
Abstract
Purpose
Adolescent mental health need is high in Aotearoa New Zealand, yet engagement of private psychologists with adolescents is limited. This study examined how private psychologists decide whether to accept adolescent referrals within a mixed public and private mental health system.
Method
Semi structured interviews were conducted with 14 purposively sampled private psychologists across three practice groups. These comprised those seeing 12 to 19 year olds, those with an adults only focus, and those who accepted adolescents selectively. Data were analysed using reflexive thematic analysis.
Results
Willingness to accept adolescent referrals reflected the interaction of interest and feasibility appraisals. Interest was shaped by comfort, perceived fit, interpretations of adolescent reluctance, and beliefs about therapeutic leverage. Feasibility appraisals filtered interest through judgements about whether adolescent work could be delivered safely and sustainably in private practice, including competence and scope concerns, system fragmentation, limited consultation and escalation options, and business viability. These appraisals were associated with conditional engagement strategies such as age thresholds and caseload limits.
Conclusions
Willingness to accept adolescent referrals was appraisal-based and potentially modifiable. Improving access may require both supporting interest formation and strengthening feasibility conditions, including consultation and escalation pathways across sectors.
Keywords
Many mental health conditions first emerge during adolescence. A recent meta-analysis estimated onset for 34.6% of disorders by age 14 and 48.4% by age 18, underscoring the importance of timely developmentally responsive intervention. 1 Adolescent mental health is increasingly described as global crisis, with substantial disability burden and worsening mental health among young people during the COVID period, further widening treatment gaps. 2
In Aotearoa New Zealand (hereafter Aotearoa), adolescents and young adults experience persistently high levels of unmet mental health need, and improving access remains a system priority.3–5 Māori young people experience disproportionate mental health burden and inequitable access to services, further highlighting the importance of workforce capacity and distribution.3–5 Workforce shortages are widely identified as a contributing factor, particularly within publicly funded mental health and addiction services.6–8 Access barriers also reflect geographic maldistribution, service thresholds, and affordability constraints within mixed public and private systems. 9 In Aotearoa, adolescents may access psychological care through publicly funded specialist, primary or community services, or alternatively, through privately funded pathways. Private psychologists usually practice in self-employed or group practice arrangements.
Workforce responses have largely focused on expanding publicly funded provision and strengthening training pipelines.10,11 Less attention has been directed toward the role of psychologists practising in private settings. Recent national psychology workforce data indicate that nearly 40% of registered psychologists primarily work in private practice (Te Whatu Ora|Health NZ. personal communication, 2026). However, willingness to work with younger adolescents appears limited. Analyses of a national survey conducted by the authors, found a clear age gradient, with psychologists reporting lower willingness to work with younger adolescents. When responses from private psychologists who reported working with adolescents were extrapolated to the full sample, only approximately one third of surveyed private psychologists were willing to work with adolescents aged 14 to 15 years, with lower proportions for those aged 12 to 13 years (Wall S, Lucassen M, and Fleming T, unpubl. data, 2025).
Within adolescent mental health research, attention has largely centred on clinical processes once young people have entered services.12–14 This literature highlights engagement challenges, therapeutic alliance processes, and developmental complexity. However, it offers limited insight into whether an adolescent referral is accepted in private practice.
The closest parallel evidence comes from research examining clinicians’ orientation toward specific client groups, most consistently studied in relation to older adults.15–18 This work suggests that interest in working with a population is shaped by attitudes, anticipated difficulty, and perceived therapeutic effectiveness, and that education and contact can influence these appraisals. Transferability to adolescent work is uncertain because adolescent practice introduces distinctive considerations including developmental variability, family involvement, confidentiality dilemmas, and escalation planning. 12 In private practice, where clinicians exercise autonomy over caseload composition and bear responsibility for business sustainability and risk management, these considerations may be particularly salient. 19
What remains underexamined is how established private psychologists appraise adolescent referrals before engagement begins. We identified no Aotearoa empirical studies focused on this decision point. This study therefore explores factors shaping private psychologists’ willingness to work with adolescents in private practice.
Methods
Design
We used semi-structured interviews with private psychologists’ to explore willingness to accept adolescent referrals.
Recruitment and sampling
Participant characteristics.
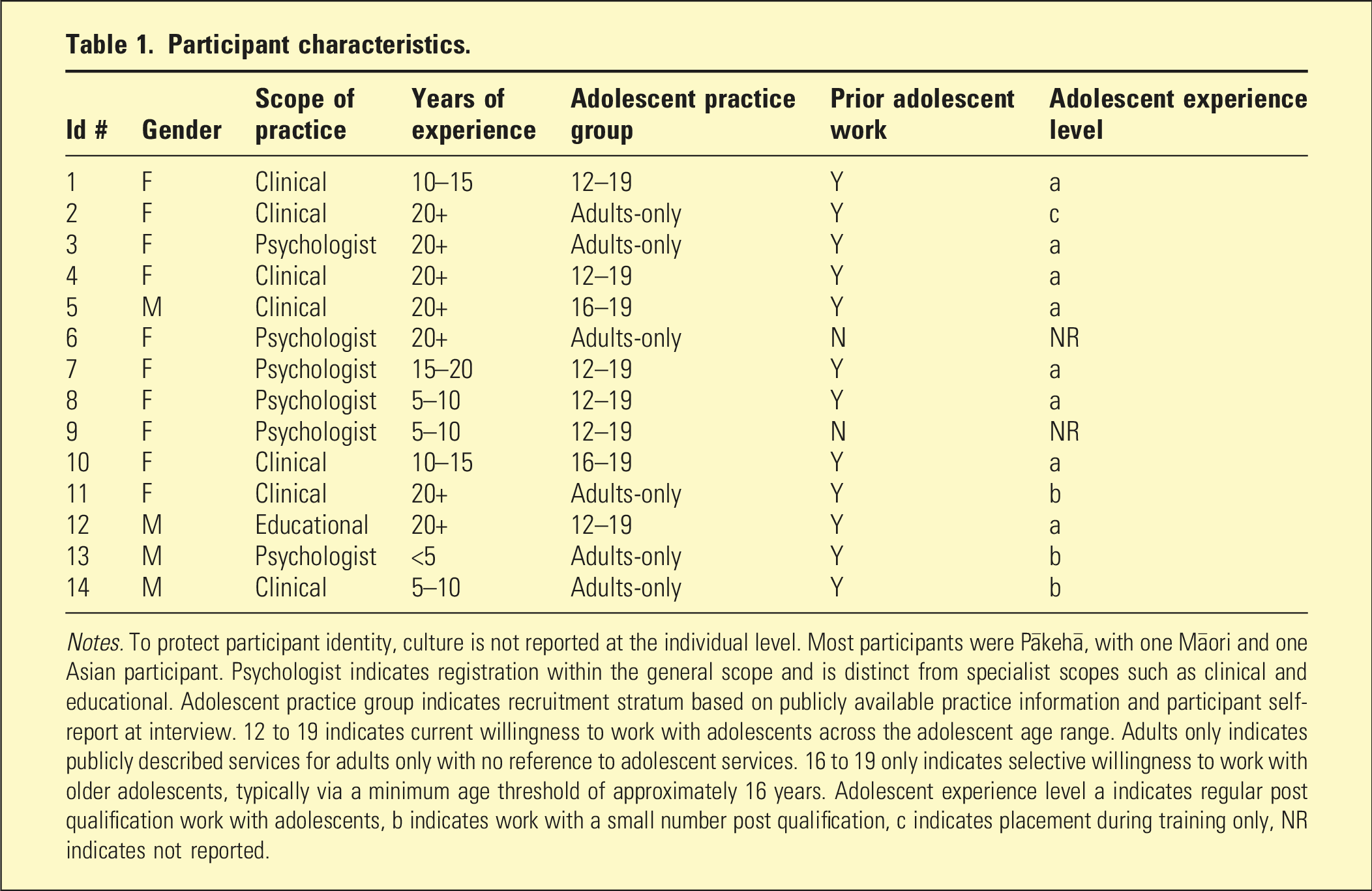
Notes. To protect participant identity, culture is not reported at the individual level. Most participants were Pākehā, with one Māori and one Asian participant. Psychologist indicates registration within the general scope and is distinct from specialist scopes such as clinical and educational. Adolescent practice group indicates recruitment stratum based on publicly available practice information and participant self-report at interview. 12 to 19 indicates current willingness to work with adolescents across the adolescent age range. Adults only indicates publicly described services for adults only with no reference to adolescent services. 16 to 19 only indicates selective willingness to work with older adolescents, typically via a minimum age threshold of approximately 16 years. Adolescent experience level a indicates regular post qualification work with adolescents, b indicates work with a small number post qualification, c indicates placement during training only, NR indicates not reported.
Procedure
Interviews were conducted by the first author via Microsoft Teams, recorded, transcribed and checked for accuracy. Participants received a NZ$30 voucher following the interview.
Data analysis
Data were analysed using reflexive thematic analysis with inductive semantic coding focused on considerations shaping acceptance, restriction or avoidance of adolescent referrals.
Rigour and reflexivity
Rigour was supported through reflexive journaling, an audit trail, and analytic discussions among authors (Susan Wall and Theresa Fleming).
Ethics
This study received ethical approval from the Victoria University of Wellington's Human Ethics Committee (Application ID 0000031034).
Results
Willingness varied across participants and reflected how adolescent work was appraised within private practice. In this study, willingness refers to openness to accepting adolescent referrals, while engagement refers to current adolescent practice. The findings show that willingness was shaped by both interest in adolescent work and judgements about its feasibility in private practice. Results are therefore organised around appraisals of interest and feasibility, followed by patterns of engagement, fluidity in participants’ perspectives, suggested leverage points, and an integrative summary.
Theme 1: Appraisals of interest
Interest in adolescent work reflected several related appraisals, including how participants understood adolescent reluctance, how emotionally comfortable they felt with young clients, whether the work fitted their therapeutic style, whether they expected to make a difference, and whether they viewed adolescent work as professionally valuable. These appraisals helped distinguish those who found adolescent work meaningful from those who experienced it as uncomfortable, unrewarding, or poorly aligned with their preferred practice.
Most participants, including those currently engaged with adolescents, described young clients as resistant or difficult to engage, often characterising them as ‘staunch, kind of surly’ (P8). Adolescents were frequently portrayed as reluctant therapy participants who ‘get dragged [to therapy] by the ear’ (P12). Participants actively engaged in adolescent work however, framed reluctance as developmentally normative and viewed engagement as the clinician’s responsibility. Adolescents were described as ‘just carrying so much’ (P7), and one participant noted that ‘it’s scary [for them] … to be relating to a psychologist’ (P9), and another noting they were ‘just big teddy bears underneath’ (P8).
Emotional comfort was a central factor. Those who found adolescent work meaningful described it as ‘immensely enjoyable … always touching and sometimes magical’ (P4). In contrast, less willing participants described fear or discomfort. One clinician found adolescent silence unsettling, stating ‘they’d be like me, and I didn’t have a lot to say’ (P2), while another linked avoidance to negative personal experiences parenting teenagers (P6).
Perceived fit also shaped interest. For some, adolescent work felt more appealing when it aligned with their preferred therapeutic style and role, and less appealing when it did not. Willing participants emphasised relational connection over technique, as illustrated by P12, ‘It’s 15% technique, 15% hope, and the rest is how we get on’. Effective engagement was associated with being ‘playful’ (P10), ‘authentic’ (P8), and ‘secure [within myself]’ (P7).
Participants also differed in expectations of therapeutic impact. Some were pessimistic, viewing family dynamics as immutable, where ‘making a difference’ (P11) felt beyond their control. Contrastingly, others believed adolescents could ‘just fly… if you provide them with what they need (P4).
Professional values were a further differentiator. Clinicians who engaged with adolescents often framed the work as preventative and ethically significant, stating ‘They deserve a fair chance’ (P8), while values-based framing was largely absent among those who avoided adolescent clients.
Theme 2: Appraisals of feasibility
Willingness also depended on feasibility appraisals. Feasibility reflected participants’ judgements about whether adolescent work could be delivered safely within private practice and sustained within a viable business model.
Clinical feasibility concerned whether adolescent work could be delivered safely within the psychologist’s competence and within a service context that could support risk management. Many participants described adult-focused training and limited structured preparation for adolescent work, contributing to uncertainty about what would count as adequate competence and scope. One participant commented that for ‘the Board to be satisfied … I would need to take a university course or significant PD [professional development]’ (P3). Others described ethical uncertainty around confidentiality, fee arrangements, and parental expectations, including discomfort in ‘taking their [parents’] money to work on something completely different to what they think or want me to’ (P13). These uncertainties were described as constraining willingness by increasing perceived professional and regulatory risk associated with adolescent work in private practice.
System fragmentation was also appraised as limiting confidence that risk could be shared or escalation could occur when needed. Clinicians described CAMHS ‘drop [ping] clients … like a hot potato’ when private clinicians were engaged (P11), which some interpreted as increasing individual responsibility for containment. Participants emphasised the absence of a reliable ‘holding framework’ beyond the private clinician, describing ‘no backup’ and limited outpatient or inpatient options unless a young person met very high thresholds (P4). Others linked this directly to felt practitioner safety, noting that when escalation pathways were unreliable ‘you just don’t feel safe … as a practitioner’ because they could not rely on ‘the next part of the system to step up … and support’ (P7). This lack of system backstop also contributed to clinicians holding cases beyond perceived fit: ‘you’re holding patients and you know you’re not the right person, but it’s the safest thing for them because there’s nowhere else… the system’s broken’ (P9). Participants further noted poor communication from public services and restricted access to psychiatric input, heightening uncertainty around assessment, diagnosis, medication questions, and escalation planning; one stated, ‘They didn’t even ask for my input [before making a diagnosis]’ (P1). Risk-sharing was rarely experienced as routine, and several emphasised clear boundaries, including that ‘I’m not a 24 hour crisis service’ (P8). Taken together, these conditions constrained feasibility by undermining clinicians’ confidence that adolescent work could be contained safely within private practice.
Practice feasibility concerned whether adolescent work could be sustained within the practical and economic conditions of private practice. Participants described adolescent work as emotionally demanding, with ‘no way you can get away from the pain and sadness’ (P12), and financially difficult where liaison with families and other services was unpaid. Some questioned the viability of this work within a fee-for-service model: ‘Who’s paying for that?’ (P5). These concerns were not usually framed as objections to adolescent work itself, but as limits on what could be sustained within private practice.
Theme 3: Patterns of engagement
Among participants who expressed at least some interest in adolescent work three patterns of engagement were identified, and these appeared shaped less by whether adolescent work was valued than by how feasible it was appraised as within private practice boundaries. Committed engagement (P1, P7, P8 and P12) involved sustained acceptance across adolescence, often supported by compensatory strategies to manage risk and coordination demand. Some of these clinicians emphasised relational and collegial scaffolding to contain complexity, as one put it, ‘I rely on my relationships [within CAMHS]’ (P1). Conditional engagement (P4, P5, P9 and P10) involved accepting adolescent work with deliberate constraints to keep it sustainable, most commonly through minimum age thresholds and caps on adolescent caseload, for example, ‘I don’t work with more than three adolescents at a time’ (P4). Disengaged engagement (P3 and P11) involved avoiding adolescent referrals altogether, typically where feasibility was appraised as too uncertain, with one participant describing difficulty accessing backup and uncertainty about ‘who or what was out there’, experienced as an ‘impassable barrier’ to adolescent work (P3).
Theme 4: Perspective fluidity
Notably, perspectives did not appear fixed. Three participants (P2, P10, P13) who had initially positioned themselves as unwilling to work with adolescents began to question the basis of that position during the interview. For example, P13 moved from low confidence to greater openness, concluding, ‘There’s no reason I couldn’t work with younger people that way’ (P13). P10 re-oriented toward adolescent work as preventative and as supporting adolescents to understand their ‘own inner world’ (P10), while P2 became more open but still expressed concern about regulatory risk: ‘I would be open to it … but I do not want to get in trouble’ (P2).
Participants’ perspectives on what could make a difference
Participants identified both developmental learning and structural supports as leverage points for strengthening sustainable engagement. Many expected that exposure to developmentally informed, relational models of adolescent work, including opportunities to observe practice, would increase confidence and clarify therapeutic leverage. Participants also emphasised supports that reduce isolation and distribute responsibility, including clearer referral pathways, consultation access, shared care arrangements, and workable coordination and escalation options across public and private services. Several identified timely access to psychiatric consultation as particularly important when risk increased or when diagnostic and medication questions arose.
Some participants added that clearer professional guidance and accessible PD on adolescent-specific practice dilemmas in private settings, including confidentiality, parental expectations, and fee-related tensions, could increase willingness by supporting safer and more confident engagement. Several further called for clearer profession-level guidance on scope and competence expectations for adolescent work in private practice.
Integrative summary
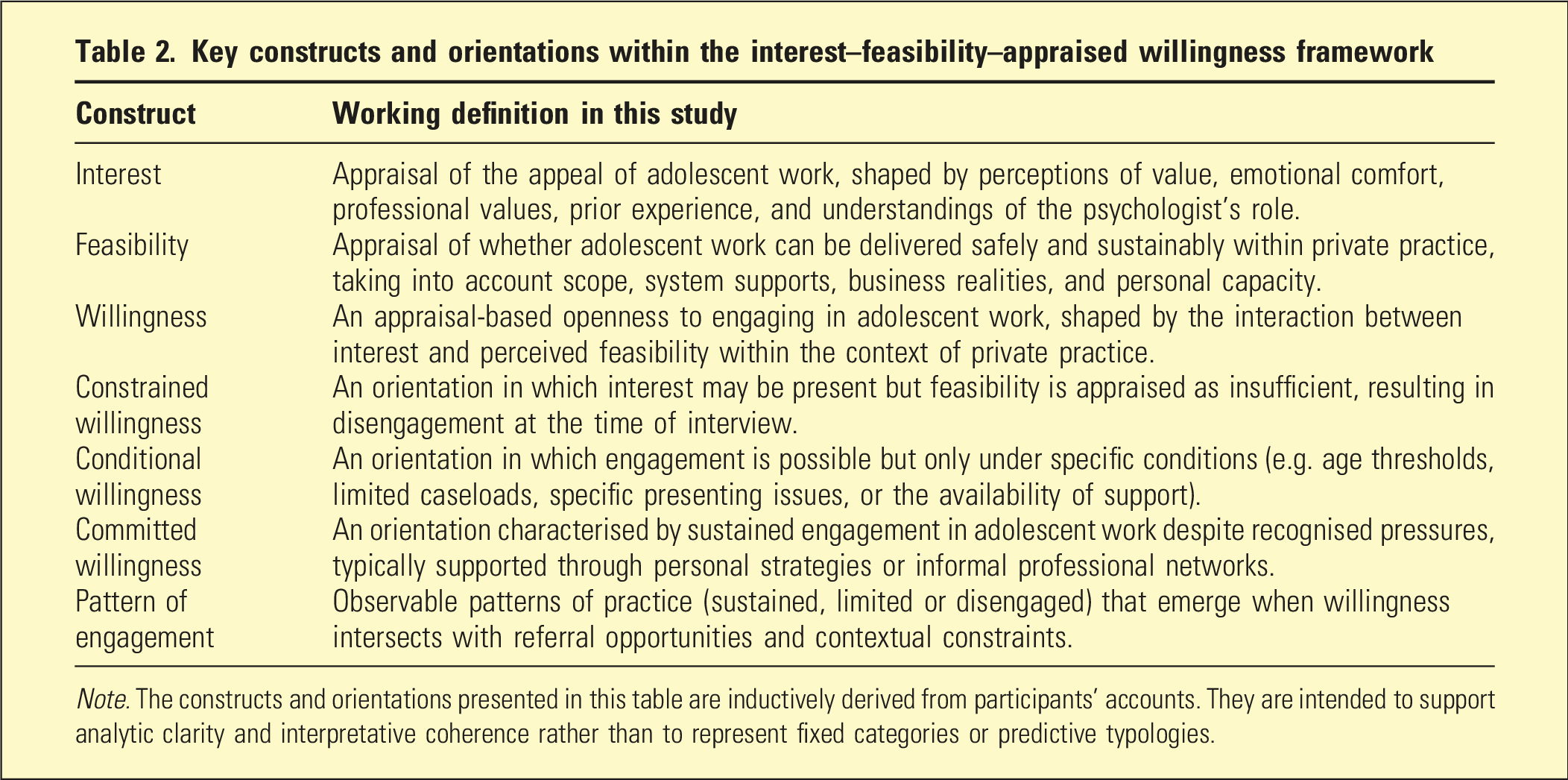
To synthesise these findings, an Interest Feasibility Appraised Willingness framework was developed in Figure 1, summarising clinicians’ patterns of adolescent practice within private settings. Definitions of key constructs are provided in Table 2. Interest-feasibility-appraised willingness framework. Note. Presents an integrative summary of the study’s findings, illustrating how willingness to engage in adolescent mental health work arises through clinicians’ appraisals of both interest and feasibility within the private practice context. Constructs used in the model are defined in Table 2. The willingness orientations (constrained, conditional and committed) represent descriptive patterns identified in participants’ accounts at the time of interview, rather than fixed categories or clinician types. Engagement patterns (sustained, limited and disengaged) reflect reported patterns of adolescent practice in relation to referral context, and are understood to be dynamic and potentially fluid over time. Key constructs and orientations within the interest–feasibility–appraised willingness framework Note. The constructs and orientations presented in this table are inductively derived from participants’ accounts. They are intended to support analytic clarity and interpretative coherence rather than to represent fixed categories or predictive typologies.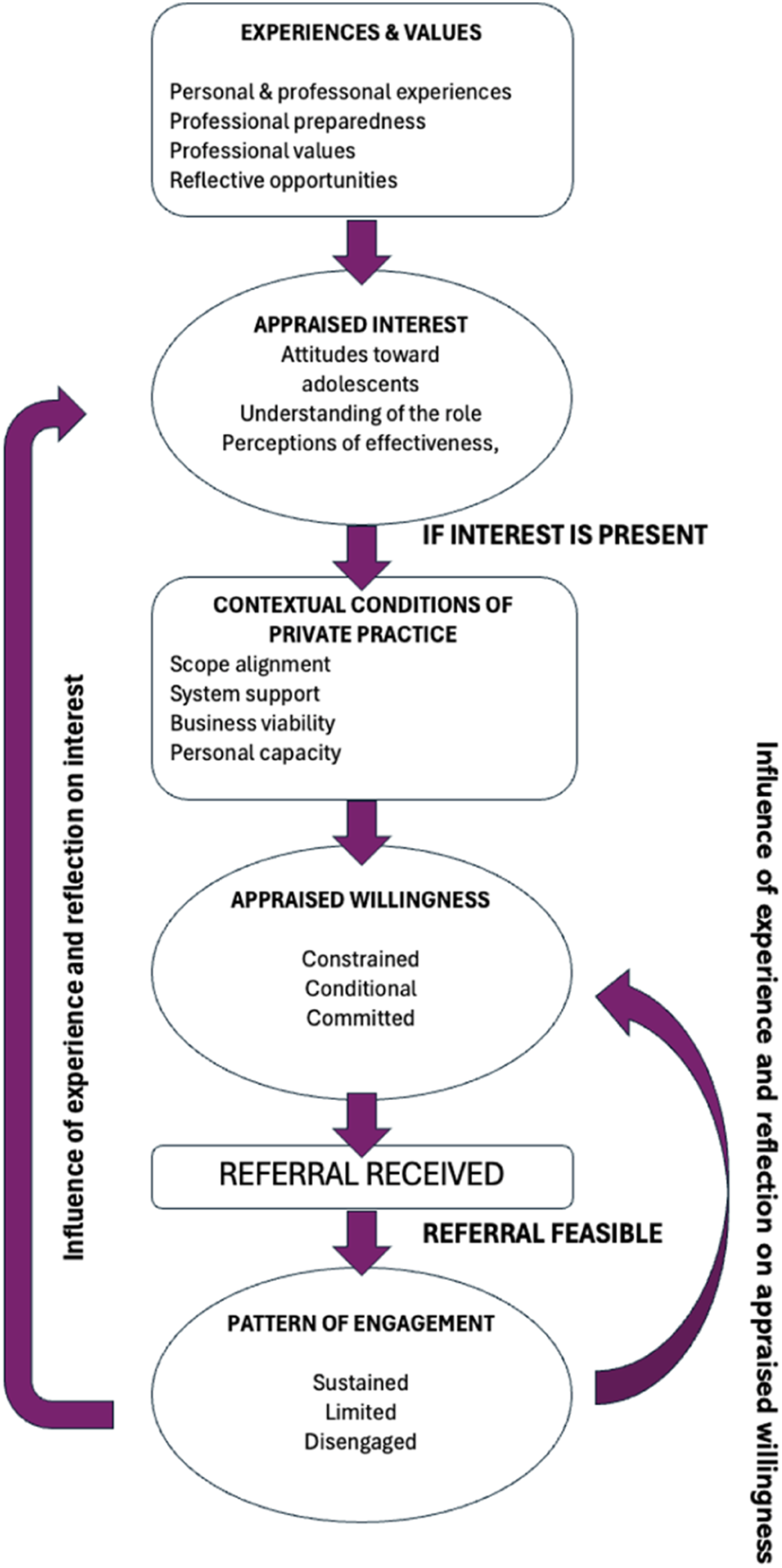
Discussion
This study examined factors shaping private psychologists’ willingness to engage in adolescent mental health work in Aotearoa. The central contribution is conceptual. Willingness is best understood not as a fixed preference or dispositional inclination, but as an appraisal-based openness emerging from the interaction between perceived interest and perceived feasibility within private practice conditions.
The findings extend literature on clinicians’ orientation toward particular client groups. Consistent with research in the older adult field,15–18 clinicians’ interest in adolescent work was shaped by anticipated relational difficulty, emotional comfort, and beliefs about therapeutic effectiveness. However, the present study suggests that in adolescent practice, interest is particularly sensitive to clinicians’ sense of therapeutic leverage in contexts characterised by variable readiness, family involvement, and developmental complexity. 12 Clinicians who framed reluctance as developmentally normative and engagement as a clinical task were more likely to sustain interest. Those who construed similar presentations as aversive, risky, or unlikely to yield meaningful change were more likely to withdraw. These findings reinforce the view that orientation toward a client group is shaped by interpretive stance and expectations of efficacy as much as by prior exposure.
The primary explanatory leverage of this study lies in how interest was filtered through feasibility. Even among clinicians who described adolescent work as meaningful or preventative, willingness was frequently contingent on whether it could be delivered safely and sustainably within private practice boundaries. This distinction aligns with implementation frameworks differentiating acceptability from feasibility as determinants of uptake and sustained delivery. 20 In this study, feasibility was shaped not only by competence concerns but by structural features of the wider service system, including fragmented communication, limited access to psychiatric consultation, unclear escalation pathways, and restricted opportunities for shared risk management.
Private practice emerged as a context in which autonomy is paired with concentrated responsibility. Clinicians exercised discretion over caseload composition yet also bore primary responsibility for risk containment, coordination, and business sustainability. 21 Where escalation pathways were perceived as unreliable and consultation supports limited, adolescent work was more likely to be appraised as high responsibility and therefore less feasible. Willingness thus depended not solely on interest but on confidence that clinical risk and system gaps could be shared beyond the individual practitioner.
In the context of the missing middle,22,23 constrained willingness within private practice may represent not merely workforce reluctance but a structural bottleneck in moderate complexity care. Adolescents whose needs exceed brief primary care input but do not meet specialist thresholds may be particularly affected when feasibility conditions limit private sector engagement. Limited participation therefore signals system design pressures as much as individual preference.
The finding that willingness shifted during interviews further supports the view that orientation toward adolescent work is not fixed. Reflection and reframing altered some participants’ positioning, echoing evidence that education and contact can modify clinician attitudes over time.24,25 However, feasibility concerns persisted across shifts, suggesting that strengthening interest alone is unlikely to substantially increase engagement where structural supports remain constrained.
Implications for strengthening professional engagement with adolescent work within private practice
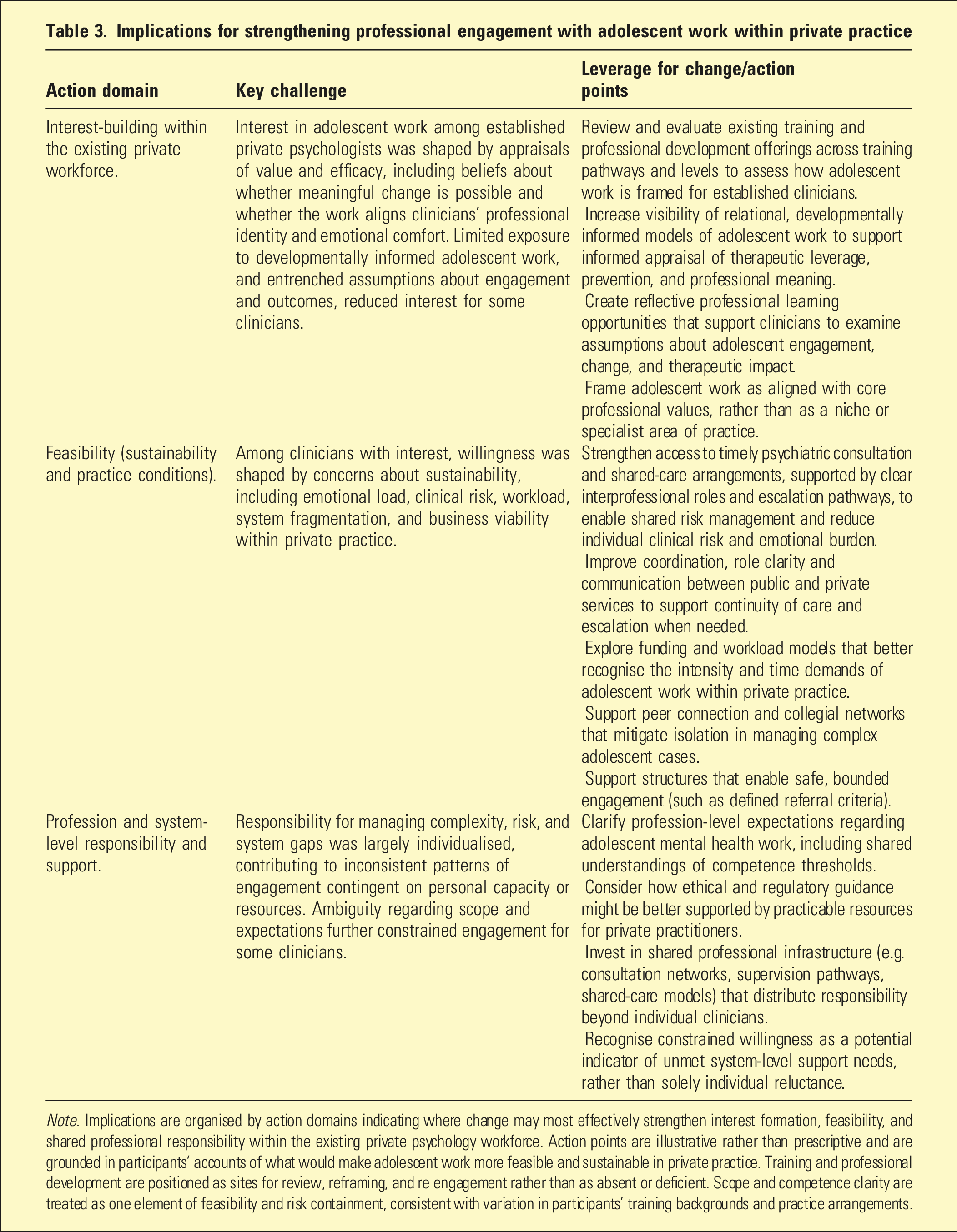
Note. Implications are organised by action domains indicating where change may most effectively strengthen interest formation, feasibility, and shared professional responsibility within the existing private psychology workforce. Action points are illustrative rather than prescriptive and are grounded in participants’ accounts of what would make adolescent work more feasible and sustainable in private practice. Training and professional development are positioned as sites for review, reframing, and re engagement rather than as absent or deficient. Scope and competence clarity are treated as one element of feasibility and risk containment, consistent with variation in participants’ training backgrounds and practice arrangements.
From a workforce and psychiatry perspective, the findings suggest that strengthening adolescent access may depend as much on collaborative infrastructure as on workforce supply. Clear escalation pathways, timely psychiatric consultation, improved cross sector communication, and profession level guidance regarding scope and competence may enhance feasibility appraisals and support more sustained engagement. Where responsibility for diagnostic complexity, medication decisions, and crisis escalation can be shared, private practitioners may experience adolescent work as more containable and sustainable.
Given documented inequities in youth mental health access in Aotearoa,3–5 variability in private sector engagement also has implications for equitable distribution of care. If participation is contingent on system containment rather than solely on interest, structural supports become not only workforce issues but equity issues.
More broadly, the Interest–Feasibility–Appraised Willingness framework conceptualises workforce participation as dynamic and modifiable when both motivational and structural dimensions are addressed. Recognising constrained willingness as a potential indicator of system level gaps, rather than solely individual avoidance, may enable more constructive policy responses.
Several limitations warrant consideration. This study reflects the perspectives of a purposively sampled group of private psychologists in one national context and cannot determine the prevalence of particular orientations across the wider workforce. Accounts represent appraisals rather than observed referral decisions, and willingness may fluctuate across time and changing system conditions. Future research could examine whether modifications in consultation access, shared care arrangements, or regulatory guidance are associated with measurable changes in referral acceptance patterns.
Despite these limitations, this study contributes an empirically grounded account of how established private psychologists make sense of adolescent referrals before engagement begins. By locating willingness at the intersection of interest and feasibility, the findings move beyond explanations centred solely on attitude or training and highlight the structural conditions that shape workforce participation. In doing so, the study offers a more nuanced basis for strengthening adolescent access within a mixed mental health system.
Conclusion
Private psychologists’ willingness to engage in adolescent mental health work in Aotearoa New Zealand is best understood as an appraisal-based process shaped by the interaction between interest and feasibility within private practice conditions. While many clinicians endorse adolescent work as meaningful and preventative, engagement becomes conditional when responsibility for risk, coordination, and system gaps is concentrated at the individual level. Limited participation therefore reflects structural constraints as well as professional preference. Strengthening adolescent access in mixed public and private systems may depend on enhancing shared consultation, escalation pathways, and cross sector collaboration so that responsibility for complexity is distributed rather than individualised. Recognising willingness as dynamic and context dependent offers a more constructive basis for workforce planning and service design.
Ethical approval
The Victoria University of Wellington’s Human Ethics Committee approved our survey (HEC Application ID 0000031034) on November 9, 2023.
Informed consent
Respondents were provided with a comprehensive information sheet, outlining the purpose and procedure of the study, their rights, and the likelihood of findings being published. They were ensured all data would be anonymised. Participation was voluntary, and participants submitted electronic consent prior to their interview.
Footnotes
Consent for publication
No consent was needed for publication as the data reported is anonymized, thereby protecting the privacy of all interviewees.
Author contributions
Susan Wall – Conceptualisation, formal analysis, investigation, methodology, project administration and writing.
Mathijs Lucassen – Conceptualisation, supervision and edit writing.
Theresa Fleming – Conceptualisation, supervision and review and edit writing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.