To highlight the medical, legal, and ethical complexities of voluntary assisted dying (VAD) particularly for patients with mental illness, specifically within the state of New South Wales in Australia, and explore the role Psychiatrists involved in VAD may play, including clarifying uncertainty relating to issues of capacity, the characteristics of the patient requesting VAD, the condition underpinning the request for VAD, and the VAD request itself, through three hypothetical case studies.
Conclusion
It is essential that Psychiatrists understand their obligations under the VAD regime within their jurisdiction. VAD, particularly in vulnerable populations such as those with mental illness, presents numerous clinical challenges and is best addressed with a consensus-based approach to complex cases drawing on relevant expertise.
While Courts have retained ultimate authority over questions of capacity to make decisions regarding medical treatment and the scope of newly implemented VAD regimes in Australia, in practice medical practitioners will primarily undertake these tasks.1,2 This article seeks to assist Psychiatrists attempting to navigate this emerging area of law and medical practice by highlighting some of the challenges that may be encountered, specifically when assessing patients with a mental illness who apply for VAD under New South Wales (NSW) legislation in Australia. While a mental illness is not an eligible condition to ground a request for VAD in Australia, neither does it preclude access, though it may add complexity to the assessment process.1,3 Three hypothetical cases will illustrate clinical challenges broadly grouped as characteristics relating to the person making the VAD request; characteristics relating to the VAD request itself; and characteristics relating to the condition underpinning the VAD request. The cases highlight several challenges within VAD for a person with comorbid mental illness, including capacity and the interplay between suicidal ideation and mental illness; the confounding factor of demoralisation; and potential issues delineating mental illness from physical sequelae in cases of terminal anorexia nervosa. It advocates the importance of an individualised, multidisciplinary outlook utilising relevant expertise to reach a consensus-based approach to challenging cases, consistent with NSW VAD legislation.4
Medical, legal, and ethical complexities in VAD
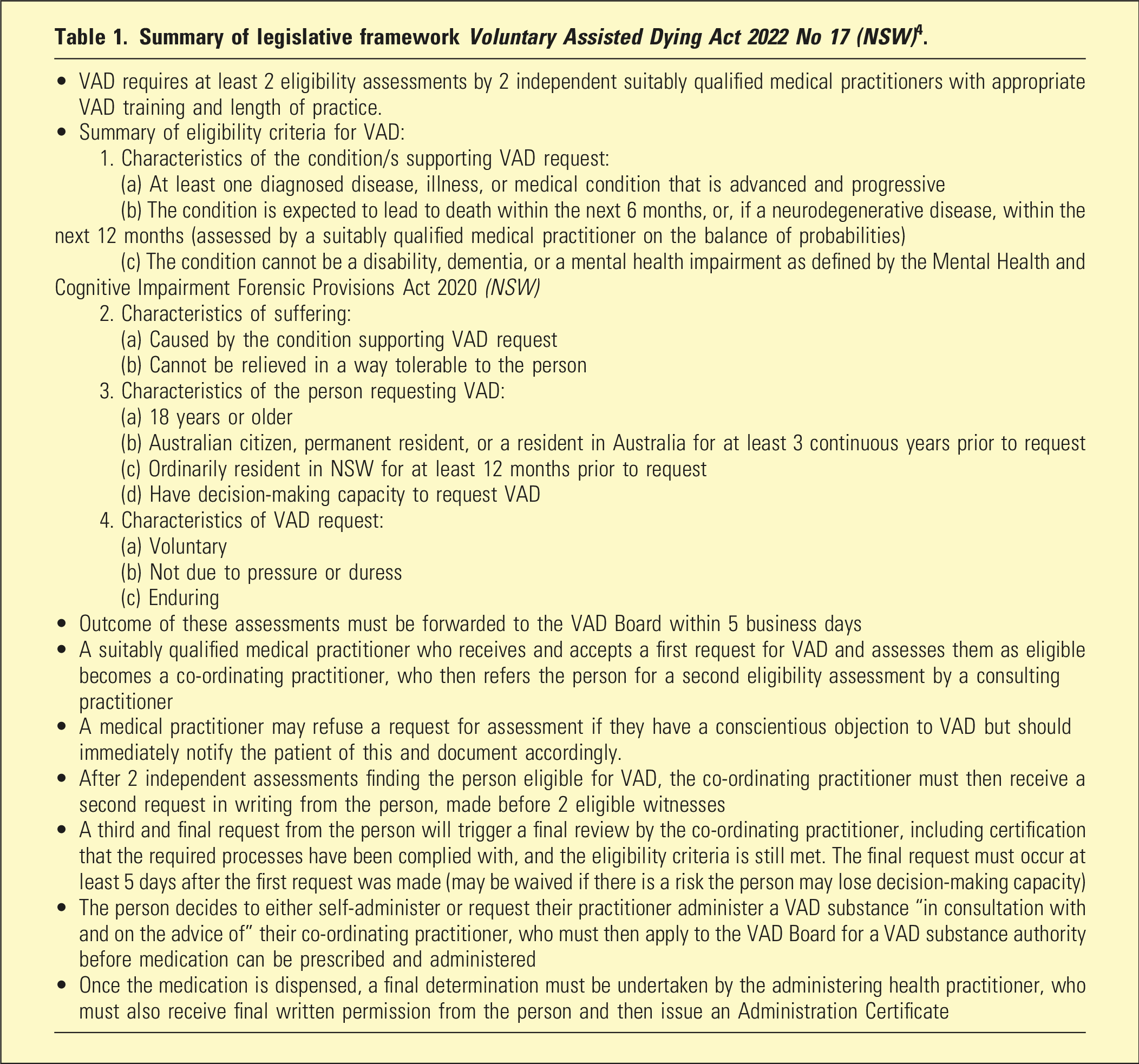
VAD represents a complex tapestry of ethical considerations often interwoven in tension.5 Primarily, VAD movements have foregrounded individual autonomy, dignity, and relief from suffering, whilst medical professional associations in Australia and internationally have expressed concerns regarding conflict between a physician’s direct involvement in ending a patient’s life and their fundamental role as healer.6–9 Additional concerns include managing risk of undue influence or coercion for vulnerable patients, the right of physicians to refuse to participate in VAD, and the need to ensure appropriate resourcing of palliative care options.7,8 The role Psychiatrists are likely to play in complex cases, such as where a patient has a mental illness, and uncertainty in distinguishing this from multifaceted distress often accompanying terminal illness, has also been highlighted.6 In Australia, these anxieties have translated into a tightly regulated VAD process with multiple procedural safeguards and relatively narrow eligibility criteria compared with (particularly European) models internationally.10–12 However, this calibration in turn raises concerns regarding equality of access to VAD.1,12 A brief outline of the legal framework for VAD in NSW is provided in Table 1.
Summary of legislative framework Voluntary Assisted Dying Act 2022 No 17 (NSW)4.
• VAD requires at least 2 eligibility assessments by 2 independent suitably qualified medical practitioners with appropriate VAD training and length of practice.
•Summary of eligibility criteria for VAD:
1. Characteristics of the condition/s supporting VAD request:
(a) At least one diagnosed disease, illness, or medical condition that is advanced and progressive
(b) The condition is expected to lead to death within the next 6 months, or, if a neurodegenerative disease, within the next 12 months (assessed by a suitably qualified medical practitioner on the balance of probabilities)
(c) The condition cannot be a disability, dementia, or a mental health impairment as defined by the Mental Health and Cognitive Impairment Forensic Provisions Act 2020 (NSW)
2. Characteristics of suffering:
(a) Caused by the condition supporting VAD request
(b) Cannot be relieved in a way tolerable to the person
3. Characteristics of the person requesting VAD:
(a) 18 years or older
(b) Australian citizen, permanent resident, or a resident in Australia for at least 3 continuous years prior to request
(c) Ordinarily resident in NSW for at least 12 months prior to request
(d) Have decision-making capacity to request VAD
4. Characteristics of VAD request:
(a) Voluntary
(b) Not due to pressure or duress
(c) Enduring
• Outcome of these assessments must be forwarded to the VAD Board within 5 business days
• A suitably qualified medical practitioner who receives and accepts a first request for VAD and assesses them as eligible becomes a co-ordinating practitioner, who then refers the person for a second eligibility assessment by a consulting practitioner
• A medical practitioner may refuse a request for assessment if they have a conscientious objection to VAD but should immediately notify the patient of this and document accordingly.
• After 2 independent assessments finding the person eligible for VAD, the co-ordinating practitioner must then receive a second request in writing from the person, made before 2 eligible witnesses
• A third and final request from the person will trigger a final review by the co-ordinating practitioner, including certification that the required processes have been complied with, and the eligibility criteria is still met. The final request must occur at least 5 days after the first request was made (may be waived if there is a risk the person may lose decision-making capacity)
• The person decides to either self-administer or request their practitioner administer a VAD substance “in consultation with and on the advice of” their co-ordinating practitioner, who must then apply to the VAD Board for a VAD substance authority before medication can be prescribed and administered
• Once the medication is dispensed, a final determination must be undertaken by the administering health practitioner, who must also receive final written permission from the person and then issue an Administration Certificate
Challenges regarding characteristics of the person requesting VAD: depression and terminal illness
Encountering a patient requesting VAD who also has depression, whether previously diagnosed or newly suspected, is likely given high rates of depression amongst people who are terminally ill.1,13 In such cases, close attention would be required to the issue of capacity, as symptoms of depression can involve adverse cognitive effects, including an overly negative future outlook, though research suggests clinicians overestimate this effect.14,15
Given capacity assessment in the VAD legislation adopts the same function-based criteria used in other areas of healthcare decision making, there is already an established body of medical practice and jurisprudence in Commonwealth countries that Psychiatrists may reference.
The starting point for any capacity assessment must be that the person is presumed to have capacity, unless there is evidence to displace this presumption. This is not achieved by simply making a diagnosis of depression or any other mental illness, with the Supreme Court of Victoria endorsing:
“The temptation to base a judgement of a person’s capacity upon whether they seem to have made a good or bad decision, and in particular upon whether they have accepted or rejected medical advice, is absolutely to be avoided…Any tendency in this direction risks infringing the rights of that group of persons who, though vulnerable, are capable of making their own decisions. Many who suffer from mental illness are well able to make decisions about their medical treatment, and it is important not to make unjustified assumptions to the contrary”(16p.7).
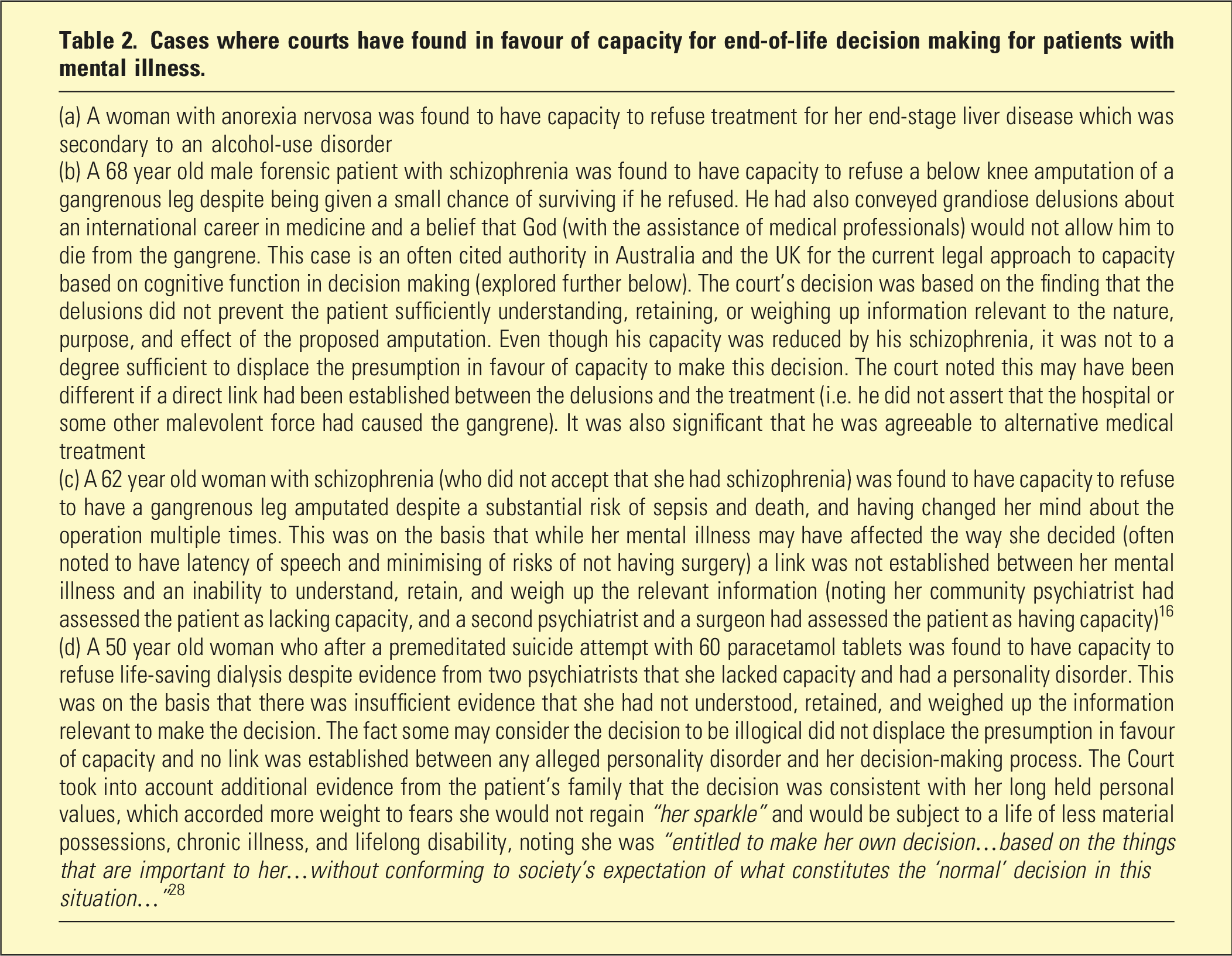
In contrast, studies suggest a significant proportion of clinicians, including Psychiatrists, instead apply a presumption that people with a mental illness necessarily lack capacity by virtue of having that diagnosis.14,15 The pitfalls of assuming a patient with mental illness will necessarily lack capacity to make decisions involving end-of-life treatment are illustrated by the situations outlined in Table 2 where courts applying similar principles about capacity to those contained in NSW VAD legislation have found in favour of the patient having capacity. The Victorian Supreme Court has referred favourably to the approaches taken by the courts in cases (b) to (d) in Table 2, describing them as “…notable for applying the capacity test in a way that is criteria focused, evidence based, patient centred and non-judgemental” (17p.66).
Cases where courts have found in favour of capacity for end-of-life decision making for patients with mental illness.
(a) A woman with anorexia nervosa was found to have capacity to refuse treatment for her end-stage liver disease which was secondary to an alcohol-use disorder
(b) A 68 year old male forensic patient with schizophrenia was found to have capacity to refuse a below knee amputation of a gangrenous leg despite being given a small chance of surviving if he refused. He had also conveyed grandiose delusions about an international career in medicine and a belief that God (with the assistance of medical professionals) would not allow him to die from the gangrene. This case is an often cited authority in Australia and the UK for the current legal approach to capacity based on cognitive function in decision making (explored further below). The court’s decision was based on the finding that the delusions did not prevent the patient sufficiently understanding, retaining, or weighing up information relevant to the nature, purpose, and effect of the proposed amputation. Even though his capacity was reduced by his schizophrenia, it was not to a degree sufficient to displace the presumption in favour of capacity to make this decision. The court noted this may have been different if a direct link had been established between the delusions and the treatment (i.e. he did not assert that the hospital or some other malevolent force had caused the gangrene). It was also significant that he was agreeable to alternative medical treatment
(c) A 62 year old woman with schizophrenia (who did not accept that she had schizophrenia) was found to have capacity to refuse to have a gangrenous leg amputated despite a substantial risk of sepsis and death, and having changed her mind about the operation multiple times. This was on the basis that while her mental illness may have affected the way she decided (often noted to have latency of speech and minimising of risks of not having surgery) a link was not established between her mental illness and an inability to understand, retain, and weigh up the relevant information (noting her community psychiatrist had assessed the patient as lacking capacity, and a second psychiatrist and a surgeon had assessed the patient as having capacity)16
(d) A 50 year old woman who after a premeditated suicide attempt with 60 paracetamol tablets was found to have capacity to refuse life-saving dialysis despite evidence from two psychiatrists that she lacked capacity and had a personality disorder. This was on the basis that there was insufficient evidence that she had not understood, retained, and weighed up the information relevant to make the decision. The fact some may consider the decision to be illogical did not displace the presumption in favour of capacity and no link was established between any alleged personality disorder and her decision-making process. The Court took into account additional evidence from the patient’s family that the decision was consistent with her long held personal values, which accorded more weight to fears she would not regain “her sparkle” and would be subject to a life of less material possessions, chronic illness, and lifelong disability, noting she was “entitled to make her own decision…based on the things that are important to her…without conforming to society’s expectation of what constitutes the ‘normal’ decision in this situation…”28
Given the gravity of the decision to access VAD, a clinician should undertake a rigorous assessment of capacity.1,3 Section 38 of the NSW VAD Act4 provides that if a consulting practitioner is unsure about a patient’s decision-making capacity in relation to VAD, or due to a past or current mental illness, they must make a referral to a Psychiatrist or “another registered health practitioner or person who has appropriate skills and training to make a decision about the matter.”
Consultant Liaison Psychiatrists have long grappled with detangling mental illness from the psychological or existential distress of demoralisation that often accompanies medical conditions such as cancer, where the illness or its treatment causes symptoms including fatigue, weight loss, and reduced appetite. Considered “a normal response to adversity,” demoralisation is clinically significant psychological distress that does not meet the threshold for a psychiatric disorder like depression, anxiety, or adjustment disorder. It is characterised by fear, sadness, or low mood; inability to cope; feelings of futility and low self-worth due to being unable to accomplish things that give life meaning for the person. It is distinguished from depression by the absence of anhedonia.18,19
Suicidality provides another complicating factor given its association with mental illness.20 However, the majority of people with a mental illness do not commit suicide, and suicidality can also be present in the absence of any mental disorder.20 If the person has a history of previous or current suicidal ideation, the usual clinical approach to assessing suicidal ideation should be used, including consideration of any active intent or plan. Risk factors including social isolation and substance use should be considered and if acute risk identified, for example, concerns the patient is in fact acutely suicidal, usual management implemented.20 Courts have commented that doctors have the skills to distinguish between suicide and VAD.21 However, efforts to impose rigid categories distinguishing suicidal ideation from requests for VAD (see, e.g. “Statement of the American Association of Suicidology”22 which identifies factors like motivation, methods used, and impulsivity) have encountered similar difficulties as the efforts to convert population-level risk factors for suicide to statistically meaningful tools, which have so far proven of limited clinical utility.20
The Psychiatrist’s documentation should make clear their assessment is based on considering the extent to which the patient meets the criteria in the function-based test for capacity contained in the NSW VAD Act. To the extent depression is relevant, it is by considering any direct link between the symptoms and the patient’s functional abilities in decision making (such as understanding, retaining, and weighing relevant information) set out in the statutory criteria for capacity that applies to all applicants. The Courts have repeatedly highlighted their concern that a capacity assessment based on any other approach is likely to discriminate against people with mental illness.1,2
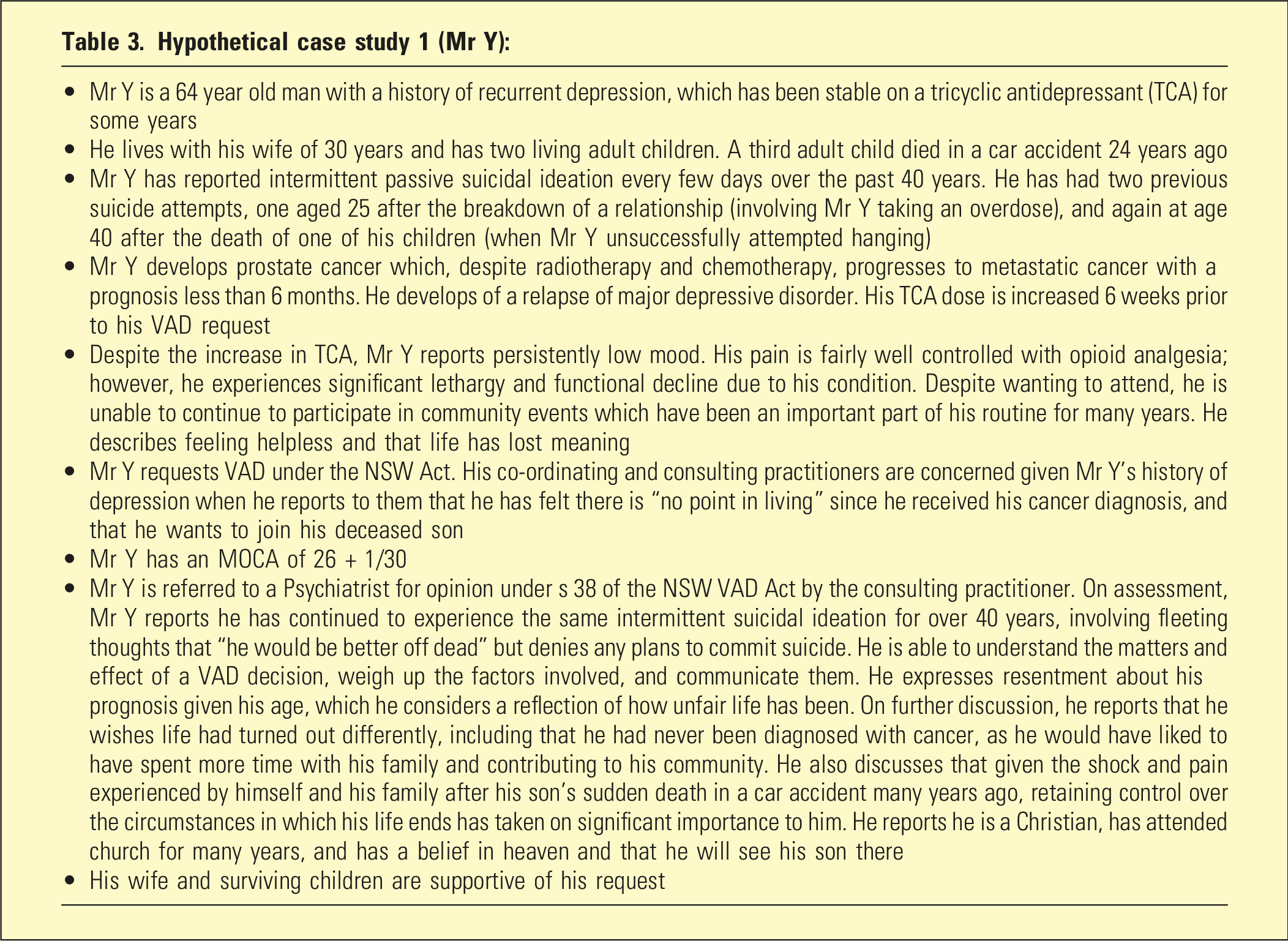
Close attention to the patient’s subjective “values, attitudes and relationships” has also been emphasised as a “reference point” as these can often provide overlooked evidence of capacity.2 This is echoed in the principles of the NSW VAD Act4 and some of the court decisions outlined above where capacity was found after close scrutiny to individual circumstances of the case, including evidence from non-clinicians (family) as to these values, even if this contradicted views from medical practitioners including Psychiatrists.2 Similarly in Table 3, assessment of Mr Y revealed his VAD request was consistent with his personal values and of a different character to his previous suicide attempts.
Hypothetical case study 1 (Mr Y):
• Mr Y is a 64 year old man with a history of recurrent depression, which has been stable on a tricyclic antidepressant (TCA) for some years
• He lives with his wife of 30 years and has two living adult children. A third adult child died in a car accident 24 years ago
• Mr Y has reported intermittent passive suicidal ideation every few days over the past 40 years. He has had two previous suicide attempts, one aged 25 after the breakdown of a relationship (involving Mr Y taking an overdose), and again at age 40 after the death of one of his children (when Mr Y unsuccessfully attempted hanging)
• Mr Y develops prostate cancer which, despite radiotherapy and chemotherapy, progresses to metastatic cancer with a prognosis less than 6 months. He develops of a relapse of major depressive disorder. His TCA dose is increased 6 weeks prior to his VAD request
• Despite the increase in TCA, Mr Y reports persistently low mood. His pain is fairly well controlled with opioid analgesia; however, he experiences significant lethargy and functional decline due to his condition. Despite wanting to attend, he is unable to continue to participate in community events which have been an important part of his routine for many years. He describes feeling helpless and that life has lost meaning
• Mr Y requests VAD under the NSW Act. His co-ordinating and consulting practitioners are concerned given Mr Y’s history of depression when he reports to them that he has felt there is “no point in living” since he received his cancer diagnosis, and that he wants to join his deceased son
• Mr Y has an MOCA of 26 + 1/30
• Mr Y is referred to a Psychiatrist for opinion under s 38 of the NSW VAD Act by the consulting practitioner. On assessment, Mr Y reports he has continued to experience the same intermittent suicidal ideation for over 40 years, involving fleeting thoughts that “he would be better off dead” but denies any plans to commit suicide. He is able to understand the matters and effect of a VAD decision, weigh up the factors involved, and communicate them. He expresses resentment about his prognosis given his age, which he considers a reflection of how unfair life has been. On further discussion, he reports that he wishes life had turned out differently, including that he had never been diagnosed with cancer, as he would have liked to have spent more time with his family and contributing to his community. He also discusses that given the shock and pain experienced by himself and his family after his son’s sudden death in a car accident many years ago, retaining control over the circumstances in which his life ends has taken on significant importance to him. He reports he is a Christian, has attended church for many years, and has a belief in heaven and that he will see his son there
• His wife and surviving children are supportive of his request
Challenges relating to characteristics of the VAD request – social determinants of health and undue influence
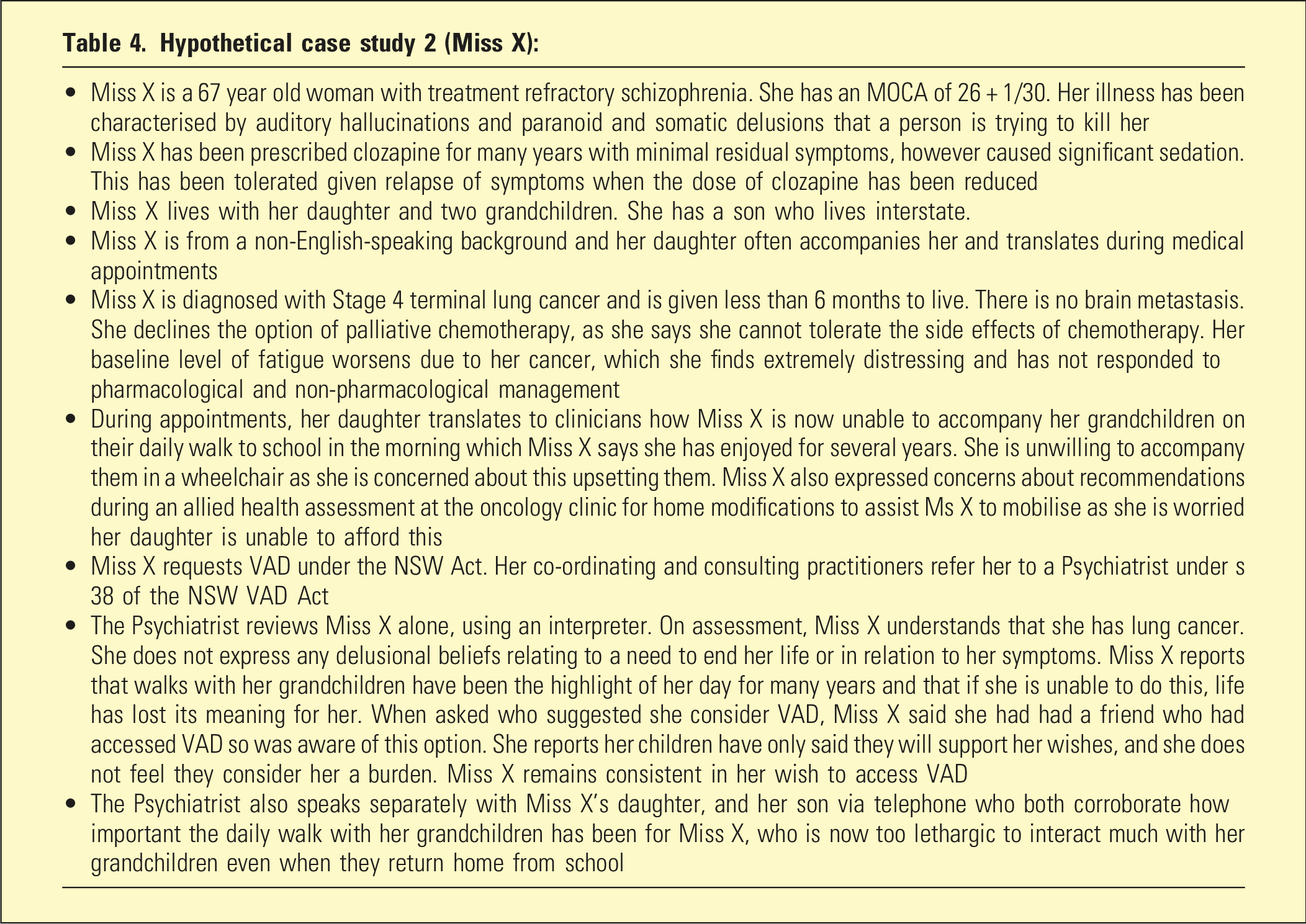
The effect of external factors on the voluntariness of the patient’s VAD request poses another clinical challenge. While undue influence of family members poses one potential avenue,3 the effect of social determinants of health including a person’s living situation should also be considered.20 In the case of Miss X in Table 4, alert to the potential for undue influence given the close involvement of her daughter and reference to financial concerns, the Psychiatrist took care to review Miss X separately from her daughter, using an independent interpreter. Additional collateral was sought from the son. Though there was history of some delusional misattribution of physical symptoms, the patient in this case was aware her physical symptoms were the result of cancer. In Re C indicates the presumption that a patient has capacity to make end of life decisions is not displaced solely by psychiatric evidence regarding presence of delusions. Rather, a direct link needs to be established showing the delusions prevent the patient from sufficiently exercising the required functional ability when making the decision (i.e. understanding, retaining, and weighing information relevant to the decision).
Hypothetical case study 2 (Miss X):
• Miss X is a 67 year old woman with treatment refractory schizophrenia. She has an MOCA of 26 + 1/30. Her illness has been characterised by auditory hallucinations and paranoid and somatic delusions that a person is trying to kill her
• Miss X has been prescribed clozapine for many years with minimal residual symptoms, however caused significant sedation. This has been tolerated given relapse of symptoms when the dose of clozapine has been reduced
• Miss X lives with her daughter and two grandchildren. She has a son who lives interstate.
• Miss X is from a non-English-speaking background and her daughter often accompanies her and translates during medical appointments
• Miss X is diagnosed with Stage 4 terminal lung cancer and is given less than 6 months to live. There is no brain metastasis. She declines the option of palliative chemotherapy, as she says she cannot tolerate the side effects of chemotherapy. Her baseline level of fatigue worsens due to her cancer, which she finds extremely distressing and has not responded to pharmacological and non-pharmacological management
• During appointments, her daughter translates to clinicians how Miss X is now unable to accompany her grandchildren on their daily walk to school in the morning which Miss X says she has enjoyed for several years. She is unwilling to accompany them in a wheelchair as she is concerned about this upsetting them. Miss X also expressed concerns about recommendations during an allied health assessment at the oncology clinic for home modifications to assist Ms X to mobilise as she is worried her daughter is unable to afford this
• Miss X requests VAD under the NSW Act. Her co-ordinating and consulting practitioners refer her to a Psychiatrist under s 38 of the NSW VAD Act
• The Psychiatrist reviews Miss X alone, using an interpreter. On assessment, Miss X understands that she has lung cancer. She does not express any delusional beliefs relating to a need to end her life or in relation to her symptoms. Miss X reports that walks with her grandchildren have been the highlight of her day for many years and that if she is unable to do this, life has lost its meaning for her. When asked who suggested she consider VAD, Miss X said she had had a friend who had accessed VAD so was aware of this option. She reports her children have only said they will support her wishes, and she does not feel they consider her a burden. Miss X remains consistent in her wish to access VAD
• The Psychiatrist also speaks separately with Miss X’s daughter, and her son via telephone who both corroborate how important the daily walk with her grandchildren has been for Miss X, who is now too lethargic to interact much with her grandchildren even when they return home from school
Challenges regarding characteristics of the condition supporting VAD request: mental illness which has caused a medical end-of-life condition
It has been argued the current NSW VAD legislation leaves open the possibility that an application could be made for VAD on the basis of a physical medical condition caused by end-stage sequelae of severe and enduring anorexia nervosa (AN).23 Capacity in patients with AN has long been a fraught issue. It is widely assumed patients with anorexia automatically lack capacity in relation to medical treatment due to the impact of their illness on executive function and delusions relating to weight gain.23 Others argue such an approach is circular and disregards the presumption in favour of capacity and need for individual assessment which focuses on function in decision making, not diagnosis.24 Consideration of factors including societal functioning, emotional state, and mentalisation have also been highlighted.25 While no legal cases in Australia or the UK have found a patient with AN has capacity to make decisions relating to medical treatment of anorexia, there is UK precedent for a person with anorexia being found to have capacity to make decisions in relation to another medical condition (liver failure secondary to alcohol dependency).23 Other contentions in this area include lack of research, clinical guidelines, and staging criteria in relation to severe and enduring AN. This can contribute to barriers accessing end-of-life care compared to patients with other forms of terminal illness.26
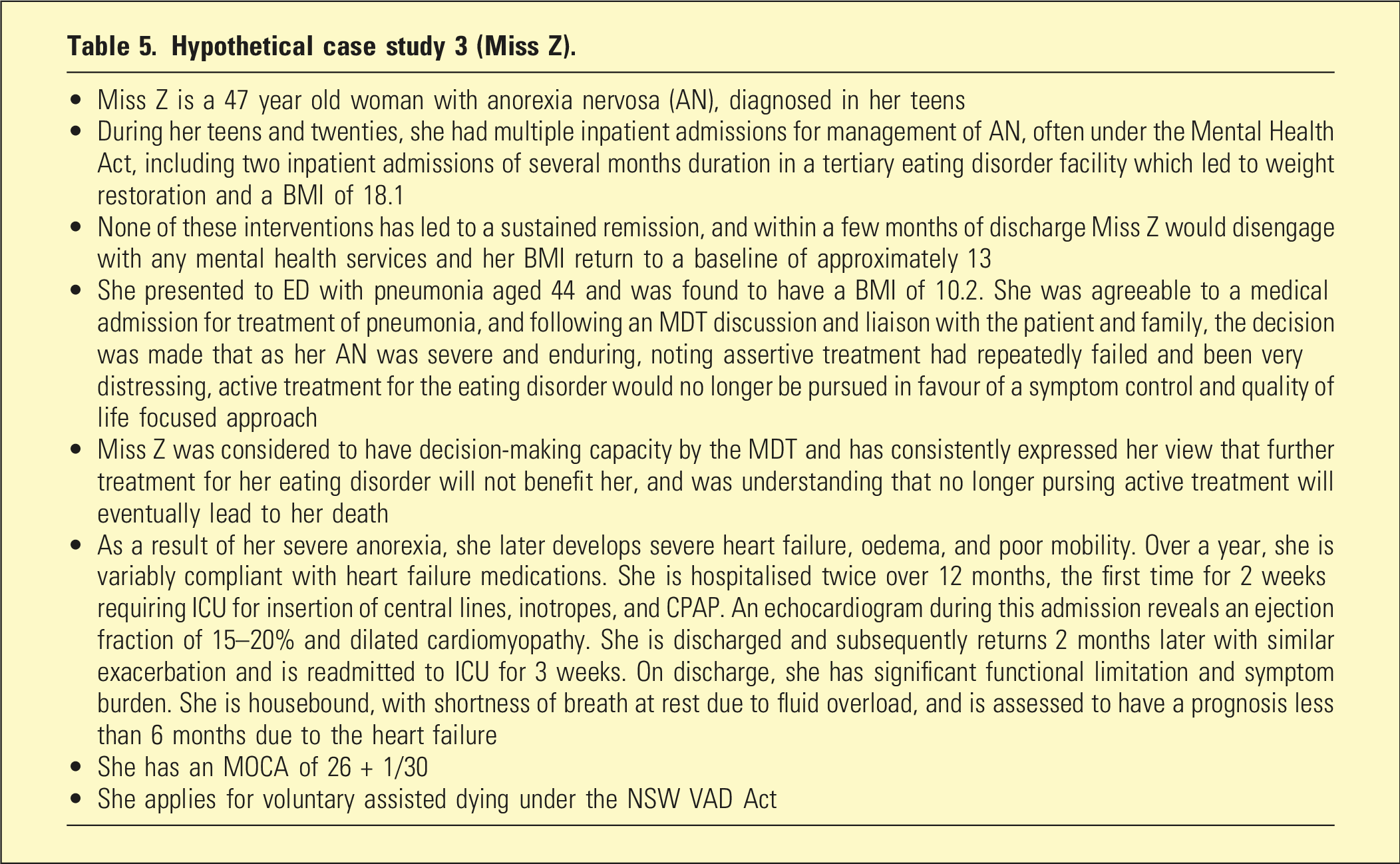
Miss Z in Table 5 represents a hypothetical test case where VAD and end-stage AN could arise. However, the same scholars who raised this possibility acknowledge legal precedent suggests Courts have adopted a holistic view of mental illness and its physical sequelae such that a test case is very unlikely to succeed.23 Regardless, approaches to the case of Miss Z should include referral for confirmation of diagnosis of AN, and separate undertaking of capacity assessment with careful consideration of Miss Z’s personal circumstances, understanding, and subjective reasons underpinning her VAD to identify any deficits in functional decision making and avoid suggestion of a “Catch 22” situation in which capacity is solely or primarily based on her diagnosis of an eating disorder.24 Nevertheless, the heart failure which developed as a result of AN is not likely to be considered a medical condition that is separate from a mental health impairment (anorexia) given it has clearly developed as a result of her severe mental illness.23
Hypothetical case study 3 (Miss Z).
• Miss Z is a 47 year old woman with anorexia nervosa (AN), diagnosed in her teens
• During her teens and twenties, she had multiple inpatient admissions for management of AN, often under the Mental Health Act, including two inpatient admissions of several months duration in a tertiary eating disorder facility which led to weight restoration and a BMI of 18.1
• None of these interventions has led to a sustained remission, and within a few months of discharge Miss Z would disengage with any mental health services and her BMI return to a baseline of approximately 13
• She presented to ED with pneumonia aged 44 and was found to have a BMI of 10.2. She was agreeable to a medical admission for treatment of pneumonia, and following an MDT discussion and liaison with the patient and family, the decision was made that as her AN was severe and enduring, noting assertive treatment had repeatedly failed and been very distressing, active treatment for the eating disorder would no longer be pursued in favour of a symptom control and quality of life focused approach
• Miss Z was considered to have decision-making capacity by the MDT and has consistently expressed her view that further treatment for her eating disorder will not benefit her, and was understanding that no longer pursing active treatment will eventually lead to her death
• As a result of her severe anorexia, she later develops severe heart failure, oedema, and poor mobility. Over a year, she is variably compliant with heart failure medications. She is hospitalised twice over 12 months, the first time for 2 weeks requiring ICU for insertion of central lines, inotropes, and CPAP. An echocardiogram during this admission reveals an ejection fraction of 15–20% and dilated cardiomyopathy. She is discharged and subsequently returns 2 months later with similar exacerbation and is readmitted to ICU for 3 weeks. On discharge, she has significant functional limitation and symptom burden. She is housebound, with shortness of breath at rest due to fluid overload, and is assessed to have a prognosis less than 6 months due to the heart failure
• She has an MOCA of 26 + 1/30
• She applies for voluntary assisted dying under the NSW VAD Act
Discussion
While individual autonomy and self-determination in end-of-life care have been prioritised via legislation of VAD, concerns persist about the State’s obligation to preserve life and for safeguards to protect vulnerable groups like those with mental illness.10–12 Efforts to balance these competing factors, and fundamental concerns to maintain equality of access to medical treatment, are reflected in the principles of the NSW VAD Act and provisions.4 Capacity assessments form the main protection in VAD legislation against people with mental illness inappropriately accessing VAD as a result of symptoms of mental illness.1 These complex assessments involve “a normative judgment in which the freedom to make one’s own decisions is balanced against society’s interest in protecting vulnerable people”(2 p51) over which the Courts have retained ultimate authority1,27 but which in practice are mostly carried out by medical practitioners.2 It is thus essential Psychiatrists familiarise themselves with the relevant VAD requirements in their jurisdiction, noting a contravention of the NSW VAD Act has potential to support a finding of unprofessional conduct or professional misconduct as defined by national professional regulations.4
VAD remains an emerging area of law and medical practice in Australia. However, we suggest that based on existing precedents, Psychiatrists are best placed to meet their obligations under NSW VAD legislation when assessing a patient where there are concerns for mental illness by paying heed to the calls from the Victorian Supreme Court for assessments to be “free of pre-judgment and stereotype” and “criteria focused, evidence based, patient centred and non-judgemental” (17p.66, 78). While these comments were made in an Australian case concerning an appeal of the decision by a State Tribunal to make an involuntary order for Electroconvulsive Therapy (ECT), in Canada Courts have similarly emphasised in relation to medical assistance in dying (equivalent to VAD):
The vulnerability of a person requesting medical assistance in dying must be assessed exclusively on a case-by-case basis, according to the characteristics of the person and not based on a reference group of so-called “vulnerable persons.” Beyond the various factors of vulnerability that physicians are able to objectify or identify, the patient’s ability to understand and to consent is ultimately the decisive factor, in addition to the other legal criteria (21 p. 111).
We propose that a criteria-focused approach to the issue of VAD should ensure the process for making a medical diagnosis, including of a mental illness, is kept rigorously separate from any assessment of capacity, which should be focused on the legal criteria for decision-making capacity as outlined in the VAD legislation.4 It has been noted1 the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) explicitly states that in most situations a clinical diagnosis will not equate to any particular legal standard including in relation to capacity, given the wide variations in impairments seen within a particular mental illness. A non-judgemental approach should ensure that the presumption that all adults have capacity is also the starting point adopted when assessing patients with a mental illness. Additionally, while the presumption that an adult has decision-making capacity is rebuttable with evidence, a criteria and evidence-based approach requires specific consideration of the extent to which a patient meets each of the legal criteria required for capacity to request VAD (whether the way the person functions in making the decision is due to symptoms of a mental illness or not). To document an assessment that a patient with a mental illness lacks capacity to request VAD based only on making a diagnosis of a mental illness, or the mere presence of specific symptoms such as delusions without linking this to the legal criteria for capacity, is likely to be considered an incorrect application of the test in the legislation. An evidence-based and patient-centred approach requires capacity assessments are rigorous and comprehensive, particularly given the significance of the decision to access VAD and known potential for mental illness to impact decision-making capacity.1 For issues of capacity (and undue influence), it may require consideration of collateral information, reflecting the Courts’ emphasis on close attention to each patient’s individual circumstances and values, which in certain cases have preferenced collateral obtained from family over expert medical opinion. Given the complexity of these considerations and the need for a case-by-case approach, Psychiatrists are likely to play an important role providing expertise to reach a consensus-based approach, noting this is also contemplated by the NSW VAD legislation.4
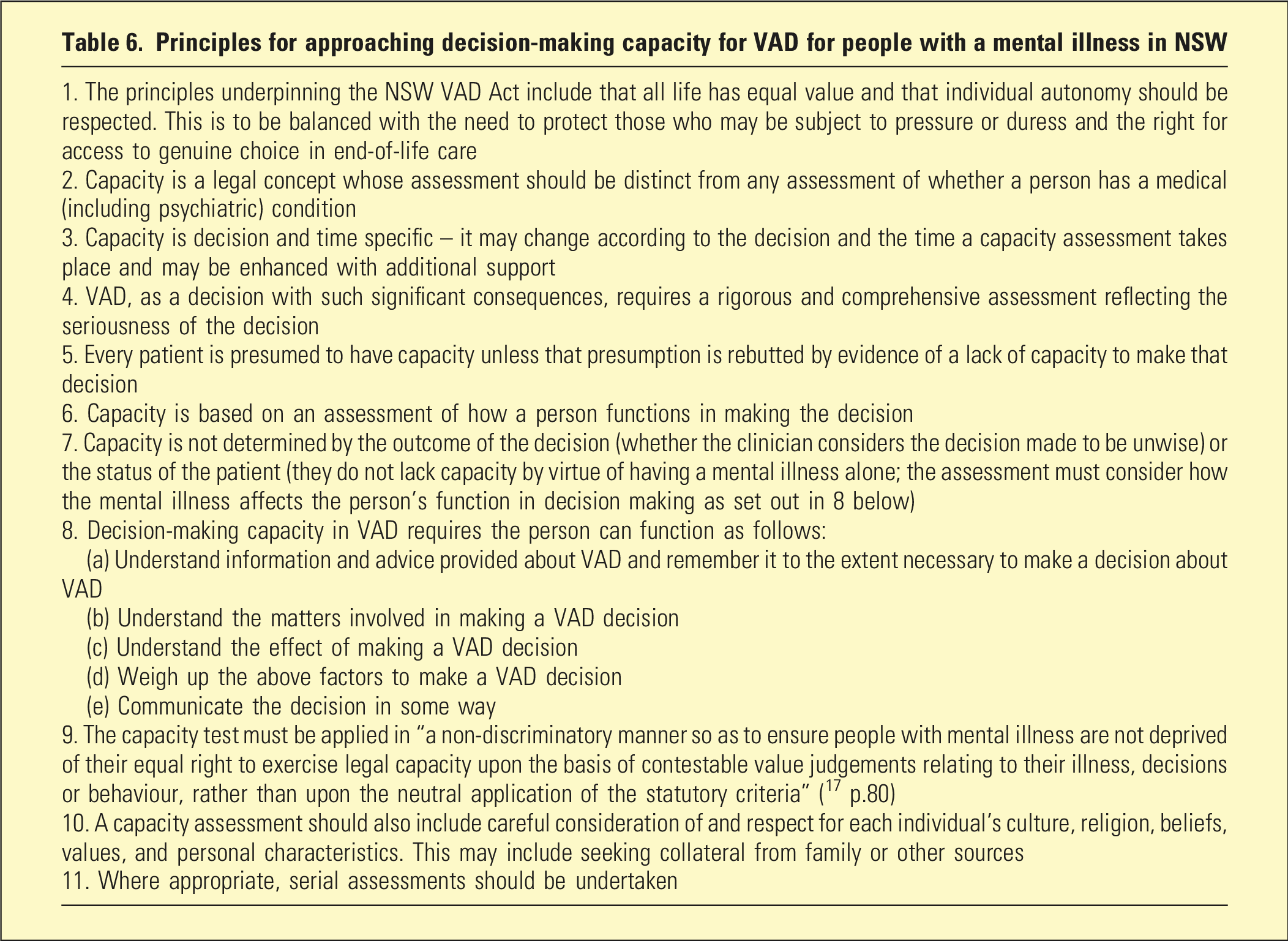
A suggested framework distilling the above principles is contained in Table 6.
Principles for approaching decision-making capacity for VAD for people with a mental illness in NSW
1. The principles underpinning the NSW VAD Act include that all life has equal value and that individual autonomy should be respected. This is to be balanced with the need to protect those who may be subject to pressure or duress and the right for access to genuine choice in end-of-life care
2. Capacity is a legal concept whose assessment should be distinct from any assessment of whether a person has a medical (including psychiatric) condition
3. Capacity is decision and time specific – it may change according to the decision and the time a capacity assessment takes place and may be enhanced with additional support
4. VAD, as a decision with such significant consequences, requires a rigorous and comprehensive assessment reflecting the seriousness of the decision
5. Every patient is presumed to have capacity unless that presumption is rebutted by evidence of a lack of capacity to make that decision
6. Capacity is based on an assessment of how a person functions in making the decision
7. Capacity is not determined by the outcome of the decision (whether the clinician considers the decision made to be unwise) or the status of the patient (they do not lack capacity by virtue of having a mental illness alone; the assessment must consider how the mental illness affects the person’s function in decision making as set out in 8 below)
8. Decision-making capacity in VAD requires the person can function as follows:
(a) Understand information and advice provided about VAD and remember it to the extent necessary to make a decision about VAD
(b) Understand the matters involved in making a VAD decision
(c) Understand the effect of making a VAD decision
(d) Weigh up the above factors to make a VAD decision
(e) Communicate the decision in some way
9. The capacity test must be applied in “a non-discriminatory manner so as to ensure people with mental illness are not deprived of their equal right to exercise legal capacity upon the basis of contestable value judgements relating to their illness, decisions or behaviour, rather than upon the neutral application of the statutory criteria” (17 p.80)
10. A capacity assessment should also include careful consideration of and respect for each individual’s culture, religion, beliefs, values, and personal characteristics. This may include seeking collateral from family or other sources
11. Where appropriate, serial assessments should be undertaken
Conclusion
VAD provides new challenges for Psychiatrists to meet in the evolution of their role in end-of-life care. This role is additionally complicated among vulnerable populations including those with mental illness, though unlike other countries, Australia has adopted a more proscriptive approach requiring any grounds for seeking VAD to be carefully separated from mental illness. While the area is still emerging within Australia, VAD legislation in NSW draws from existing medical and legal practice, particularly regarding capacity assessment, and awareness of potential pitfalls and complexities in these areas can provide a guide for Psychiatrists navigating VAD.
Footnotes
ORCID iD
Sara Alamyar
Ethical considerations
This article does not contain any studies with human or animal participants. There are no human participants in this article, and informed consent and ethical approval are not required.
Author contributions
Duncan George devised the concept of the article (lead) with Sara Alamyar and Linda Sheahan (supporting). Sara Alamyar undertook research (lead) with Linda Sheahan and Duncan George (supporting). Sara Alamyar wrote the original draft of the manuscript as well as edited and drafted revised versions. Duncan George and Linda Sheahan revised and edited several versions of the manuscript and approved the final version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1.
BoyleSMcGeeAWoodF. How to determine the capacity of a person with depression who requests voluntary assisted dying. Psychiatr Psychol Law2024; 32: 1–15. Available at:https://doi.org/10.1080/13218719.2023.2296486
PeisahCSheahanLWhiteBP. Biggest decision of them all – death and assisted dying: capacity assessments and undue influence screening. Intern Med J. 2019; 49(6): 792–796. Available at:https://doi.org/10.1111/imj.14238
GalderisiSAppelbaumPSGillN, et al.Ethical challenges in contemporary psychiatry: an overview and an appraisal of possible strategies and research needs. World Psychiatry. 2024; 23(3): 364–386. Available from:https://doi.org/10.1002/wps.21230
World MedicalAssociation.Policy tag: euthanasia [Internet]. Ferney-Voltaire:World Medical Association, 2022. [cited 24 March 2024]. Available from:https://www.wma.net/policy-tags/euthanasia/
10.
BraunK.Looking back to look forward—the history of VAD laws in Australia and future law reform in the Australian territories. Med Law Rev. 2024; 32(1): 42–60. Available from:https://doi.org/10.1093/medlaw/fwad030
WhiteBCloseEWillmottL, et al.Comparative and critical analysis of key eligibility criteria for voluntary assisted dying under five legal frameworks. UNSW Law Journal. 2021; 44(4): 1663–1700. Available from:https://doi.org/10.53637/JUWL9208
13.
HolmesALangePCameronS, et al.Can depressed patients make a decision to request voluntary assisted dying?Intern Med J.2021; 51(10): 1713–1716, Available at:https://eprints.qut.edu.au/226586/
14.
TrachselMJoxRJ. Suffering is not enough: assisted dying for people with mental illness. Bioethics. 2022; 36(5): 519–524. Available from:https://doi.org/10.1111/bioe.13002
15.
ShawDTrachselMElgerB. Assessment of decision-making capacity in patients requesting assisted suicide. The British journal of psychiatry: The Journal of Mental Science. 2018; 213(1): 393–395. Available from:https://doi.org/10.1192/bjp.2018.81
WhiteBPWillmottLDel VillarK, et al.Who is eligible for Voluntary Assisted Dying: Nine medical conditions assessed against five legal frameworks. University of New South Wales Law Journal.2022; 45(1): 401-444, , at 421. Available from:https://doi.org/10.53637/fyid9182
ElzakkersIFDannerUNHoekHW, et al.Mental capacity to consent to treatment in anorexia nervosa: explorative study. BJPsych open. 2016; 2(2): 147–153. Available from:https://doi.org/10.1192/bjpo.bp.115.002485
26.
GaudianiJLBogetzAYagerJ. Terminal anorexia nervosa: three cases and proposed clinical characteristics. J Eat Disord. 2022; 10(1): 23–37. Available from:https://doi.org/10.1186/s40337-022-00548-3