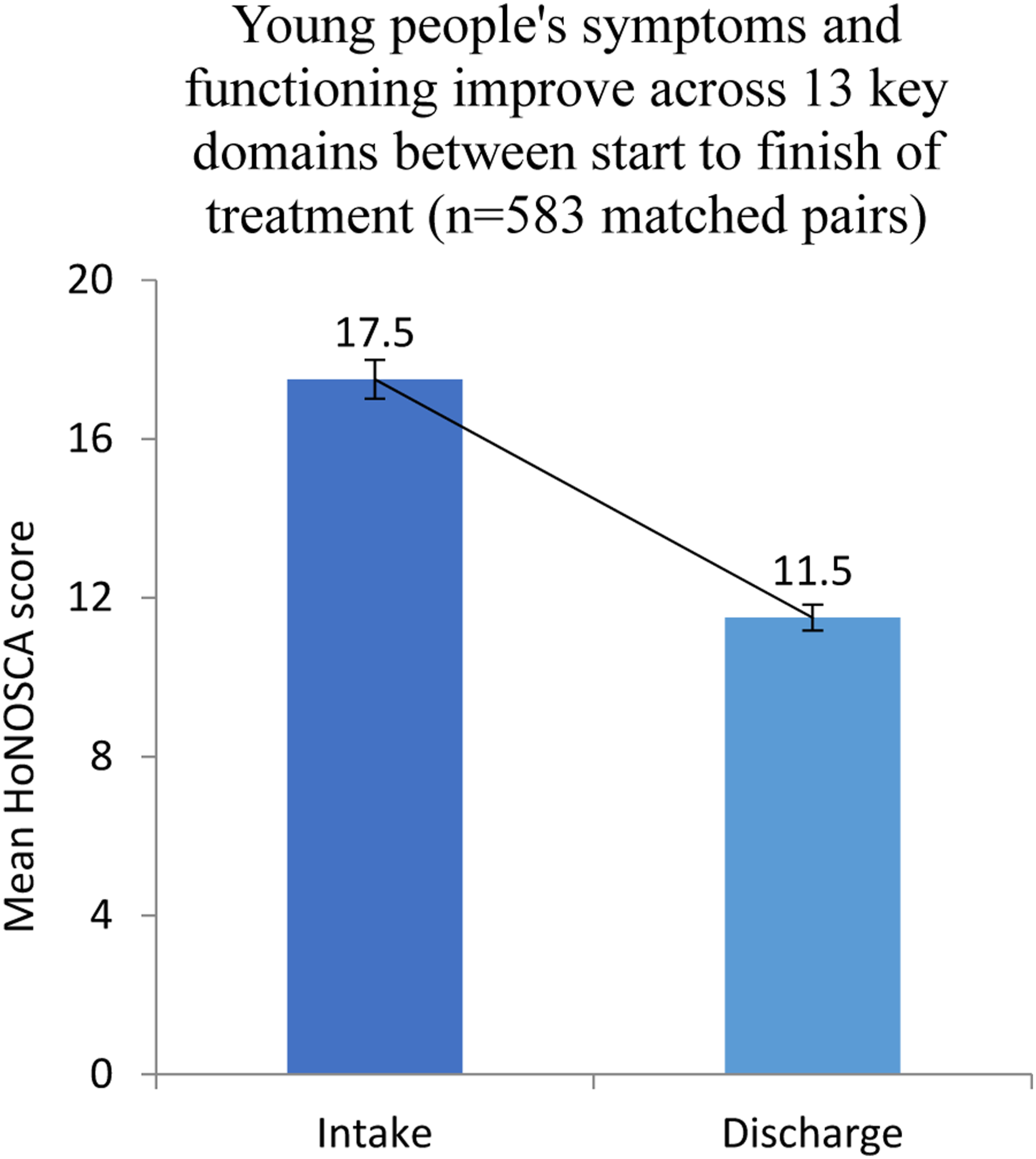
Figure 3 below outlines the average intake to discharge change of individual HoNOSCA scales. Overall, the most severe initial scale scores for YETTI consumers were Emotional Symptoms, Family relationships, Peer relationships, Overactivity, and Self-care. Post hoc analysis incorporated a Bonferroni correction from p < .05 to p < .003 due to there being 13 comparisons. Results showed a significant reduction in symptomology across all HoNOSCA scales from treatment start to finish (F scores between 31.56 and 246.25, df = 1, 551, p < .001). Effect sizes varied from small 0.05 for Hallucinations, to large 0.49 for Emotional symptoms. Problems with Self-harm and School/Vocational attendance problems almost halved. Average consumer HoNOSCA scale score pre and post treatment.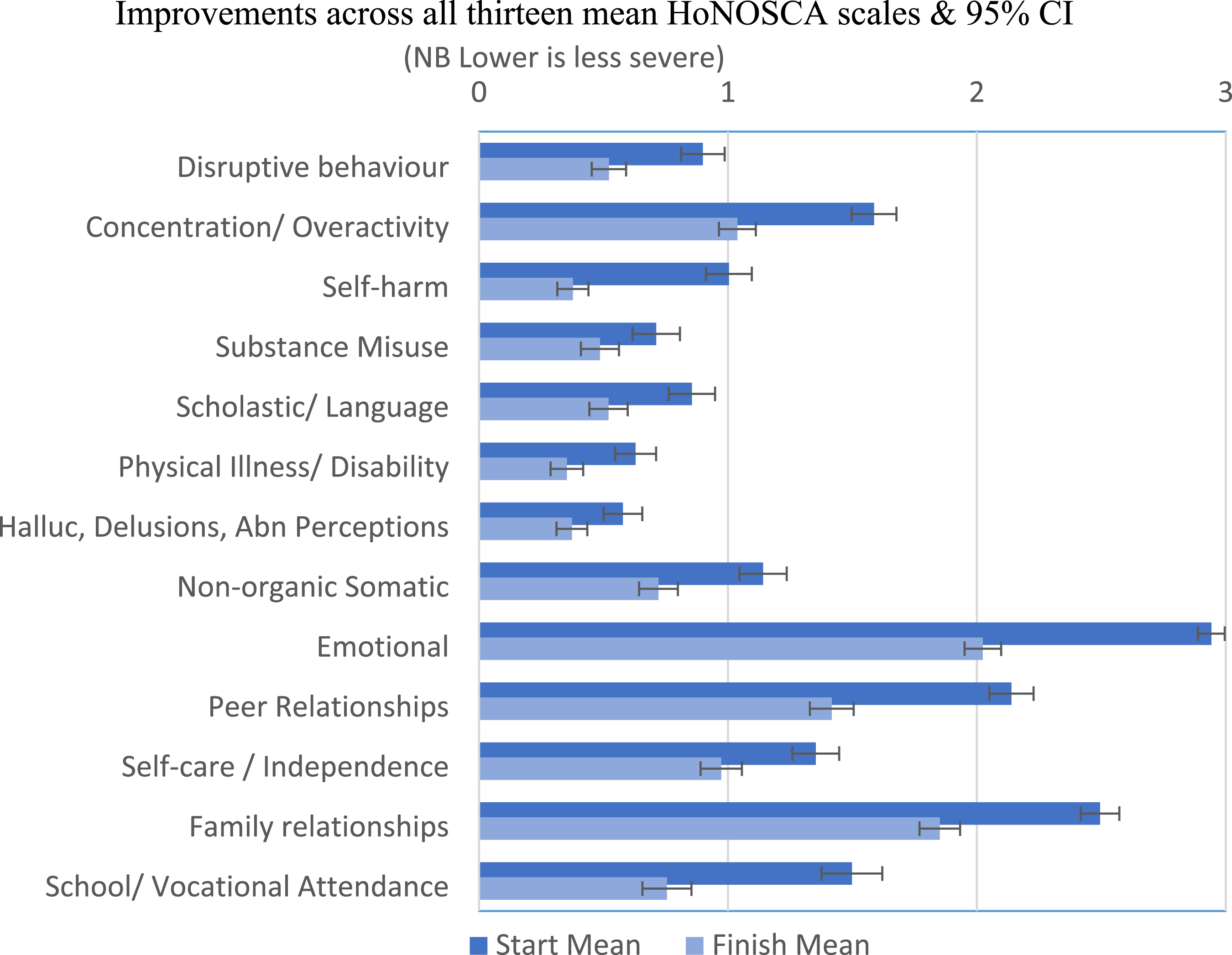
Consumer Self-reported Outcomes
Nearly 50% of case managed consumers experienced difficulty in completing self-report measures (SDQ and K10) subsequent to intake. This was particularly during COVID with increased use of telehealth. A total of 409 consumers completed both intake and discharge K10s and a further 134 provided matched pair SDQs. From this combined group 81.4% reported at the end of their engagement with YETTI that their mental health had improved. These consumers either stated they did not require further support or were referred onto a more generalist service (e.g. back to headspace). No change in mental health was indicated by 13.6% of YETTI consumers, with 5% indicating a deterioration generally requiring a more intensive level of care such as referral to a tertiary mental health service (ICYMHS).
The Session Rating Scale was completed by 531 consumers at the conclusion of one of their clinical sessions (usually within the first 3 months of care). All four satisfaction dimensions of the SRS (Relationship, Goals, Approach, and Overall) were rated at 90% or greater.
Satisfaction With YETTI
Consumers and Carers
From 842 surveys completed by consumers and carers, overall satisfaction with YETTI was rated as 84.8%. Consumer/carer ratings across the varying domains of YETTI care are outlined in Figure 4. Consumers and family satisfaction with YETTI across 5 care domains.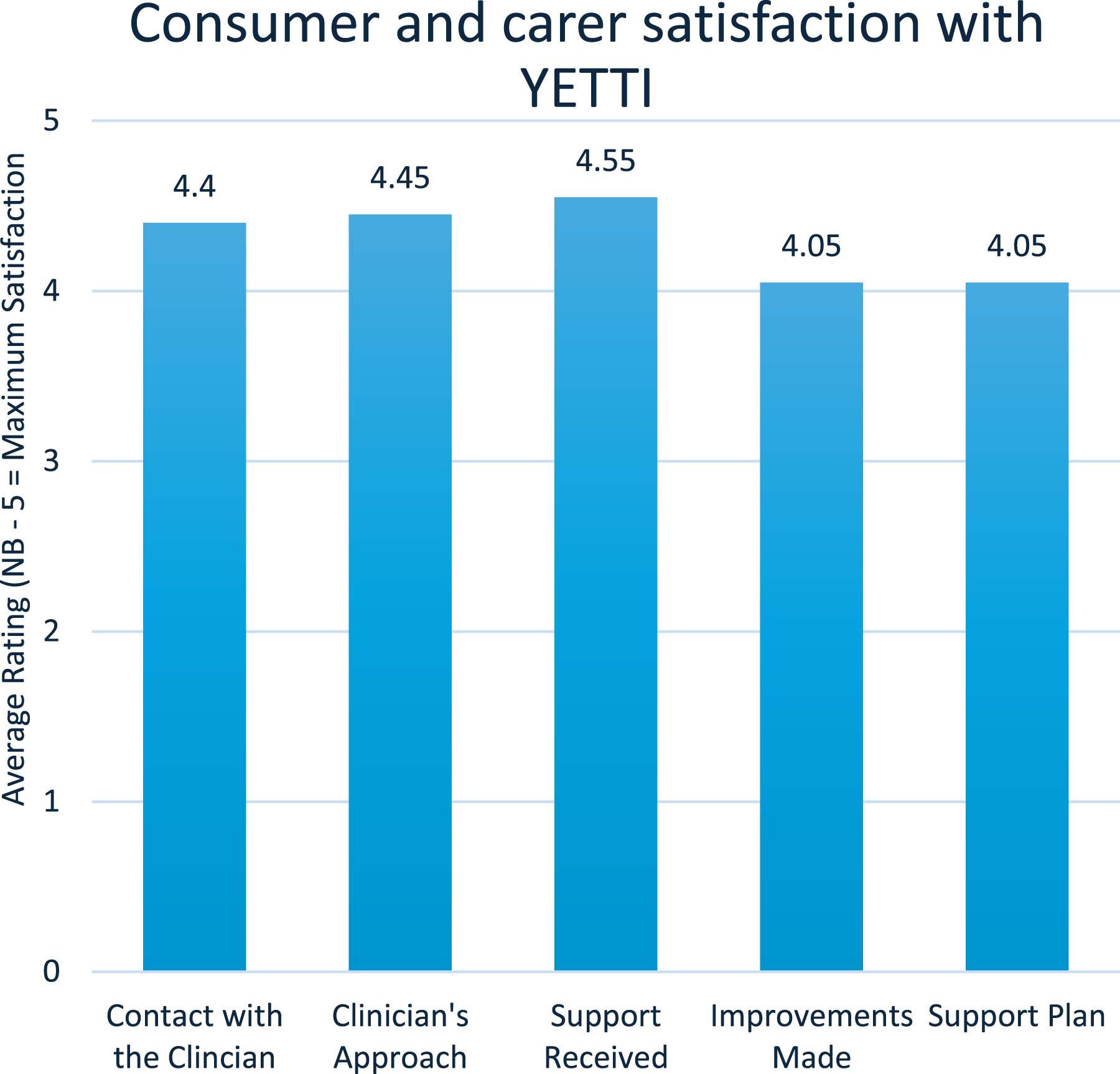
Qualitative data from consumers and carers regarding the treatment and support they received from YETTI were generally very positive. • YETTI gave me a good understanding of my situation and the reassurance that things are going to be ok. • YETTI explained what I’m feeling and validated it, talked me through coping mechanisms and explained what to do in stressful situations. Also changed the way I think about myself - like self-compassion • We couldn’t have done this without the support from YETTI. Thank you for keeping my daughter alive. • YETTI helped with communication between our young person and our family. We were able to open up to create more strategies/ideas.
Stakeholders
Stakeholder satisfaction was also rated by managers and clinicians within the 15 key youth services which partnered with YETTI across the Region. Satisfaction with the service was rated very highly (Overall 95%, ‘consumer outcomes’ 97%, and ‘Response to referrals’ 93%). Qualitative feedback indicated stakeholders valued the strongly collaborative and supportive relationship with YETTI in relation to its consumer work, as well as the formal and informal upskilling and clinical support YETTI provided to their agency. • Their program and the support they provide young people and their families is incomparable. We rely on YETTI so heavily and would be lost without their phenomenal support. There is no need for improvements unless you can clone the team. (A headspace leader) • They need more staff and resources-they are so busy. Their work is brilliant and much needed. We have a very effective and collaborative working relationship (headspace worker)
Discussion
The current study reports an evaluation of a pilot clinical youth mental health service model designed to provide tertiary level treatment and support to young people and their systems of care, whose mental health and psychosocial needs were too complex and/or acute for them to be assisted by lower levels of care. YETTI operated through collaboration with enhanced youth health and wellbeing services operating within real-world settings. The majority of those accessing YETTI identified as being a member of at least one priority target group (e.g. First Nations, LGBTQIA+). Given the relatively high average initial HoNOSCA score, it is important to note that individuals with more severe problems have greater scope for improvement. Noting this, the Service reported an overall clinically and statistically significant six-point reduction in consumer symptoms and difficulties with functioning, between intake to discharge – a larger reduction than the National CYMHS average. This was also a consistent symptom reduction across all 13 HoNONSCA scales. A large number of young people accessed YETTI across its six years of operation, 80.7% of whom were clinician-rated to have improved, with 81% self-reporting improvement in their mental health and well-being across their episode of care. Further, consumers, carers and stakeholders consistently expressed high levels of satisfaction with both the YETTI service delivery model, as well as the quantitative and qualitative outcomes. As such, the YETTI program is associated with improved mental health outcomes through reportedly accessible and acceptable interventions, even across the time of COVID which required an agile, rapid transition to include telehealth as a mode of service delivery.
Services which support young people with severe mental ill-health are generally community based and include the promotion of living skills, educational and/or occupational outcomes.27,28 These are very important aspects of a person’s mental well-being and can work particularly well in concert with sound clinical treatment, something that can be difficult for vulnerable young people to access or afford. It is likely a number of factors potentially contributed to the positive outcomes reported here: the multidisciplinary approach; interventions involving both the young person and their system of care challenging a culture which tends to conceptualise mental ill-health as individually situated; YETTI operated within headspaces which vulnerable young people report viewing as trustable and safe 9 ; headspace triaging and referring consumers made YETTI more efficient and able to focus on intervention; the model requiring cooperation and collaboration between often siloed federal and state funded mental health services, creating a continuum of care with potential for step-up and step-down care pathways informed by changing consumer need.
Limitations and Future Directions
Key limitations of this research include: the lack of a control group due to YETTI operating in a naturalistic setting; the inability to undertake an economic analysis and Service comparison with other youth mental health providers due to session data being collected directly by the funding body; and the use of broad functioning/symptom psychometric tools that may not detect subtle symptom changes over time. Additionally, as part of routine outcome measurement, clinicians were not independent of the HONoSCAs so there is a possibility that rating bias occurred. Satisfaction measures were specifically co-designed as feedback for program improvement and lack validation, with likely ceiling effects making it difficult to differentiate between each groups’ respective scores on the different scales. Whilst reflecting broader headspace trends, 29 two thirds of YETTI consumers were female, so greater engagement with young males and gender diverse people is needed, as they may access support seldom or differently. 30 Finally, while clinician-rated matched pair data was sound, higher discharge response rates from consumers and carers would strengthen findings. Future research could incorporate digital tools to enhance this.
Conclusion
In conclusion, despite limitations, the YETTI model seems to offer an acceptable treatment program associated with positive change in mental health and wellbeing in a significant number of vulnerable young people. Future longitudinal and ecological momentary analysis research would go some way to determining the role of the YETTI service model in arresting and reversing mental health deterioration in young people, thus potentially reducing a disrupted developmental trajectory, mental health crises, and/or the need for costly longer term ICYMHS involvement.
Footnotes
Acknowledgements
The authors wish to sincerely thank all those who worked with the Youth Engagement and Treatment Team Initiative whose data contributed to this evaluation. Also, the Eastern Melbourne Primary Health Network for funding the YETTI team. Finally, thanks also to the YETTI team members and leadership whose commitment and expertise supported all aspects of this initiative across its six years of operation.
Ethical considerations
Ethics approval for this project was granted by the Eastern Health Human Research and Ethics Committee (LR25-072-121684).
Author contributions
HM contributed to the study design, literature search, data analysis, first and subsequent drafts. TC contributed to the study design, literature search, initial draft, and subsequent reviews. LA, NH, & PJ, contributed to the study design, initial and subsequent drafts, SI contributed to initial and subsequent drafts, PB contributed to the study design, data analysis, first and subsequent drafts.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support this study is available on reasonable request and approval from the Eastern Health HREC.