
Abstract
Objective
To examine the impact of the COVID-19 pandemic on adolescent psychiatric inpatient admissions by comparing sociodemographic, diagnostic, and clinical characteristics before and during the pandemic.
Methods
A Melbourne adolescent psychiatric inpatient unit admitted 963 adolescents during March–December 2019 (pre-pandemic) and March–December 2020 (pandemic). Comparisons of demographics, diagnoses, symptom severity and functioning (HoNOSCA, SDQ), and admission characteristics including restraint and seclusion were analysed.
Results
Admission volume increased by 17% while overall symptom severity remained stable. Personality and Autism Spectrum Disorder diagnoses increased, as did use of physical restraint and symptoms of hyperactivity, psychosis, and somatic complaints. Substance misuse decreased significantly. Most demographic variables were unchanged, except for a decline in Indigenous admissions. Effect sizes were small.
Conclusion
While concerns about increased mental health problems have been expressed during the pandemic period, adolescent admissions did not show increased symptom severity or functioning difficulties. The increased admission rate was accompanied by increases in only two diagnostic groups; possibly overlapping in heightened internal distress amid pervasive social disruption. That one vulnerable group – indigenous young people – had lower admission rates, may talk to stronger community supports or to further marginalisation from the health care system, during the pandemic.
Keywords
Mental illness and substance use are leading causes of disability in young people, accounting for nearly half of the global burden of disease in those aged 10–24 years. 1 Adolescence is a critical developmental period, during which early-onset psychiatric disorders can shape long-term health trajectories and affect future generations. 2
The COVID-19 pandemic and associated lockdowns created an unprecedented disruption to adolescent social, educational, and family environments. Young people are particularly vulnerable to such disruptions, given their reliance on peer relationships, schooling, and community supports.3–5 Evidence from previous public health crises suggests heightened risks of abuse, neglect, and mental health problems during periods of social restriction.4,6 Melbourne, Australia, experienced one of the world’s longest lockdowns, with restrictions lasting 262 days, raising concerns about its potential impact on youth mental health.7,8
Emerging international evidence has reported mixed effects of the COVID-19 pandemic on adolescent psychiatric presentations (see Appendix 1). Several studies have found increases in self-harm, anxiety, and eating disorder presentations,9,10 whereas others found stable or reduced rates of hospital attendance, 11 often attributed to service restrictions and help-seeking behaviour.12,13 However, most of this research has examined community or emergency department settings, and largely originates from North America and Europe, where lockdown measures were typically shorter and less restrictive than those in Victoria, Australia.
Consequently, little is known about how prolonged lockdowns affected the clinical profile, diagnostic complexity, and severity of adolescents requiring hospitalisation. Inpatient data offer a unique perspective on the most acute and complex presentations, complementing community-based research that may underestimate the pandemic’s impact on severe mental illness.
This present study addresses this gap by comparing sociodemographic, diagnostic, and clinical characteristics of adolescent psychiatric inpatient admissions before and during Victoria’s first 9 months of lockdown. By analysing diagnostic distributions, clinician- and self-reported symptom measures, and hospital variables such as restraint use, the study provides insight into how systemic disruptions may alter both the nature and severity of cases requiring hospital care.
Method
Design and setting
This retrospective cohort study analysed admissions to a 12-bed public adolescent inpatient psychiatric unit (AIPU) in metropolitan Melbourne, Australia. Admissions during the COVID-19 pandemic (1 March–31 December 2020) were compared with the equivalent pre-pandemic period in 2019. This timeframe was selected to capture the full duration of the most intense and disruptive lockdown phases, when access to education, social contact, and health services was most restricted. A matching pre-pandemic period was chosen to ensure temporal comparability and minimise seasonal confounding.
Ethics approval was obtained from the local Human Research Ethics Committee (Number withheld for anonymity).
Participants
There were 963 admissions aged 13 to 17 years from March 2019 to December 2020.
Data source and extraction
Data were extracted from the statewide psychiatric database (Client Management Interface, CMI), including sociodemographic variables (age, gender, Indigenous status, rurality), hospital characteristics (admission numbers, length of stay [LOS], seclusion, restraint use), and clinical measures (HoNOSCA, SDQ, and ICD-10 discharge diagnoses). Ten percent of cases were randomly audited against original records, with no discrepancies identified.
Measures
The Health of the Nation Outcome Scales for Children and Adolescents (HoNOSCA): Clinician-rated measure of psychological symptoms and functioning at admission, with demonstrated reliability and validity. 14
The Strengths and Difficulties Questionnaire (SDQ), Self- and parent-rated measure of emotional and behavioural functioning. 15 The Total Difficulties Score combines the Emotional, Conduct, Hyperactivity, and Peer Problems subscales and has satisfactory internal consistency and validity.15,16
Discharge diagnoses were recorded using ICD-10. Multiple principal diagnoses are regularly recorded for individual admissions in routine clinical practice. Specific diagnoses were grouped under the ICD-10 block headings, and a heuristic hierarchy was applied to determine the priority diagnosis (see Appendix). This approach prioritises a diagnostic group based on clinical severity and functional impact. 14 For example, an individual with personality, mood and adjustment disorder diagnoses would be grouped under the personality disorder category. This priority diagnostic hierarchy was used to avoid statistical inflation from multiple diagnostic categorisations and to enhance comparability across admissions.
Statistical analysis
An a priori power analysis (G*Power) indicated a required sample of 788 admissions to detect a small effect (Cohen’s d = 0.2, α = 0.05, power = 0.80). 17 Continuous variables were compared using independent-samples t-tests, and categorical variables with chi-square or binomial tests. Multivariate analysis of variance (MANOVA) with Bonferroni correction was used for HoNOSCA and SDQ subscales. As the SDQ has parent and youth versions, both were analysed. Analyses were conducted using IBM SPSS Statistics v27.
Results
Sociodemographic and admission variables
Comparison of sociodemographic and hospital admission variables.
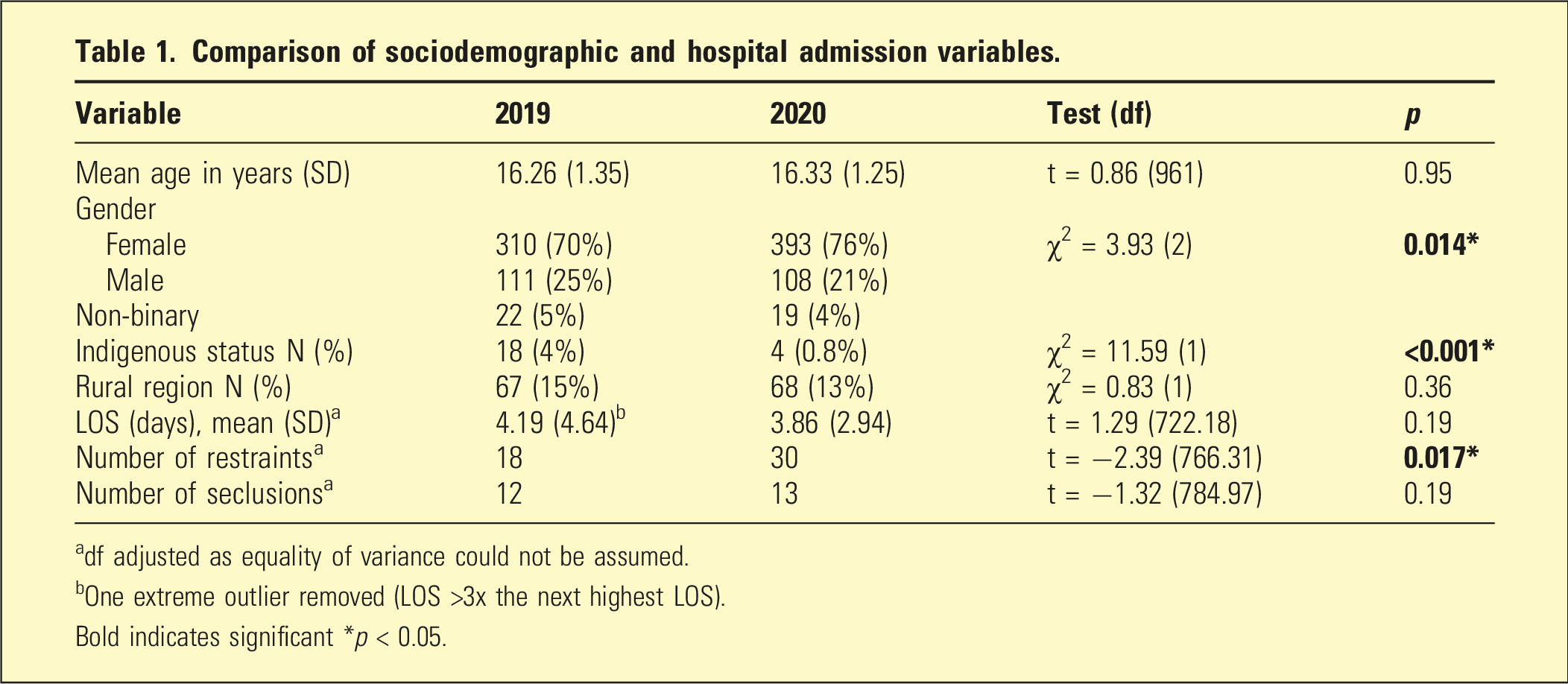
adf adjusted as equality of variance could not be assumed.
bOne extreme outlier removed (LOS >3x the next highest LOS).
Bold indicates significant *p < 0.05.
Further breakdown of physical restraints use by diagnostic category or number of individuals restrained was not possible, as episode-level data were not consistently linked to diagnostic entries in the statewide database.
With LOS, one outlier was three times longer than the next highest LOS. This extremely long admission, due in part to post-discharge placement problems, was excluded from the LOS analysis. Variance equality could not be assumed, and t-test parameters were adjusted accordingly (Table 1).
Diagnoses
Change in priority diagnoses (ICD-10).
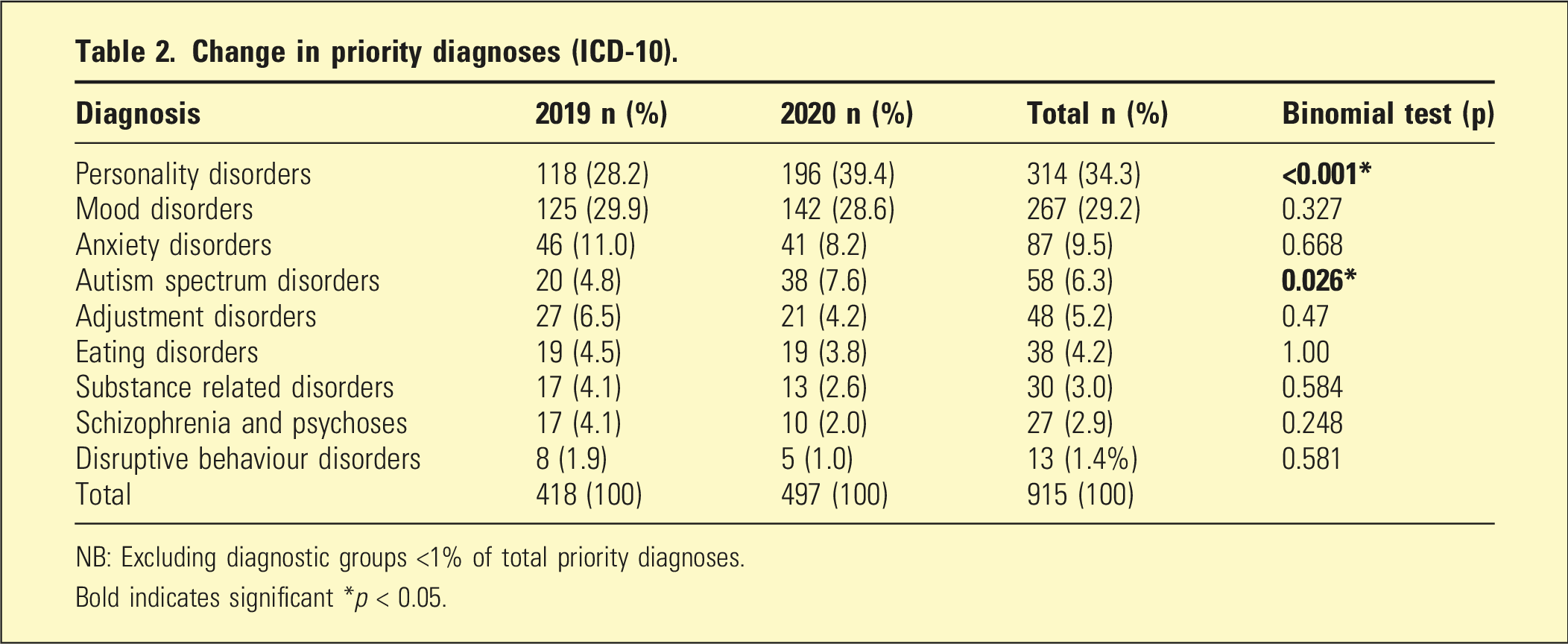
NB: Excluding diagnostic groups <1% of total priority diagnoses.
Bold indicates significant *p < 0.05.
Clinician-rated symptoms (HoNOSCA)
Comparison of mean (sd) HoNOSCA scales by year.
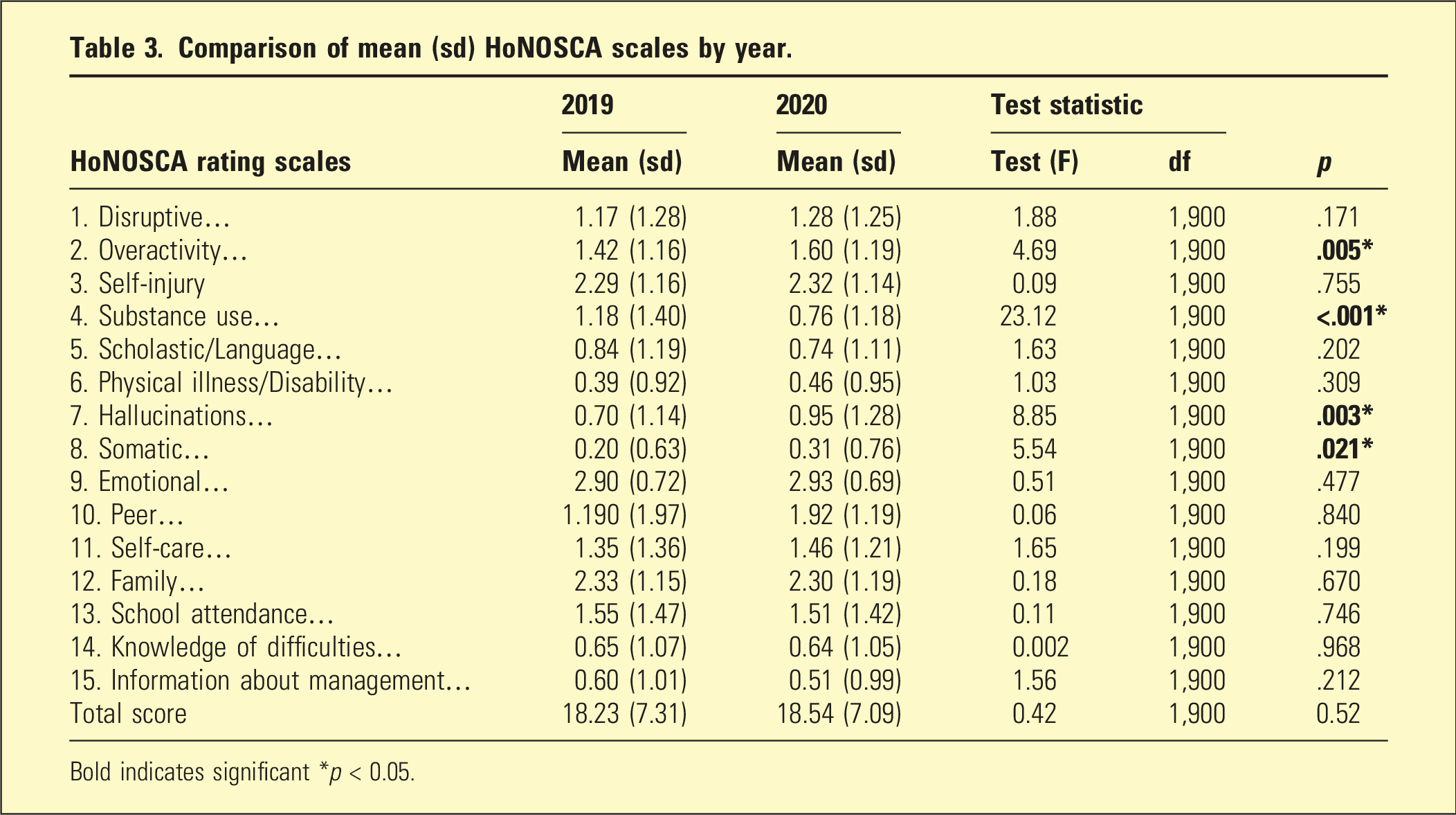
Bold indicates significant *p < 0.05.
Self-reported and parent-reported symptoms (SDQ)
Completion rates for SDQs were modest (2019 - youth 47%; parent ∼37%, 2020 – youth 45%, parent 35%. No significant differences were found in Total Difficulties Scores between years indicating neither parents nor young people perceived a change in the average level of difficulties (2019: m = 19.91, sd = 6.49.2020: m = 20.63, sd = 6.74). Using MANOVA to examine the four difficulties subscales, a significant difference was found between years (F = 2.62, df = 4,785, p < 0.05) and between young people and parents (F = 9.51, df = 4,785, p < 0.001). There was no interaction between informant and year. Follow up revealed that the only difference between years was an increase in Hyperactivity/Inattention difficulties (F = 8.04, df = 1,788, p < 0.001.2019: m = 6.19, sd = 2.37.2020: m = 6.69, sd = 2.52).
A supplementary finding was that, irrespective of year, young people rated themselves as having more severe difficulties than parents (F = 10.41, df = 1, 788, p < 0.001. Youth mean = 20.95, sd = 6.35; Parents mean = 19.44, sd = 6.89). This finding was repeated with the subscales where young people also reported more difficulties than parents in Hyperactivity/Inattention and in Peer Relationships across both years.
Where significant differences were identified, effect sizes (Cohen’s d for continuous variables and Cramer’s V for categorical comparisons) were calculated to indicate the magnitude of change; these were generally small, suggesting limited clinical impact despite statistical significance.
Discussion
This study is, to our knowledge, the first in Australia to examine the impact of the COVID-19 pandemic and associated lockdowns on AIPU. By comparing admissions during 2020 with the equivalent period in 2019, it provides a unique perspective on the most severe youth presentations requiring hospitalisation. Overall admission numbers increased whereas international reports showed no widespread rise in adolescent psychiatric hospitalisations during early COVID-19.18,19 While admissions increased, clinician’s, parent’s and young people’s perception of overall symptom and functioning remained stable. Adolescents admitted to hospital typically represent the most severe and complex presentations, suggesting both a possible ceiling effect for admission, and a potentially reduced capacity for the community to manage severe problems during the pandemic.
Clear diagnostic and symptom shifts were observed. The significant rise in PD aligns with literature highlighting the vulnerability of adolescents with borderline traits during COVID-19 (20). Disruptions to therapeutic alliances, peer relationships, and schooling likely contributed to heightened emotional instability and crisis presentations.20,21 Beyond individual vulnerabilities, broader family dynamics during lockdowns may also have contributed. Extended time spent at home during prolonged lockdowns likely increased family exposure to adolescents’ emotional and behavioural difficulties, prompting earlier recognition and, in some cases, lower tolerance for distress or dysregulation. Heightened parental stress, financial strain, and reduced access to community and respite supports may have further intensified family dynamics. These contextual factors may have influenced both the timing of hospital presentations and clinicians’ formulation of diagnoses, particularly for disorders characterised by interpersonal and emotional dysregulation. Many of these features could also have contributed to the increase in Autism Spectrum Disorders (ASD) admissions, although it is not clear whether this is confounded by the increasing community-based presentations of ASD over the last decade 22 .
No increase in eating disorder admissions was found, diverging from international evidence of escalating adolescent eating disorder presentations23,24 and from an Australian study. 25 This discrepancy may reflect local service pathways with medically unstable cases admitted to specialised paediatric eating disorder units/wards,26,27 or diagnostic overlap where disordered eating behaviours were coded under personality disorder features.28,29
The decline in substance misuse is consistent with studies showing reduced access to alcohol and illicit substances during lockdowns.30,31 While this reduction may have been protective in the short term, it raises questions about post-pandemic trajectories once access is normalised.
Increased hyperactivity was a notable and consistent finding across clinician-rated and self-reported measures, echoing international reports of worsening ADHD-related difficulties during the pandemic.32,33 Loss of daily routines, reduced opportunities for physical activity, and prolonged online learning may have amplified attentional and behavioural regulation problems in adolescents, particularly those with pre-existing vulnerabilities. 34 This finding underscores the importance of environmental structure and routine in managing hyperactivity, and highlights the need for targeted supports during periods of systemic disruption.
The rise in the use of physical restraints during the pandemic was interesting. This trend has also been observed in other inpatient settings during the pandemic. 35 Given that there was not higher severity in disruptive behaviours this may reflect the heightened challenges faced by staff working under the restrictive pandemic conditions. Importantly, this occurred during a period when physical distancing requirements limited close contact, potentially constraining the use of standard de-escalation strategies. This finding raises concern about the effectiveness and sustainability of de-escalation practices during times of systemic stress and underscores the need for additional staff training, reflective supervision, and organisational support to maintain trauma-informed and non-restrictive approaches even under crisis conditions.
Increased clinician-rated psychotic symptoms, without a parallel rise in formal psychotic disorder diagnoses, mirrors local reports of increased first-episode psychosis admissions in Melbourne. 36 This suggests dimensional measures such as the HoNOSCA may capture early shifts in severity not reflected in categorical diagnoses.
Finally, the decrease in Indigenous admissions is concerning and warrants cautious interpretation. The dataset did not include information to differentiate whether this reduction reflected barriers to accessing inpatient care during lockdowns, 37 or protective factors arising from strengthened family and community supports. 38 Both possibilities are plausible. Lockdowns and service restrictions may have compounded pre-existing access barriers for Aboriginal and Torres Strait Islander young people, including mistrust of mainstream services, reduced outreach, or geographic isolation. Conversely, some communities have reported strengthened kinship support and culturally grounded coping responses during the pandemic, which may have reduced the need for hospitalisation. Without more granular data, these explanations remain speculative. This finding nonetheless highlights the importance of culturally safe service design and the need to ensure equitable access to care during public health crises. Further investigation comparing outcomes across other cultural and racial groups would assist in determining whether inequities were specific to Indigenous populations or reflected broader systemic disparities in service reach and responsiveness.
Self- and parent-reported data (SDQ) showed no change in functional difficulties and complexity between the pre-pandemic and pandemic periods, consistent with stable clinician-rated severity. While complexity may have changed within community settings, neither parents, adolescents nor clinicians observed an overall change in this tertiary AIPU. A supplementary finding revealed an increase in over activity/inattention that was noted by parents, adolescents, and clinicians. In times of social restriction, the AIPU could be considered an island of face-to-face interactions.
These findings have several implications for service planning. Aboriginal and Torres Strait Islander young people, a high-risk group, had fewer admissions during the pandemic. It may be that periods of social crisis require additional engagement strategies to maintain accessibility for vulnerable groups. Secondly, increased admissions alongside a requirement to achieve social distancing with the adolescents created additional pressures within the AIPU. Achieving increased social distancing required more active staff intervention. The observed rise in restraint use may be partly consequent to this shift in the milieu rather than simply an increase in admissions with disruptive behaviours. Forward planning addressing increased social restrictions without exacerbating aggressive interactions may be prudent.
Finally, the increase in PD and in ASD admissions raises the question of flexibility in service response. For example, young people with ASD may have been particularly vulnerable to the disrupted routines and supports during lockdowns, while the reliability of the interpersonal relationships of those with a PD may have been impacted by the pandemic. How an inpatient unit could alter its’ therapeutic approach to a changing diagnostic profile, let alone account for the pandemic impact, is a complex matter for consideration. While treatment and milieu approaches were not examined, the question of therapeutic flexibility remains important in achieving a patient-focussed unit.
Ongoing monitoring is required to detect shifts in adolescent presentations, and planned treatment modules should be identified that can respond. Longer term research may distinguish temporary pandemic effects from enduring service needs, but that will not diminish the need to respond to respond appropriately to the short-term changes.
Strengths and limitations
This study has several strengths. First, it used a large, unselected cohort of 963 admissions, providing robust statistical power and ensuring findings reflect the full inpatient population. Second, data were drawn from routine clinical records across multiple domains, including sociodemographic, diagnostic, and clinical measures, as well as hospital variables. The inclusion of clinician-rated (HoNOSCA) and youth- and parent-reported (SDQ) outcomes offered a multi-informant perspective on clinical severity. Data quality was further supported by an audit of 10% of cases, which confirmed accuracy and completeness. Together, these factors enhance the reliability and ecological validity of the findings.
Several limitations should also be acknowledged. The retrospective observational design restricts causal inference, limiting conclusions to associations rather than direct effects of the pandemic. The study was conducted at a single metropolitan unit in Melbourne, a city with the longest cumulative lockdown globally, and findings may not generalise to other settings with different restrictions or service structures. Diagnostic categories were based on clinician judgement at discharge rather than structured diagnostic interviews, which may introduce variability.
Although the priority diagnostic approach has precedence in Australian outcome-measure reporting, and is transparent, the specific hierarchy has not been formally validated. It is unlikely that many would place an Adjustment Disorder as more severe than an Eating Disorder, though there may be disagreement about ASD severity compared with Eating Disorders. There has been debate about Personality Disorder diagnoses in adolescents, 39 and while assigning the highest priority to Personality Disorder will not have amplified its frequency, it will impact on describing diagnoses lower in the hierarchy. Services that are more reluctant to diagnose Personality Disorder will of course describe a different diagnostic mix. Without some prioritising, diagnoses are likely to be over counted or misinterpreted (e.g. On a diagnostic number count, psychosocial factors will appear to be the highest diagnostic group in an AIPU).
Completion rates for the SDQ were modest, particularly for parents, reducing the representativeness of these self-reported data.
Also, the study period captured only the first 10 months of the pandemic, meaning delayed or longer-term trends in adolescent mental health may not have been observed. Data preceding 2019 were not available for analysis, limiting the ability to determine whether observed differences reflected pre-existing trends or pandemic-specific effects.
Finally, while the heuristic diagnostic hierarchy provided a practical means of managing multiple discharge diagnoses, it has not been formally validated. It also apparent that the specific hierarchy applied could be modified. For example, there has been debate about the validity of the personality disorder diagnosis in adolescent populations 39 and this could lead to a promotion or demotion of this group. Having personality disorders at the top of the hierarchy will not have amplified its relative frequency, but it will have an impact on describing diagnoses lower in the hierarchy. Furthermore, while every diagnosis did occur in routine clinical practice, it is acknowledged that not all services may be as comfortable in diagnosing personality disorder in adolescents.
Whether the observed changes reflected continuations of pre-existing trends requires an extended research study.
Conclusion
Adolescent psychiatric inpatient admissions did increase during the COVID-19 pandemic, but this was not accompanied by a rise in overall symptom severity. The clinical profile showed more Personality and Autism Spectrum Disorders, increased hyperactivity, and restraint use, alongside reduced substance-misuse and fewer Indigenous admissions.
The rise in restraint at a time of increased volume and stable acuity may have been influenced by the demand for physical distancing rather than behavioural challenges amongst adolescents.
These results suggest that the changes during the pandemic were different to what was discussed in community settings. Ongoing monitoring is more important than ever at an AIPU to ensure appropriate interventions and that marginalised groups are not left behind during a pandemic.
Supplemental material
Supplemental material – The impact of the COVID-19 pandemic on admissions to an adolescent inpatient psychiatric unit
Supplemental material for The impact of the COVID-19 pandemic on admissions to an adolescent inpatient psychiatric unit by Thomas Klug, Sarah Latowicz, Stanley Innes, Paul Robertson, Peter Brann in Australasian Psychiatry
Footnotes
Ethical considerations
Ethics approval was obtained from the Eastern Health Human Research Ethics Committee (LR21-036-77,798). Informed consent was waived by the Eastern Health Ethics Committee.
Author contributions
PB was responsible for the study design, literature search, data extraction, first draft and subsequent reviews. SL & TK were responsible for literature search, data extraction, data analysis, PCS scoring, initial draft and subsequent reviews. PR for review of drafts. SI was responsible for data review, first writeup and reviews.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data Availability Statement
The data that support this study is available on request and approval from the Eastern Health HREC.
Supplemental material
Supplemental material is available online.
Note
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.